Article Text

Abstract
Background Chronic obstructive pulmonary disease (COPD) is a chronic disease associated with recurring exacerbations, which influence morbidity and mortality for the patient, while placing significant resource burdens on healthcare systems. Non-invasive ventilation (NIV) in a domiciliary setting can help prevent admissions, but the economic evidence to support NIV use is limited.
Methods A Markov model-based cost-utility analysis from the UK National Health Service perspective compared the cost-effectiveness of domiciliary NIV with usual care for two end-stage COPD populations; a stable COPD population commencing treatment with no recent hospital admission; and a posthospital population starting treatment following admission to hospital for an exacerbation. Hospitalisation rates in patients receiving domiciliary NIV compared with usual care were derived from randomised controlled studies in a recent systematic review. Other model parameters were updated with recent evidence.
Results At the threshold of £20 000 per quality-adjusted life-year (QALY) domiciliary NIV is 99.9% likely cost-effective in a posthospital population, but unlikely (4%) to be cost-effective in stable populations. The incremental cost-effective ratio (ICER) was £11 318/QALY gained in the posthospital population and £27 380/QALY gained in the stable population. Cost-effectiveness estimates were sensitive to longer-term readmission and mortality risks, and duration of benefit from NIV. Indeed, for stable Global Initiative for Chronic Obstructive Lung Disease (GOLD) for stage 4 patients, or with higher mortality and exacerbation risks, ICERs were close to the £20 000/QALY threshold.
Conclusion Domiciliary NIV is likely cost-effective for posthospitalised patients, with uncertainty around the cost-effectiveness of domiciliary NIV in stable patients with COPD on which further research should focus.
- non invasive ventilation
- COPD epidemiology
- COPD exacerbations
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Taking into account recently published evidence on effectiveness, what is the longer-term cost-effectiveness of domiciliary non-invasive ventilation (NIV) in posthospitalised and stable patients.
What is the bottom line?
Health economic decision modelling found that domiciliary NIV is highly, likely to be cost-effective in posthospitalised patients, but unlikely to be cost-effective in stable patients, compared with usual care.
Why read on?
Currently, there is uncertainty surrounding the effectiveness and cost-effectiveness of domiciliary NIV, and commissioning of this intervention varies across and within countries (including the UK). This paper reports an updated model-based analysis of the cost-effectiveness of domiciliary NIV for end stage COPD, incorporating new effectiveness evidence.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive lung disease often accompanied by recurring exacerbations, that lead to clinical deterioration, and when severe, require hospitalisation.1 When comparing non-invasive ventilation (NIV) with either no ventilation or invasive mechanical ventilation in hospital settings, in the context of type two respiratory failure/acute hypercapnic respiratory failure (AHRF), but not the absence of type 2 respiratory failure (T2RF), various study designs have consistently shown better outcomes for NIV in the form of reduced inpatient mortality and length of stay.2–6
NIV may also be administered at home with or without oxygen therapy. Based on randomised controlled trials (RCTs), a previous systematic review7 found no evidence for a survival benefit and limited evidence for fewer hospitalisations in stable populations. A survival benefit was also not demonstrated for posthospitalised patients (those recently discharged from admission to hospital for an exacerbation) with inconsistent findings on hospital readmissions.
We have previously demonstrated in a model-based cost-effectiveness analysis considerable uncertainty regarding cost-effectiveness of domiciliary NIV for both stable and posthospital patients.7 The analysis was sensitive to assumptions regarding the strength and duration of treatment effect. As a consequence of the uncertainty over evidence, commissioning of domiciliary NIV varies across and within countries (including the UK), and a robust model could aid formation of national guidance and streamline processes surrounding this treatment in the UK.
There is growing evidence relating to the effectiveness of domiciliary NIV in COPD.1 This paper reports an analysis of the cost-effectiveness of domiciliary NIV for end-stage COPD updating our previously published model7 with estimates of clinical effectiveness including recent and previously missed evidence.8 Other model parameters are updated using real-life COPD data from the UK, including the National COPD audit9 and Clinical Practice Research datalink,10 which provide robust UK baselines of COPD outcomes for an untreated population.
Methods
Two cost-utility analyses were undertaken comparing domiciliary NIV with usual care for two COPD populations:
Patients starting domiciliary NIV in a stable state, where they had no recent exacerbations, hospital admissions or other major change in clinical parameters over a defined period (4 or more weeks).7
Patients starting domiciliary NIV immediately following admission to hospital for an exacerbation.
A Markov cohort model was constructed in TreeAge Pro (TreeAge Software, 2019) to estimate quality-adjusted life years (QALYs) and costs from the UK National Health Service (NHS) perspective. A 10-year time horizon was selected owing to high mortality in this patient population, with monthly time cycles. QALYs and costs were discounted at 3.5% as per UK guidance11 with half-cycle correction performed. Model results are predicated on the benefit of NIV being accrued via a reduced risk of hospitalisation and associated cost-savings, life years gained and utility improvements.
