Article Text

Abstract
Rationale The heterogeneity in efficacy observed in studies of BCG vaccination is not fully explained by currently accepted hypotheses, such as latitudinal gradient in non-tuberculous mycobacteria exposure.
Methods We updated previous systematic reviews of the effectiveness of BCG vaccination to 31 December 2020. We employed an identical search strategy and inclusion/exclusion criteria to these earlier reviews, but reclassified several studies, developed an alternative classification system and considered study demography, diagnostic approach and tuberculosis (TB)-related epidemiological context.
Main results Of 21 included trials, those recruiting neonates and children aged under 5 were consistent in demonstrating considerable protection against TB for several years. Trials in high-burden settings with shorter follow-up also showed considerable protection, as did most trials in settings of declining burden with longer follow-up. However, the few trials performed in high-burden settings with longer follow-up showed no protection, sometimes with higher case rates in the vaccinated than the controls in the later follow-up period.
Conclusions The most plausible explanatory hypothesis for these results is that BCG protects against TB that results from exposure shortly after vaccination. However, we found no evidence of protection when exposure occurs later from vaccination, which would be of greater importance in trials in high-burden settings with longer follow-up. In settings of declining burden, most exposure occurs shortly following vaccination and the sustained protection observed for many years thereafter represents continued protection against this early exposure. By contrast, in settings of continued intense transmission, initial protection subsequently declines with repeated exposure to Mycobacterium tuberculosis or other pathogens.
- tuberculosis
- clinical epidemiology
- respiratory infection
Data availability statement
Data are available in a public, open access repository. Stata code for meta-analysis, and the data and Python V.3.6 code for generating figures 2 and 3 are available at https://github.com/jtrauer/bcg_tb_context_review.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key message
What is the key question?
What is the reason for the extreme variation in efficacy estimates between trials of BCG vaccination?
What is the bottom line?
Variation in background intensity of Mycobacterium tuberculosis transmission is able to explain the considerable heterogeneity in the results of trials of BCG vaccination, with sustained protection more evident in settings of declining transmission.
Why read on?
We propose a new framework for understanding the substantial variation in BCG vaccination trial results, with profound implications for understanding BCG’s effects on the global tuberculosis epidemic.
Introduction
Tuberculosis (TB) is the world’s leading infectious disease killer,1 and BCG is the only approved vaccine for its control. Global BCG coverage was 88% in 2019, close to the highest coverage of any vaccination.2 The substantial heterogeneity in the efficacy of BCG vaccination between studies has long been recognised, with study-level variables such as age, latitude and BCG strain able to explain some of this variation in meta-analyses unrestricted by age.3–5
Past attempts to understand this heterogeneity have often started from the assumption that protection wanes with time from vaccination.6 7 However, time since vaccination parallels immunological maturation and changing TB phenotype,8–10 which may lead to confounding. While retrospective national health data have shown that vaccine effectiveness can be sustained for >15 years,11 12 multiple observational studies in low-burden settings have found that past history of BCG vaccination significantly increases subsequent disease risk in TB contacts.13 14
These observations suggest that intensity or timing of M. tuberculosis (Mtb) exposure relative to age and time since vaccination may be important in determining vaccine effectiveness. However, no coherent theoretical framework has been proposed to explain the diversity of results and the adverse effects of BCG sometimes observed. Because of the markedly different disease phenotypes and onset timing relative to age of exposure,14 15 we reviewed evidence for the efficacy of BCG vaccination with a focus on TB-related epidemiology, diagnostic approach, time from vaccination and age.
Methods
Reference management
We performed a systematic review of studies of the effect of BCG vaccination on TB disease, including subcategories of TB disease, with search strategy and inclusion/exclusion criteria identical to Abubakar et al5 and consistent with our PROSPERO-registered protocol (CRD42019119676), but with search dates extended to 31 December 2020 (section 2, online supplemental appendix). Details of our search strategy are presented in section 13 of online supplemental appendix. We focused on clinical trials as the highest form of evidence, but also reviewed cohort studies as a secondary level of evidence, as presented in the study profile (figure 1). We considered studies comparing participants receiving their first BCG vaccination against unvaccinated controls, excluding trials of BCG revaccination, consistent with previous reviews. No further eligible trials were identified that had not been included in the earlier review, with the recent trial of placebo, H4:IC31 vaccine and BCG (which observed no TB cases) excluded as a revaccination trial.16 All data extracted from studies published from 2009 to 2020 were reviewed by two authors.
