Article Text

Abstract
Background The prevalence of venous thromboembolic event (VTE) and arterial thromboembolic event (ATE) thromboembolic events in patients with COVID-19 remains largely unknown.
Methods In this meta-analysis, we systematically searched for observational studies describing the prevalence of VTE and ATE in COVID-19 up to 30 September 2020.
Results We analysed findings from 102 studies (64 503 patients). The frequency of COVID-19-related VTE was 14.7% (95% CI 12.1% to 17.6%, I2=94%; 56 studies; 16 507 patients). The overall prevalence rates of pulmonary embolism (PE) and leg deep vein thrombosis were 7.8% (95% CI 6.2% to 9.4%, I2=94%; 66 studies; 23 117 patients) and 11.2% (95% CI 8.4% to 14.3%, I2=95%; 48 studies; 13 824 patients), respectively. Few were isolated subsegmental PE. The VTE prevalence was significantly higher in intensive care unit (ICU) (23.2%, 95% CI 17.5% to 29.6%, I2=92%, vs 9.0%, 95% CI 6.9% to 11.4%, I2=95%; pinteraction<0.0001) and in series systematically screening patients compared with series testing symptomatic patients (25.2% vs 12.7%, pinteraction=0.04). The frequency rates of overall ATE, acute coronary syndrome, stroke and other ATE were 3.9% (95% CI 2.0% to to 3.0%, I2=96%; 16 studies; 7939 patients), 1.6% (95% CI 1.0% to 2.2%, I2=93%; 27 studies; 40 597 patients) and 0.9% (95% CI 0.5% to 1.5%, I2=84%; 17 studies; 20 139 patients), respectively. Metaregression and subgroup analyses failed to explain heterogeneity of overall ATE. High heterogeneity limited the value of estimates.
Conclusions Patients admitted in the ICU for severe COVID-19 had a high risk of VTE. Conversely, further studies are needed to determine the specific effects of COVID-19 on the risk of ATE or VTE in less severe forms of the disease.
- pulmonary embolism
- viral infection
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is the key question?
Are arterial and venous thromboembolic events common in patients with COVID-19, and what condition may modify their prevalence?
What is the bottom line?
Our results suggested that venous and, in to a lesser extent, arterial thromboembolism, are common in patients with COVID-19 admitted in the intensive care unit, despite thromboprophylaxis. The systematic screening of venous thromboembolism may be relevant.
Why read on?
This is the first systematic evaluation of existing evidence regarding thrombotic manifestations of COVID-19, summarising the current evidence on a novel spectrum of this viral disease.
Introduction
COVID-19 is a viral respiratory illness caused by SARS-CoV-2. In severe cases, COVID-19 is characterised by cytokine outburst and hyperinflammation, platelet activation, endothelial dysfunction and sepsis-related coagulopathy.1 Consistently, high levels of D-dimers were repeatedly shown to be associated with the need for intensive care unit (ICU) admission and mortality among patients with COVID-19.2 While initial anecdotal reports described cases of pulmonary embolism (PE) diagnosed concomitantly with COVID-19,3 more recent observational studies suggested that venous thromboembolic events (VTEs) are common among patients with COVID-19 hospitalised in the ICU, thrombosis prevalence ranging from 0%4 to 69%.5 Few series also suggested an elevated incidence of arterial thromboembolic events (ATEs).6 7 Importantly, however, these prevalence estimates have been largely inconstant with a high heterogeneity across studies and are subjected to several biases. Moreover, many series also reported a low prevalence of deep vein thrombosis (DVT),4 questioning the peculiar mechanism responsible for pulmonary vessel occlusions.
While international experts recently recommended an early therapeutic anticoagulation for these patients despite the increased risk of bleeding and previous negative trials of endogenous anticoagulants in sepsis,8 9 relevant estimates of the occurrence of ATE and VTE are lacking to inform on the best therapeutic approach in these patients. Therefore, the present meta-analysis aimed to determine the prevalence of VTE and ATE in patients with COVID-19.