Model population
The stable model population was reflective of stable patients included in RCTs from the clinical effectiveness systematic review.8 The mean age was 67, 54% were female, and 52% smokers (online supplemental appendix 1). Distribution between 2011 GOLD stages was not commonly reported, therefore an assumption was made that 50% were in Global Initiative for Chronic Obstructive Lung Disease (GOLD) severity stage 3% and 50% in stage 4, and domiciliary NIV would not be required in earlier disease stages, or where significant comorbid disease contributed to the underlying respiratory failure. COPD stage was defined according to 2011 GOLD classifications; GOLD stage 3 had a predicted forced expiratory volume in one second (FEV1)≥30%, <50% and GOLD stage 4 a predicted FEV1≤30%. As real-world information was available for posthospital patients, the model population was reflective of patients in the 2017 National UK COPD audit,9 mean age 73, 47% female, 31% smokers, with an assumed 50% in GOLD stage 3 and 4 (online supplemental appendix 1). Online supplemental appendix 2 details all model assumptions.
Supplemental material
Model structure
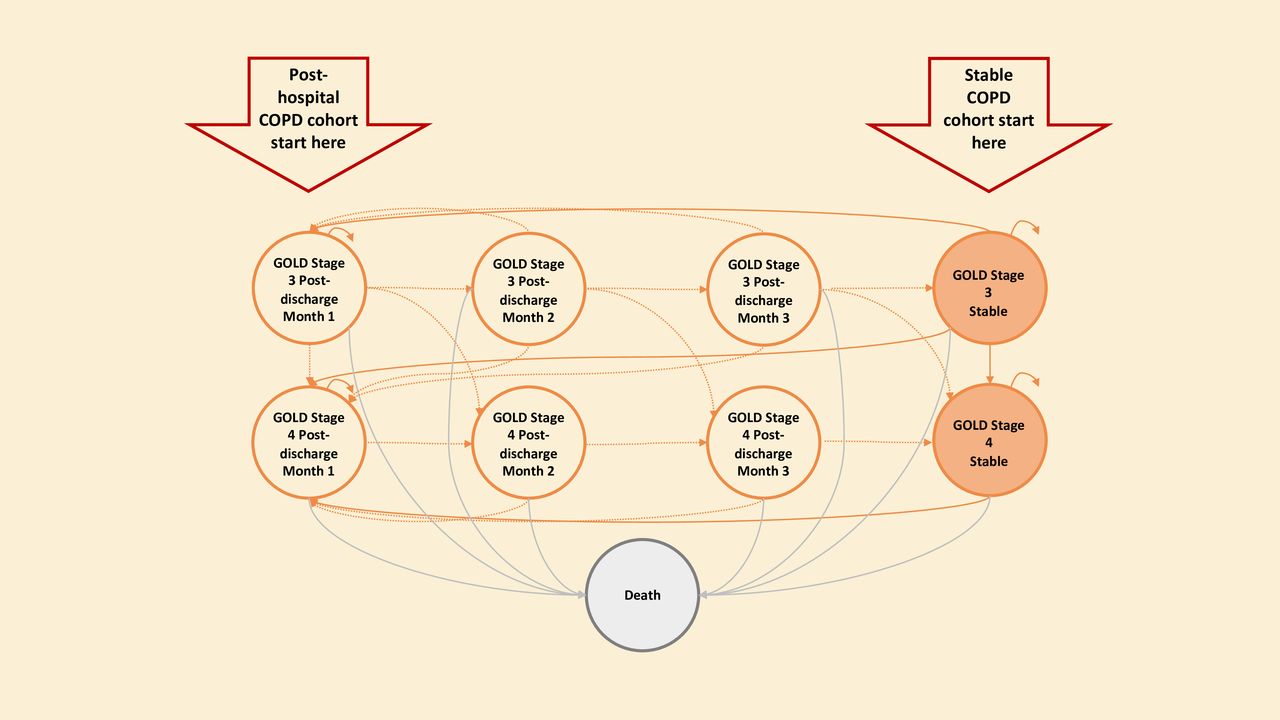
Figure 1, adapted from Dretzke et al,7 shows the model composition. The same structure was used for both populations, although posthospitalised patients started in ‘postdischarge month 1’, while stable patients began in stable states. The model used tunnel states to represent increased risk of mortality and readmission, lower quality of life, and higher costs, in those discharged after admission for an exacerbation. Accordingly, patients could not remain in postdischarge states by definition. Posthospitalised patients moved to stable health states after the postdischarge period, and stable patients moved to a posthospital state if they experienced an exacerbation requiring hospitalisation. There was a differing mortality risk in each state, according to population and health state. Patients could transition from GOLD stage 3–4, although not 4–3 as the disease is progressive. Online supplemental appendix 3 provides further detail.

State-transition schematic. GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Model parameter estimates
Table 1 presents the model parameters for hospitalisation, mortality and discontinuation.
Hospitalisation, mortality and discontinuation parameters
Hospitalisation and mortality in postadmission health states
Transition probabilities for mortality and readmission for postdischarge states in both populations were obtained from the most recent UK audit of patients with COPD admitted to hospital.9 Risk of readmission and mortality were assumed (1) to be evenly distributed over the 3-month period, and (2) to not to differ by GOLD stage as there is no evidence on a differentiated risk.7
Hospitalisation and mortality risks for the posthospital population
Beyond the postdischarge period for the posthospitalised population, there was greater uncertainty regarding admission rates and mortality. Four studies12–15 were identified which reported long-term admission rates and mortality. Highest and lowest rates were used in sensitivity analyses, with mid-range rates used for the base case.