Supplemental material

Modified PRISMA flow diagram. aIncludes two reports of one revaccination trial which observed zero cases of TB during follow-up. bTrials in Chicago medical students, Chicago nursing students and New York infants were not included in Mangtani review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; TB, tuberculosis.
Data extraction
We describe all trials in detail in our extended narrative review (sections 3–11, online supplemental appendix). Unlike previous reviews,4 5 17 we considered how age-specific reactivation profiles may be influenced by the background intensity of Mtb transmission and formulated a new classification for included trials and conceptual framework for integrating their results. Specifically, we considered participant age, local background TB burden and duration of follow-up as the main factors in classifying included trials. Trials not exclusively recruiting neonates have previously been grouped according to study-level factors, including: stringency of latent TB infection (LTBI) testing, as either single or multiple tests; and age group, as either school aged or other age. However, previous reviews classified several studies as ‘other age’, even though most participants were children, which we believe is misleading.4 5 We also identified errors in the previous reviews (section 2.3, online supplemental appendix), including two major trials incorrectly assigned according to the authors’ classification system, with the differences between our results and those of the previous reviews confirmed by three authors blinded to each other’s assessment (JMT, AK and RR).
Because the Chengalpattu trial was the largest ever trial of BCG vaccination, was performed in a high-burden setting and was relatively recent, we also obtained unpublished estimates from this study disaggregated by age and time from vaccination. To illustrate the interacting effects of age and time from vaccination, we extracted data from reports of trials for which data could be disaggregated by both age at TB diagnosis and time from vaccination, in combination with the previously unpublished data from the Chengalpattu trial.
Data synthesis and analysis
We used a hierarchical approach to estimating effect sizes, given the diverse approaches to presenting outcomes. Where possible we estimated effect sizes from information on person-years of follow-up and number of cases occurring in the vaccinated and unvaccinated groups. If this was unavailable, we estimated follow-up periods from the information provided (section 2.2, online supplemental appendix).
In our classification, we first grouped all trials in neonates and young children into a single category. Next, we divided the remaining trials into those recruiting predominantly older children and adolescents or those recruiting predominantly adults, and considered the studies with follow-up periods of no more than 5 years separately from those with longer follow-up. Of the remaining trials with longer follow-up, we classified according to whether transmission remained substantial or declined to low levels during the follow-up period. This required some subjective judgement, given that burden indicators were invariably not reported at the exact level that the study was undertaken. However, there were important differences between these studies with regard to TB burden. For the paediatric studies, we considered that burden was likely to have been higher in Puerto Rico by the end of the 1960s (around 12 deaths per 100 000 per year)18 than it was in the UK in the early 1970s (<2 deaths per 100 000 per year), the USA in the late 1960s (2–3 deaths per 100 000 per year) and the USA in the late 1990s (<0.5 deaths per 100 000 per year). For the adult studies, burden was likely to have been considerably lower in the general population in 1970 than in psychiatric inpatient care in 1960 in the USA, and while India had substantial TB transmission throughout the duration of the Chengalpattu trial, mortality fell approximately ten-fold in Madanapalle due to the highly effective active case finding campaign linked to this BCG trial.19
Meta-analysis was performed under our new classification with Stata V.16.1. The forest plot was generated using the random effects model of DerSimonian and Laird with the Mantel-Haenszel assessment of heterogeneity from the metan package. Pooled effect size estimates and confidence limits are also presented using REML with Knapp-Hartung adjustment provided by Stata’s meta function.
Stata code for meta-analysis and the data and Python 3.6 code for generating figures 2 and 3 are available at https://github.com/jtrauer/bcg_tb_context_review.