COPD-related mortality was captured via the risk of a COPD-related death either during admission or in the 3-month postdischarge period.9 These risks in combination with the all-cause mortality risk reported in Garcia-Aymerich et al 12 were assumed to stay constant over the cohort lifetime.
Exacerbation and hospitalisation risk in stable health states
For the stable population, data on exacerbation and hospital admissions in the stable health states were drawn from a large UK study (n=12 830) with long-term follow-up of a COPD general practice population.9
Mortality risks for the stable population
For health states for the stable population, Office for National Statistics life tables were used to populate age and gender-specific all-cause mortality probabilities, adjusted to avoid double counting of COPD-related mortality (online supplemental appendix 4).
Discontinuation rate
After an initial period, it was assumed a proportion of patients starting domiciliary NIV would discontinue treatment. Non-adherence and discontinuation rates vary across both populations,8 therefore it was assumed that 15% of patients would discontinue after 3 months. Patients who discontinued NIV were assumed to incur costs but not benefits of NIV in the initial 3 months, and neither costs nor benefits of NIV beyond 3 months.
Disease progression in stable and posthospital population
Baseline risks of hospital admission and mortality need to be extrapolated beyond the follow-up duration in source studies. Accordingly, to capture long-term prognosis, patients were allowed to move between GOLD stages. Probabilities associated with moving to GOLD stage 4 were sourced from a previously published model16 and applied to GOLD stage 3 states for both populations (online supplemental appendix 5).
Effectiveness of domiciliary NIV
Hospital admission data were taken from our meta-analysis of absolute differences8 and converted to rate ratios by estimating the number of events and total time at risk (assuming complete follow-up) from relevant RCTs. The rate ratio and SE were calculated using Poisson regression, rate ratios with 95% CIs (table 1).
The base case analysis considered all studies in the review; however, to account for differences between healthcare systems, a sensitivity analysis was also performed on studies in Western/high-income settings. Further sensitivity analyses used individual studies with the best-case and worst-case rate ratios for the effect of NIV on hospital admissions.
Given that hospital admission is associated with increased mortality risk, the model produces an improvement in mortality for NIV indirectly by preventing admissions. To assess external validity, the extent to which the model reflects the real-world, model survival rates were contrasted with those found in the RCTs in the clinical effectiveness systematic review.8
Following consultation with clinicians involved with treating patients with NIV, it was assumed that the effect of NIV in reducing admissions would last 5 years in both patient groups, with alternative periods of efficacy tested in sensitivity analysis.
Utility values
Utility values were obtained for each stable GOLD stage 3 and 4 from EQ-5D-5L (the five level EuroQol five dimensions) values for 336 participants with a confirmed diagnosis of COPD from a UK cohort study,17 table 2. No effect on quality of life is assumed above that of the impact NIV has on exacerbations and mortality, this assumption is tested in sensitivity analyses.
Utility scores and costs for stable GOLD states, and costs of providing a domiciliary NIV service
In line with previous COPD models,18–20 disutility values associated with moderate or severe exacerbation were taken from Rutten-van Mölken et al.21 A disutility of 15% for a moderate exacerbation was assigned for a period of 1 month, with a 50% loss in the first month of a severe exacerbation and a 25% loss in second and third months.
Costs
Costs were presented in 2019/2020 pounds sterling and inflated to current value using hospital and community health services index and NHS cost inflation index.22 Costs were subdivided into three components, (1) routine COPD care, (2) treatment of exacerbations, and (3) provision of domiciliary NIV.
All detailed cost calculations for each component can be found in online supplemental appendix 7, with table 2 providing headline costs, as well as the methodology for estimating the cost of providing domiciliary NIV, estimated at £1698.18 in the first year and £1086 in subsequent years (further details in online supplemental appendix 7).
Analyses
A cost-utility analysis was undertaken to estimate incremental cost-effectiveness ratios (ICERs), the difference in costs divided by the difference in QALYs of two strategies, with results presented as cost-per-QALY gained. Cost-effectiveness was considered in relation to the lower NICE threshold of £20 000 per-QALY gained.23 Each result reflects mean costs and QALYs as an average of 10 000 model iterations generated by probabilistic sensitivity analysis, used to account for parameter uncertainty. Where possible, distributions were attached to probabilities, utilities and costs in the model. Beta distributions were attached to transition probabilities and utilities, with natural logs of rate ratios sampled normally and exponentiated.24 The model results were expressed as a cost-effectiveness acceptability curve (CEAC) showing graphically the probability of cost-effectiveness of domiciliary NIV across a range of cost-per-QALY thresholds.24 Deterministic sensitivity analyses were used to assess the individual impact of varying model parameters on cost-effectiveness results.
Expected value of perfect information (EVPI)
EVPI is a quantitative method of assessing the marginal value of further studies, and in essence helps consider whether it is worth conducting more research.25 In order to calculate the population EVPI the size of population expected to benefit must be calculated. We estimated this to be 661 199 for stable patients and 190 049 for posthospital patients over a 10-year time horizon (calculations in online supplemental appendix 8).
Results
Posthospital population
Base case for the posthospital population
In the base case analysis for the posthospital population domiciliary NIV was £4799 more costly, delivering 0.424 more QALYs, making the ICER £11 318/QALY gained. This was 99.9% likely to be cost-effective at the £20 000/QALY threshold (table 3).
Base case analyses posthospital population
Using hospitalisation rates from Western studies, QALY gains reduced to 0.168 for £4765 additional cost, increasing the ICER to £28 430/QALY with domiciliary NIV only 46.9% likely to be cost-effective.
The base case cost-effectiveness plane in figure 2 shows NIV is more effective and costly in all model iterations (hence all iterations in the north-east quadrant). The corresponding CEAC (figure 3) demonstrates domiciliary NIV is very likely to be cost-effective over thresholds of about £12 500/QALY and is always cost-effective between £20 000/QALY and £30 000/QALY.
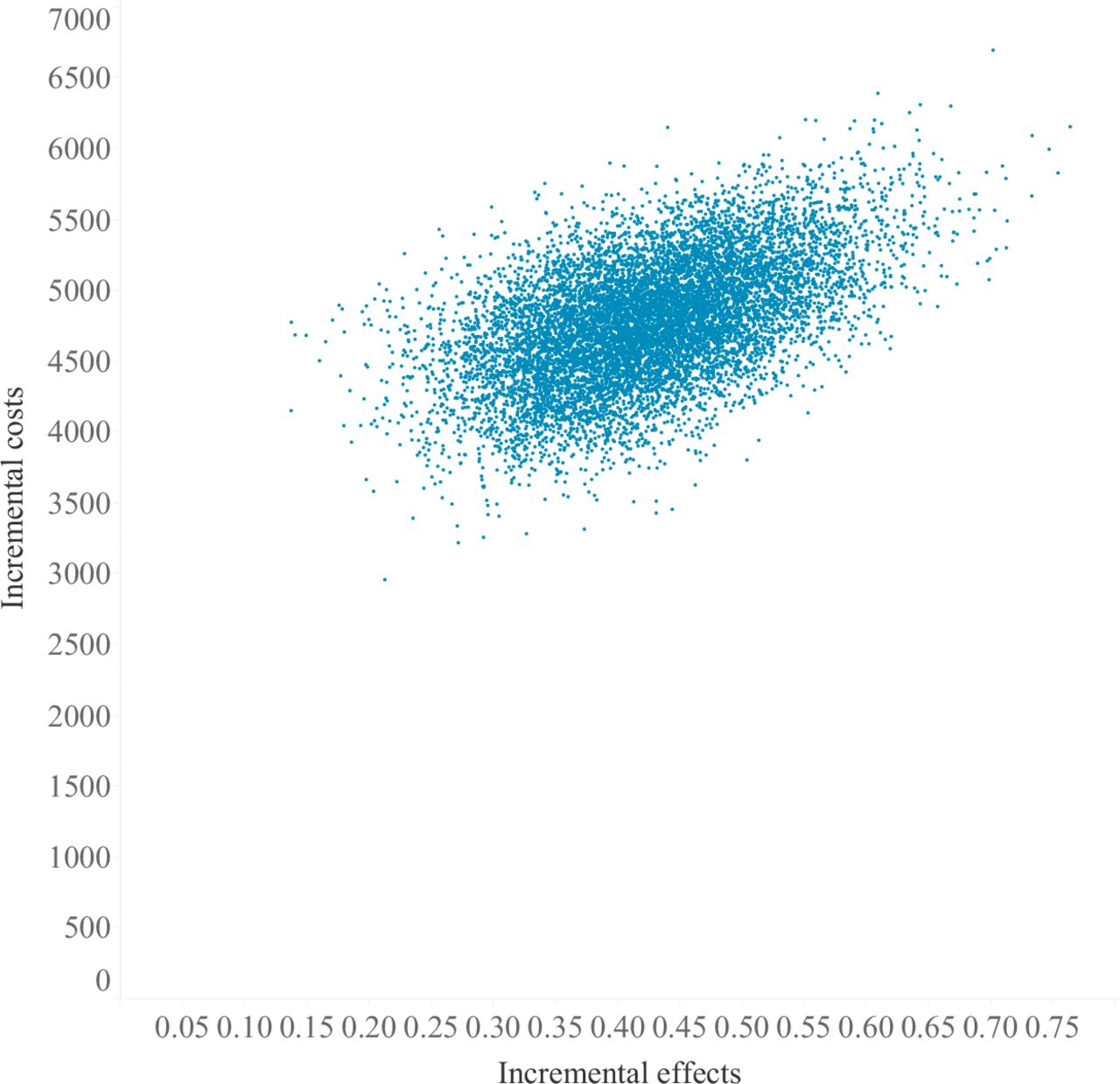
Base case cost-effectiveness plane for domiciliary NIV for posthospitalised patients. Incremental costs and effectiveness reflect the sum of mean costs and quality-adjusted life years (QALYs) of domiciliary non-invasive ventilation (NIV) minus those of usual care. Results are generated from probabilistic sensitivity analysis, where 10 000 unique Monte Carlo simulations sample from the known distributions of model parameters. Accordingly, each dot reflects the incremental costs and QALYs for each one of the 10 000 model iterations. Notice, all dots lie above 0 for incremental effectiveness indicating NIV is more effective, and all points above 0 for incremental costs indicating NIV is more expensive. The size of the cloud of dots reflect the range of incremental costs and QALYs that the model results could take, given the uncertainty in the model parameters.