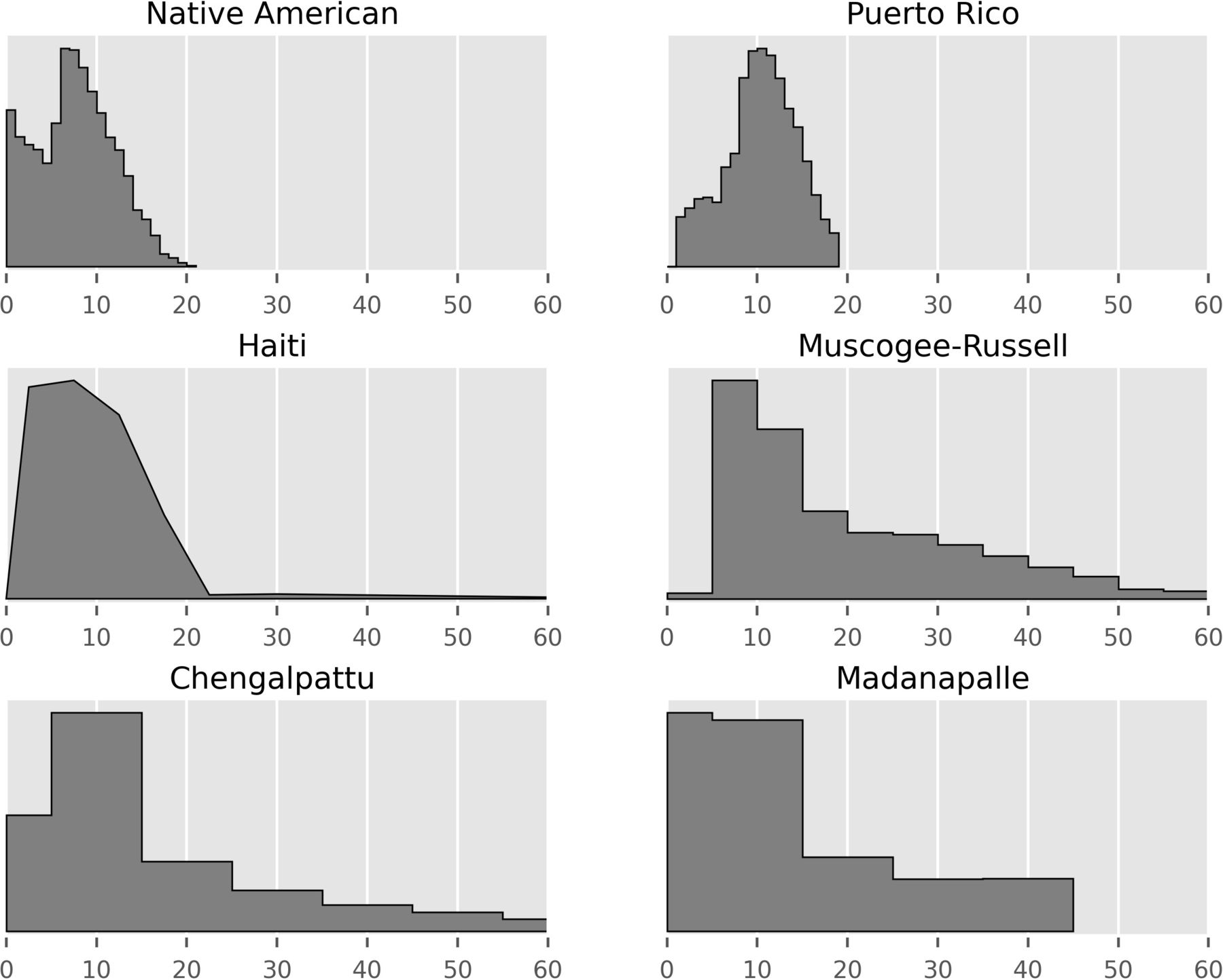
Age distribution (in years) of participants in studies for which these data were provided. Studies with very narrow age inclusion criteria not presented (ie, five neonatal trials and English cities trial of children aged 14–15½ years). All age distributions normalised to the same maximum vertical height.