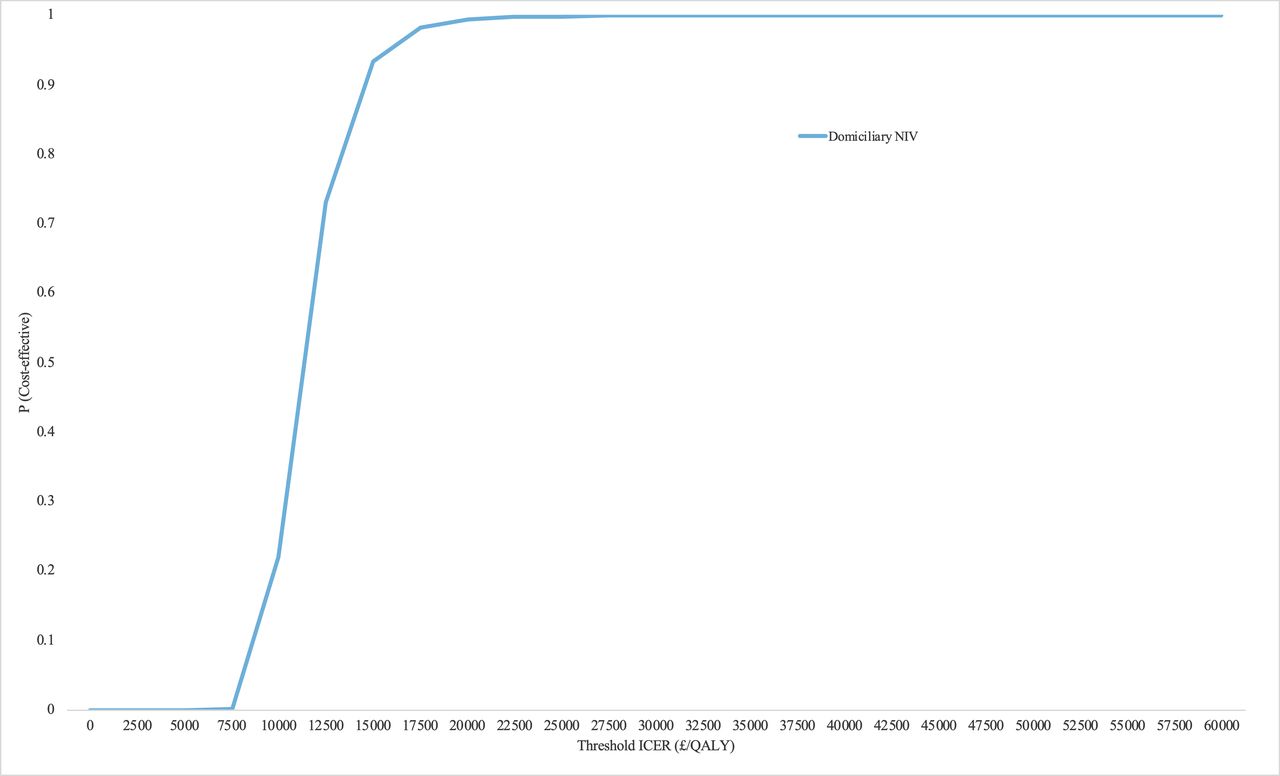
Base case cost-effectiveness acceptability curve. The graph plots the probability that domiciliary NIV is cost-effective at various UK thresholds for willingness to pay for 1 QALY (£/QALY). Between the commonly used UK thresholds of £20 000 to £30 000 per QALY, it can be seen NIV is consistently 99%–100% likely to be cost-effective. ICER, incremental cost-effectiveness ratio; NIV, non-invasive ventilation; P, probability; QALY, quality-adjusted life year.
Sensitivity analysis
Table 4 shows the impact of alternate parameter values on cost-effectiveness in posthospital patients. Applying the rate ratio for hospital admissions from the worst-case study results in NIV being dominated, that is both more costly with worse health outcomes in all study settings. Assuming the duration of effect of domiciliary NIV in reducing hospital admissions is only 2 years, gives a higher ICER of £22 078/QALY, with likely cost-effectiveness reduced to 26%. However, it would take a 0.10 reduction in utility on NIV to significantly impact the likely cost-effectiveness, resulting in an ICER of £35 526/QALY and only 5% likely to be cost-effective.
One-way sensitivity analysis in the posthospital population
Changing baseline hospitalisation and mortality data to lower estimates14 increased the ICER to £21 473/QALY and reduced the probability of NIV being cost-effective to 39%. However, increasing all mortality risks by a factor of two decreased costs and outcomes owing to shorter survival, reducing the ICER to £9883/QALY.
Varying the time horizon did not impact cost-effectiveness significantly, neither did analyses on various machine costs, lifespans, maintenance cost of NIV (online supplemental appendix 9) or different population subgroups (online supplemental appendix 10).
In terms of model validity, base case estimated mortality at 2 years was 43.5% on usual care and 36% on NIV, this is similar to an RCT which reported 2-year mortality at 40% in posthospitalised patients receiving NIV.26 Moreover, the relative risk of mortality on NIV compared with usual care of 0.83 is statistically similar to the relative risk of mortality for the posthospitalised population found in RCTs in the systematic review 0.78 (0.60–1.03).8
EVPI for the posthospital population
The EVPI for the posthospital population was estimated to be £3.25 per patient, reflecting low uncertainty in the base case analysis at a threshold of £20 000/QALY. The estimated population EVPI over the next 10 years was estimated at £617 659.
Stable population
Base case
In the base case analysis for the stable population, domiciliary NIV was £8488 more costly but gave 0.310 additional QALYs, for an ICER of £27 380/QALY, only 4% likely to be cost-effective at the £20 000/QALY threshold (table 5). Using a rate ratio estimate from ‘Western’ settings, saw a smaller QALY gain of 0.14 for £8400 additional cost, increasing the ICER to £60 000/QALY. The likely cost-effectiveness was 25% due to uncertainty in the effectiveness estimate.
Base case analyses stable population
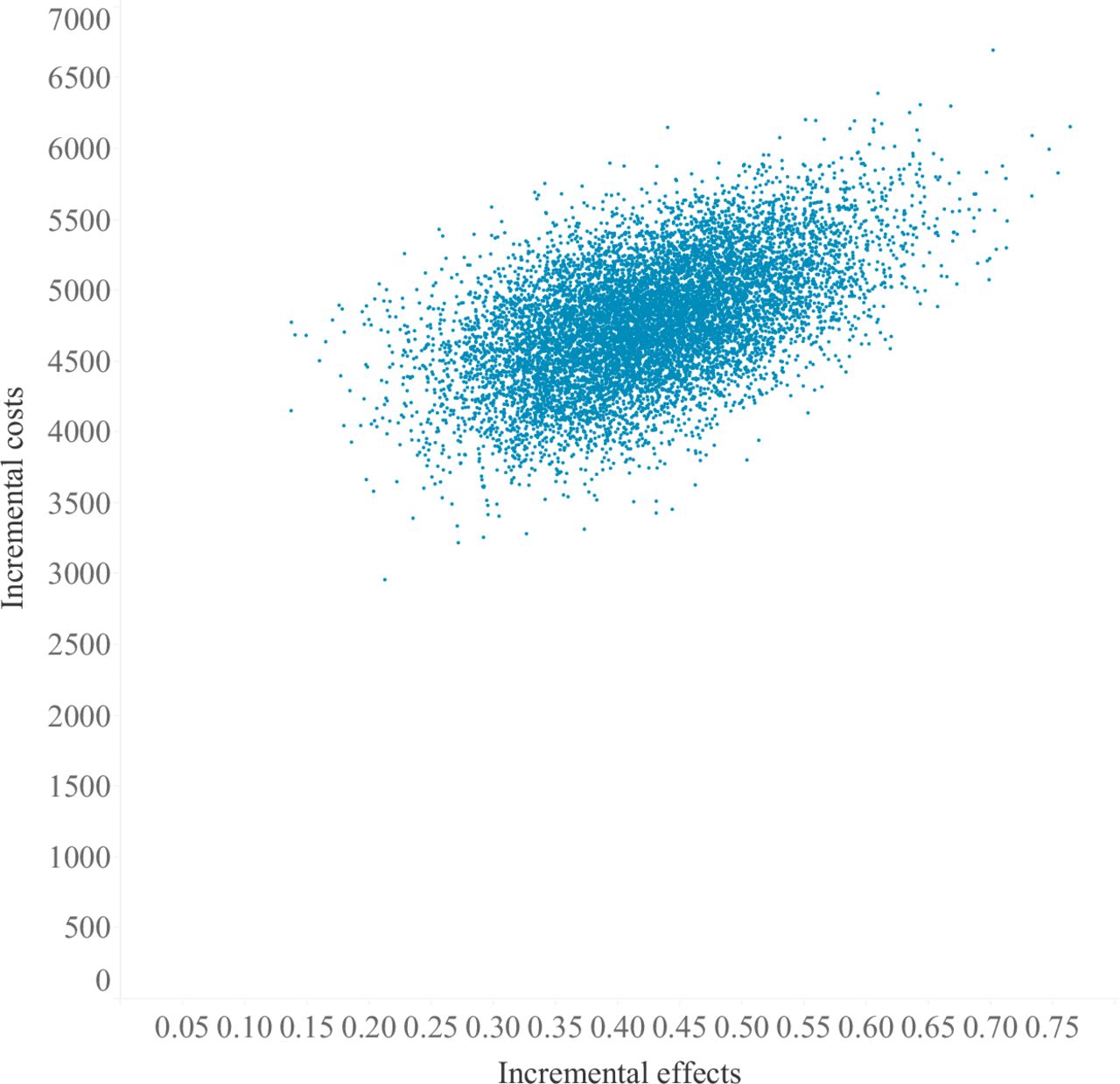
The base case cost-effectiveness plane (figure 4) shows NIV was more effective and costly in most model iterations. The corresponding CEAC (figure 5) demonstrates QALY increases come at a high cost, with domiciliary NIV only likely to be cost-effective over thresholds of £40 000/QALY.