Distribution of cases of active TB occurring in the vaccinated (red) and unvaccinated (blue) populations in which timing of cases by age can be determined to within a 5-year interval. The area of each marker is set proportional to the number of cases occurring within a certain time/age interval and then linearly scaled by an arbitrary value for visual effect. First six studies assigned to vaccinated and control in a 1:1 ratio, while Chengalpattu assigned in ratio of 2 BCG: 1 control, with the size of the vaccinated circles halved to compensate for this effect. Madanapalle panel presents results for bacteriologically-confirmed cases only. First panel data obtained from table IV of Ferguson 1949,20 second panel data obtained from figure 1 of Rosenthal 1961,23 third panel data obtained from table 3 of MRC 1972,54, fourth panel data obtained from table 3 of Rosenthal 1963,37 fifth panel data obtained from tables 1 and 2 of Bettag 1964,40 sixth panel data obtained from table 5 of Frimodt-Moller 1973,9 seventh panel presents previously unpublished data. TB, tuberculosis.
Results
Included studies are described in our narrative review (sections 3–11, online supplemental appendix) and summarised as follows and in table 1. Assessment of study quality according to standard criteria for the assessment of clinical trials has been undertaken in previous systematic reviews (online supplemental appendix),5 and our assessments did not deviate from these findings.
Characteristics of BCG vaccination trials
Neonatal vaccination trials
Of 21 included trials we identified, six recruited neonates only.20–25 A small minority of the participants in the Saskatchewan native infants and New York infants trials received oral vaccination, but most infants in these trials received parenteral vaccination. The trial in New York infants reported on TB-related mortality but not TB incidence, finding eight deaths in each of the vaccinated and control groups during its alternate assignment period.26 Although the trial undertaken in the lowest resource and likely highest transmission setting reported the lowest efficacy, estimates of protection were homogeneous, with most trials consistent with the pooled estimate of protection for trials in neonates and young children. Follow-up duration varied, although none followed participants into or beyond adolescence in a setting of continued intense transmission.
Trials recruiting young children
Although the Agra trial was previously included with school-aged vaccination and is only reported very briefly, participants were up to 5 years of age at entry.27 The efficacy in this trial was 60% (95% CI 17% to 81%) protection, consistent with estimates for neonates. The other trial recruiting the youngest children (previously classified as school aged) observed three cases of TB, all among control participants, also consistent with high childhood efficacy.28
Reclassification of trials not restricted to young children
The categorisation of these studies as ‘school’ or ‘other’ age fails to convey that many studies previously categorised as ‘other’ age predominantly recruited children. This often occurred because of an expansive population age pyramid and/or inclusion criteria that typically included negative LTBI testing, the prevalence of which declines with age, particularly in high-burden settings. A prime example is the population-wide Haiti trial, in which tuberculin skin test (TST)-negativity in adults was so rare that the protocol was modified to exclude participants aged over 20, resulting in a predominantly paediatric cohort (figure 2).29
Trials recruiting broadly across paediatric age ranges
Three trials recruited across most or all paediatric age ranges to approximately 20 years.29–31 The Haitian trial observed participants for 3 years, with one case occurring in the vaccinated and five in the controls, suggesting good short-term protection in a high transmission setting.29 The large Puerto Rico trial (previously misclassified as non-stringent TST) was undertaken in a setting of rapidly declining but substantial burden and showed modest efficacy.31 32 The trial in native Americans was undertaken in a setting in which rates of disease rapidly declined to very low levels throughout most of follow-up, with sustained efficacy for >60 years.21 30 33
Paediatric/adolescent trials
The trial in Georgia schools recruited ages 6–17, with the small number of cases that occurred all accruing after 6 years of follow-up.32 34 The large MRC-funded trial was undertaken in school children in large English cities and found high efficacy in a setting of rapidly declining burden (figure 3).35 36
Trials in young adults with shorter follow-up
Three trials from Chicago of participants at high risk because of occupational or residential exposure risk were included in this category, along with one trial of participants at high occupational risk from a high-burden setting. The trial of mental health patients observed only one case of ‘bilateral minimal arrested TB’ in 35 participants, providing little information. Two reports from Chicago describe BCG vaccination trials in students of nursing and medicine followed for the duration of their studies. Both were small and excluded from previous reviews for methodological limitations, with only 11 cases occurring across both trials.4 37 38 The trial in South African mine workers was also excluded from past reviews for including some participants who were TST-positive at baseline,6 but found fewer cases in the vaccinated over 3.6 years of follow-up.39
Trials recruiting across all ages with extended follow-up
The trial in Muscogee and Russell counties, USA, achieved broad community participation in those aged over five in a setting of low and declining transmission, finding slightly fewer cases in the vaccinated.32 34 The trial in Lincoln State School describes an adult cohort followed in a high transmission setting and suggested a trend towards more cases in the vaccinated, particularly after 5 years of follow-up (figure 3).40
The Chengalpattu trial was the largest BCG vaccination trial ever undertaken and was among the best reported, although it employed one-stage TST screening.41 It enrolled participants aged 1 month and above, followed for 15 years in a very high transmission setting and found slightly higher TB rates in the BCG vaccinated, although protection was suggested in children.42 The Madanapalle trial43 followed participants for 21 years in an initially high transmission setting and focused on the end point of smear-positive TB, which likely explains the low number of paediatric cases (figure 3).9 Although previously classified as employing stringent TST testing, one-stage testing with a cut-off of <5 mm was used in around 95% of participants.
Meta-analysis
Heterogeneity was not observed when studies were grouped according to our classification (figure 4). The pooled estimate for the incidence rate ratio of BCG vaccination in trials of neonates and young children was 0.26 (95% CI 0.17 to 0.35). For other paediatric studies in high-burden settings, we refer readers to the descriptions of the original trials. For paediatric studies with longer follow-up in settings of declining burden, the incidence rate ratio was 0.25 (95% CI 0.20 to 0.30). Trials of adults in high-burden settings with short follow-up durations were methodologically heterogeneous, but the pooled estimate suggested benefit, with an incidence rate ratio of 0.59 (95% CI 0.31 to 0.87). Trials of adults with longer follow-up duration were all consistent with a null overall effect, with marginal protection suggested in settings of declining burden and the Chengalpattu trial dominating the effect estimate in high-burden settings.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of TB incidence rate ratios from trials of BCG vaccination by participant demographics and background epidemiology. Pooled effects are from random effects meta-analysis. Pooled estimates with confidence limits when using a restricted maximum likelihood model with Stata 16.1 and Knapp-Hartung adjustments were: all neonatal and young children: 0.27 (0.15, 0.40); Paediatric/adolescent, declining burden, longer follow-up: 0.25 (0.17, 0.33); adult, short follow-up: 0.59 (0.42, 0.77); adult, declining burden, longer follow-up: 0.86 (0.08, 1.64), adult, high-burden, longer follow-up: 1.05 (0.50, 1.61). New York infants trial not included because only the outcome of TB-related deaths was reported from this trial. TB, tuberculosis.
Cohort studies
Observational studies are summarised in online supplemental appendix table 1.
Study quality
Study quality is discussed with a focus on TB epidemiological context throughout our narrative review (online supplemental appendix). Standard risk of bias assessments were also performed, with all results identical to those of Abubakar et al5 (Appendix 4, first table).
Discussion
Few trials of BCG vaccination followed participants for more than 5 years post-vaccination, but of those that did, settings with sustained exposure risk showed lower effectiveness than those in which risk predominantly accrued shortly after vaccination. Therefore, we propose that timing of Mtb exposure, rather than timing of TB disease, should be the main consideration in understanding the differences in BCG efficacy between settings (table 2). In settings of rapidly declining TB burden, exposure is less likely further from vaccination and the effect of BCG in preparing the participant’s immune system for early exposure is robust. By contrast, in sustained high-burden settings, participants are more likely to be exposed after a longer period from vaccination when BCG efficacy has waned or after re-exposure has occurred. This interpretation implies that BCG is likely to have little effect in settings of persistent exposure.