Base case cost-effectiveness plane for domiciliary NIV for stable patients. Incremental costs and effectiveness reflect mean the sum of mean costs and quality-adjusted life years (QALYs) of domiciliary non-invasive ventilation (NIV) minus those of usual care. Results are generated from probabilistic sensitivity analysis, where 10 000 unique Monte Carlo simulations sample from the known distributions of model parameters. Accordingly, each dot reflects the incremental costs and QALYs for each one of the 10 000 model iterations. Notice, all dots lie above 0 for incremental effectiveness indicating NIV is more effective, and all points above 0 for incremental costs indicating NIV is more expensive. The size of the cloud of dots reflect the range of incremental costs and QALYs that the model results could take, given the uncertainty in the model parameters.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Base case cost-effectiveness acceptability curve. The graph plots the probability that domiciliary NIV is cost-effective at various UK thresholds for willingness to pay for 1 QALY (£/QALY). Above thresholds of £40 000 per QALY, it can be seen NIV emerges as likely to be cost-effective. ICER, incremental cost-effectiveness ratio; NIV, non-invasive ventilation; P, probability; QALY, quality-adjusted life years.
Sensitivity analyses
Table 6 shows sensitivity analyses for stable patients. When using alternate rate ratios, NIV is almost certain to be cost-effective at £20 000/QALY in the best case all studies estimate, whereas the best-case Western study only gives an ICER of £31 196/QALY. Cost-effectiveness was very sensitive to changes in utility, with a +0.05 gain in utility on NIV reducing the ICER to below £20 000/QALY. While assuming the effect of NIV lasted for a 10-year time horizon also reduced the ICER to £19 119/QALY.
One-way sensitivity analysis for stable population
Domiciliary NIV is more cost-effective in patients with higher baseline hospitalisation and mortality risks. Higher baseline hospitalisation and mortality risks12 reduced the ICER to £20 797/QALY, increasing the probability of NIV being cost-effective to 44%.
Sensitivity analyses on alternative machine cost, lifespan and annual NIV maintenance cost did not influence cost-effectiveness (online supplemental appendix 9).
Choice of GOLD stage starting cohort also influenced the likely cost-effectiveness, the ICER fell to £21 132/QALY with a 43% probability of being cost-effective when only GOLD stage 4 patients were considered. Results for other subgroups were similar to the base case (online supplemental appendix 10).
EVPI analysis for the stable population
The EVPI per patient for the posthospital population was estimated to be £18.01 per patient and over the next 10 years generated population EVPI of £11 908 194.
Discussion
This updated and enhanced economic model for domiciliary NIV in severe patients with COPD provides evidence on the likely cost-effectiveness of domiciliary NIV in a posthospital population. The high likelihood of cost-effectiveness in the posthospitalised population is driven by favourable new evidence on hospital admissions from recently published RCTs, and those conducted in China not included in previous systematic reviews.8 However, caution is required for generalisation to the UK, as the likely cost-effectiveness is below 50% when applying estimates of NIV effect from ‘Western’ studies. While NIV for those with more stable disease is unlikely to be cost-effective, the ICER for stable patients in GOLD stage 4 and with higher exacerbation risks was only just over the £20 000/QALY threshold.
Are there settings in which domiciliary NIV is more cost-effective?
Cost-effectiveness and clinical effectiveness are related, in that groups with the most clinical benefit will usually incur lower costs, and this is the case with domiciliary NIV. Analyses on admissions and mortality risks demonstrated that posthospitalised patients, who have inherently higher admission and mortality risks, are more likely to benefit from domiciliary NIV.
The rate ratio in posthospitalised populations in ‘Western’ settings, derived from fewer studies, was also higher than the all-studies estimate and lowered the likely cost-effectiveness somewhat, suggesting other factors might be influencing outcomes independently of NIV in ‘Western’ settings. Assuming that NIV only impacts hospital admissions for a duration of 2 years also raises the ICER over the £20 000/QALY threshold. Long-term registry-based studies of domiciliary NIV might assist in generating the data to estimate how long the true effect lasts.
Domiciliary NIV for stable populations is not likely to be cost-effective at the £20 000/QALY threshold. However, there is evidence that patients with a higher risk of mortality and admission are more likely to benefit from domiciliary NIV, and it remains possible that stable populations such as those with a high blood CO2 level27 would benefit more. However, sensitivity analyses based on severe hypercapnia, or change in hypercapnia with treatment, were not possible because of poor reporting, and a lack of studies targeting appropriate patients.
How certain are the results?