Proposed conceptual framework for understanding the effect of BCG vaccination
None of the eight studies of neonates or young children followed a substantial cohort of participants into the high-risk adolescent period in a high-transmission setting, but all were consistent with significant protection in early life. Among paediatric and adolescent trials, two larger studies in settings of declining burden showed substantial protection, and one suggested short-term protection in a high-burden setting. In adults, four high-quality studies with long-term follow-up have been undertaken, with the two performed in high transmission settings suggesting a null or adverse effect,40 41 while one in a low transmission setting32 34 and one linked to case finding43 suggested modest protection. Methodologically heterogeneous trials with short follow-up of participants were also consistent with short-term protection in adults.
Included trials predominantly considered persons without prior Mtb sensitisation; however, the background intensity of Mtb transmission remains relevant to the relative importance of early and late reactivation.44 In settings of declining burden, TB episodes many years from vaccination are more likely to represent progression of infection acquired shortly following vaccination. Conversely, in high-burden settings, late-presenting episodes may result from later exposure. Under this conceptual framework, trials in both low-burden and high-burden settings will show high initial effectiveness, whereas later protection is dependent on transmission intensity. As late reactivation is commoner in adolescence and adulthood,14 these effects will be less apparent in studies that do not follow participants passing into adulthood. The recent BCG and H4:IC31 revaccination trial was conducted in adolescents in a high-burden setting. BCG boosting in those previously BCG-vaccinated decreased persistent Mtb sensitisation, consistent with short-term protection from infection.16
A null effect in studies enrolling across a broad range of ages should not necessarily be interpreted as lesser protection in older participants, because such studies may include substantial cohorts of young children and follow-up invariably emphasises the early post-vaccination period. We found marked and significant effects for young children and for the immediate post-vaccination period, which would be expected to favour a protective overall effect in many trials. Therefore, it is plausible that protection remains present in these groups in some trials with longer follow-up and a broad age range of participants, but is offset by adverse effects in adults in the late post-vaccination period. An example is the Chengalpattu trial which reported considerable protection in children aged <15 during the first 12.5 years of follow-up,42 but with a marginally deleterious effect in the trial overall. We expected to observe marked protection in children and in the early post-vaccination period with increased rates of TB in the later follow-up period in adults on reanalysis of this trial. These patterns were only observed to a very limited extent in this trial, and although this pattern was suggested in the Lincoln State School, numbers were lower.
Our framework for understanding BCG efficacy is biologically plausible because the most favourable outcome following exposure is stable immune tolerance, and because the immunology of TB differs fundamentally between infants, children and adults.10 Infants, with reduced capacity of antigen-presenting cells, show higher mortality and more frequent disseminated TB, which is ameliorated by BCG enhancing early Mtb containment.45 Ages 5–14 years represent an epidemiological paradox of low TB risk despite high Mtb exposure in high-burden settings, during which vaccination may be less important.46 However, ‘trained’ immunity, which refers to epigenetic modulation of innate immune cells (monocyte, NK and γδT-cells in the case of BCG) may become increasingly important into adulthood, as TB rates increase and the classic pulmonary cavitary disease phenotype emerges.47 If by 15–20 years post-vaccination acquired T cell protection wanes, but trained immunity persists, then the host will have lost the beneficial T cell-mediated effects of BCG, but acquired a persistent hyper-reactive innate response, which is consistent with transcriptomic evidence.48 Therefore, because TB disease is immunologically mediated, it is plausible that inducing T cell sensitisation to a broad range of Mtb antigens could protect against the first encounter with the organism during an age of suboptimal immunity, but have a reduced or adverse effect with repeated exposure in adulthood, when the immunological response is vastly different.