The probability of cost-effectiveness in posthospital populations is close to 100% at the £20 000 per QALY threshold; however, there is more uncertainty in stable patients. Cost-effectiveness of NIV in the posthospital population is higher (99.9%) than in our original model (72%) reflecting reduced uncertainty. However, the ICER is actually higher (£11 318/QALY vs £10 107/QALY) as the time horizon and NIV effect duration were lowered to 10 years and 5 years, respectively, reflecting greater knowledge of long-term outcomes. The result in the stable population is sensitive to assumptions, for example, applying an increase in utility of 0.05 on NIV lowers the ICER below the £20 000/QALY threshold, and using the best-case rate ratio estimate results in the intervention being close to 100% cost-effective at the £20 000/QALY threshold.
What studies should be done next?
One of the limitations of our study concerns the pooling of data from potentially heterogenous patients with COPD, and clearly given the sensitivity to variation in clinical risk there could be real value in exploring the effect of NIV in these subgroups. In particular, the estimate for the value of further research in the stable population is substantial, reflecting the sizeable population expected to benefit. However, uncertainty regarding mortality and readmission rates, which are shown to influence cost-effectiveness in both populations, is not parameterised in this model (and therefore excluded from the EVPI) owing to the lack of consistency, and ought to be a target for further research. More nuanced studies enrolling subgroups of patients with COPD in the stable state, for example, studies targeting specific subgroups within a stable population, for example, severely hypercapnic patients (eg, pCO2>7.5 kPa), and studies using higher pressure settings28 and longer-term follow-up could reduce uncertainty in future cost-effectiveness evaluations. Moreover, research will be required to understand the long-term impact of the COVID-19 pandemic on patient with COPD outcomes and treatment patterns, and may require updated modelling to reflect the new normal.
Strengths and limitations
Key strengths of this analysis derive from the original model design, which considers stable and posthospital patients with COPD separately, allowing for appropriate risk estimates for each population. Moreover, the utilisation of postadmission health states allows higher risks of readmission and mortality in patients with COPD immediately after discharge. Results are strengthened by the updating of model parameters using recently published data.
Moreover, the use of more robust assessment of clinical effectiveness evidence has decreased the uncertainty regarding the treatment effect of NIV (hospital admissions) in posthospital patients. This has arisen from the incorporation of a large number of additional studies and the decision to use a pooled effect estimate, despite some evidence of heterogeneity. This was felt to be a reasonable decision in this case as the direction of effect was consistent (bar one study), unlike the original analysis which was limited to three studies with substantial uncertainty around direction of effect. The degree of uncertainty regarding the pooled estimate in the stable population has also been reduced, driven by the inclusion of previously unidentified studies conducted in China. The inclusion of evidence from studies conducted world-wide strengthens the overall cost-effectiveness findings, although the generalisability of these findings to different healthcare settings needs further evaluation.
However, the analyses cannot overcome uncertainties in parameters, in particular for the longer-term risks where there is only limited evidence. Nonetheless, this analysis provided extensive sensitivity analyses to illuminate the implications of this uncertainty wherever possible.
It is possible our dichotomisation of stable and posthospital patients reflects more the pathway by which hypercapnia is identified than different populations, further research is required. Importantly, patients with COPD are mainly monitored for respiratory failure using oxygen saturations, and rarely blood gases, when stable. This may lead to late identification of stable hypercapnia, whereby it is only deterioration with resultant acidosis and hospital admission that leads to blood gas being taken during admission and at follow-up. Research to date to identify factors predicting hypercapnia has been unable to identify accurately all those who might require blood gas testing, but those with severe disease and with a prior admission (even if not requiring NIV) may be an important group.29 Alternatively, they may be truly different due to medical optimisation while admitted, or other as yet unknown factors.
Conclusion
Domiciliary NIV appears to be cost-effective when started immediately after or within 4–6 weeks of a hospital admission in which NIV was required. Cost-effectiveness is greater in more severely ill patients, and in those with a higher risk of mortality or subsequent admission. Uncertainty remains around the cost-effectiveness of domiciliary NIV in stable patients with COPD, as well as patients within a stable population that might benefit most, and further research should focus on this area.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge the contribution of Rahul Mukherjee in assisting with the pricing of the various non-invasive ventilation machines, as well as providing information for JH and SJ on the use of the machines in clinical practice. We would also like to acknowledge the contribution of Malcolm Price, for statistical guidance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JamesHall795, @SusieJ71
Contributors JH edited the existing model, updated model parameters, conducted statistical analyses, performed the economic analysis and wrote the paper with guidance from SJ, AMT, JD and DM. SJ designed the original health economic analyses, supervised the economic modelling and contributed to writing the paper. AMT provided clinical guidance on and identified the updated model parameters and contributed to writing the paper. JD and DM designed the systematic review from which the hospitalisation data was drawn, advised on use of parameters in the economic model and contributed to the writing of the paper. JD led and undertook the systematic review. SJ is the guarantor and accepts full responsibility for the work and the conduct of the study, and controlled the decision to publish.
Funding This study was funded by a non-commercial grant from ResMed and Phillips. The funders had no input to the study design, conduct or interpretation of the results.
Competing interests AMT has received grant funding to her institution for the work contained in the manuscript from ResMed/Phillips, which funded JH and JD, as well as contributions for oversight from DM and SJ. She has also received grant funding and/or honoraria from several companies involved in treatment of COPD, specifically AstraZeneca, Chiesi, GSK and Boehringer Ingelheim.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.