Past reviews have proposed that between-trial heterogeneity may be partially explained by latitudinal gradient in non-tuberculous mycobacteria (NTMs) exposure, particularly in studies employing one-stage TST testing.4 These arguments require that: (1) NTM sensitisation decreases with latitude, (2) TST positivity detectable only with two-stage testing frequently represents sensitisation to NTMs rather than Mtb, (3) NTM sensitisation confers immunity to Mtb and (4) because of NTM-conferred immunity to Mtb, BCG vaccination boosts immunity to Mtb to a lesser extent in those with NTM sensitisation than those without. Although point (1) is well-established, latitudinal gradient also applies for Mtb. To our knowledge, evidence is conflicting for point (2)38 and derived from animal models for points (3)49 and (4).50 The greater rates of TB observed in NTM-naïve persons at an equivalent TST response51 likely reflect a greater probability of Mtb infection. Reanalysis of the Chengalpattu study suggested somewhat lower protection in NTM-sensitised participants,52 although the statistical significance of this finding was unclear, while the one trial conducted across sites at multiple latitudes found similar effects by location.32 Although we do not discount the importance of NTM sensitisation, a greater effect of vaccination on clearly TST-negative participants and young children would also support our hypothesis. That is, if the lower efficacy of BCG distant from vaccination is attributable to accumulated exposure to Mtb, then exposure to both Mtb and NTMs could have similar effects in mitigating vaccine efficacy. As such, the recent success of the M72/AS01E trial in Mtb-exposed, predominantly BCG-vaccinated adults in a high-burden setting supports the need for revaccination with new antigens to mitigate any increased risk from past BCG vaccination.53
We, therefore, believe that our hypothesis is supported by the evidence to a considerably greater extent than previously accepted explanations. However, as is common in empiric research, not every aspect of the analysis is perfectly consistent with the hypothesis. For example, our hypothesis does not explain the adverse effect suggested in the Georgia schools trial, although the confidence intervals were wide due to low case numbers and heterogeneity was not observed in this trial category. We also expected more TB cases in the vaccinated group late from enrolment in the Chengalpattu trial, which was seen to only a minor extent. As previously suggested, this may be explained by high rates of pre-existing Mtb exposure in both the control and vaccinated participants because of one-stage TST testing.
We propose that BCG vaccination protects against early post-vaccination exposure to Mtb, but is ineffective with later exposure, that the results of most or all past trials of BCG vaccination are consistent with this hypothesis and that this framework is more plausible than previously proposed explanations. We believe this explanation is also highly intuitive in retrospect, but may not have been recognised previously because Mtb sensitisation at recruitment has generally been excluded in trial participants based on TST. The absence of an effect late from follow-up in high transmission settings is infrequently observed because it is only seen in studies with long follow-up undertaken in high-burden settings, which are also the most logistically challenging to perform. Given that no clinical trial has found a statistically significant increased risk of disease, any increased rates of TB from late post-vaccination Mtb exposure may not represent an increased lifetime risk in high-burden settings. However, deferring episodes of disease could still have extremely important epidemiological effects, given that paediatric TB more often results in serious sequelae, whereas adult TB is more infectious and critical to perpetuating the epidemic. It is essential that future studies of TB risk and the effect of BCG vaccination present results disaggregated by age and time from exposure to fully elucidate these distinct reactivation profiles.
Data availability statement
Data are available in a public, open access repository. Stata code for meta-analysis, and the data and Python V.3.6 code for generating figures 2 and 3 are available at https://github.com/jtrauer/bcg_tb_context_review.
Acknowledgments
We express our great thanks to the staff of the National Institute for Research in Tuberculosis for providing the disaggregated results used to generate the last panel of figure 3, including Dr Srikanth Tripathy, Basilea Watson and others. We also gratefully acknowledge the contribution of the following individuals who assisted with data extraction for non-English language papers: Eike Steinig, Maddalena Cerrone and Joanna Zając.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JamesTrauer
Contributors JMT designed the study. AK and JMT designed and performed the literature search. AK, JMT, RR and BMW contributed to data extraction and analysis. JMT wrote the first draft and all authors contributed to producing the final text of the manuscript.
Funding JMT is a recipient of an Early Career Fellowship from the Australian National Health and Medical Research Council (APP1142638).
Disclaimer The authors acknowledge that the article title for reference Bettag et al, 1964 may cause offence and would like to note that 'mentally retarded' is not an acceptable terminology but is one that was used during the time of the publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.