Materials and methods
This systematic review and meta-analysis (http://www.crd.york.ac.uk/PROSPERO, CRD42020184252) was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions10 and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.11
Search strategy
A literature search was performed to identify all published studies reporting thromboembolic events in COVID-19. MEDLINE, Embase and Google Scholar were searched between 1 January 2020 and 30 September 2020 using the keywords “coronavirus”, “severe acute respiratory syndrome coronavirus 2”, “SARS-CoV-2”, “novel coronavirus”, “nCoV”, “2019-nCoV”, and “COVID-19” and “thrombosis”, “stroke”, “myocardial infarction”, “acute coronary syndrome”, “pulmonary embolism” and “venous thromboembolism” (see appendix). The websites of major journals were also searched, including the New England Journal of Medicine, Journal of the American Medical Association, Lancet, Lancet Haematology, British Medical Journal, Journal of the American College of Cardiology, Circulation, Journal of Thrombosis and Haemostasis, Thrombosis and Haemostasis and Thrombosis Research. Bibliographies of each included study, as well as any review article, systematic review, meta-analysis or text found were also searched for additional papers that may contain further studies. Given that preprint papers in databases such as bioRvix and medRvix were not peer-reviewed, we did not include papers found in such databases in our analysis to avoid any potential misinformation being disseminated. There was no restriction on the language and type of publication.
Study selection
The inclusion criteria for studies were the following: (1) cohort studies of >10 patients, (2) patients with COVID-19 (positive reverse transcription PCR (RT-PCR)) or positive CT scan in patients with suggestive gestalt) and (3) available rate of objectively documented ATE or VTE as defined by investigators. Moreover, publications specific to the paediatric population were excluded.
The titles and abstracts of all articles were independently reviewed by two authors (BKT and J-CL). If pertinent, each reviewer independently retrieved and explored complete articles to make a final decision about their inclusion in the meta-analysis. Disagreements were resolved by consensus or by consulting a third reviewer (SM). Throughout this process, the reviewers were blinded to authors’ names, journal and year of publication of the papers. If studies that had been reported in multiple papers were identified, the analysis was limited to the largest cohort unless the necessary data had appeared only in another paper. A log of reasons for rejection of citations identified from the searches was kept.
Outcomes
The main outcomes were the rate of distal (located below the knee) and proximal (involving popliteal, femoral, iliac vein and inferior vena cava) DVT, VTE (distal and proximal DVT and PE) and the rate of ATE (myocardial infarction, stroke, limb and visceral arterial ischaemia).
Assessment of methodological quality
The methodological quality of the selected studies was systematically evaluated using the Methodological Index for Non-randomised Studies (MINORS), which contains six items for non-comparative studies.12
Data extraction
Two reviewers (BKT and J-CL) independently extracted study design; the study country; patient characteristics, including the proportion of patients hospitalised in the ICU; the method used to diagnose COVID-19 and VTE; the follow-up duration, whether symptomatic testing versus asymptomatic screening was performed; and the proportion of patients receiving anticoagulants.
Statistical analysis
We constructed a random-effects (Mantel-Haenszel) model to obtain a summary estimate and 95% CI for the prevalence of VTE and ATE using arcsine transformation. These data were combined by using an approximation to the inverse variance approach, effectively weighting each study according to its sample size. Arcsine transformation was used to stabilise the variance.13 I2 statistic for heterogeneity was used to assess between study heterogeneity. To investigate sources of heterogeneity in the main analysis, if any, we planned a priori subgroup analyses for relevant categorical variables (single centre vs multicentre, consecutive vs non-consecutive series, retrospective vs prospective, systematic assessment of thrombosis vs symptomatic testing, a majority of included patients being hospitalised within the ICU or not), as well as metaregression for continuous variables (study size, the MINORS score, proportion of male sex,14 mean lymphocyte count15 and D-dimer value,15 proportion of patients hospitalised in the ICU,14 proportion of patients receiving anticoagulants). Metaregression was not performed if the number of studies was ≤10 to avoid overfitting using linear weighted random/mixed-effects model (rma function, metafor package).16
Publication bias was assessed visually using funnel plots. We assumed that the effect of publication bias should be minor if the plot of the magnitude of effect size in each study versus its precision estimate (ie, SE) shows a roughly symmetrical funnel shape. We also formally tested the presence of publication bias using the SE-based and study size-based funnel plot and related asymmetry tests. All analyses were performed with R (R Foundation for Statistical Computing, Vienna, Austria).
Results
Literature search and agreement
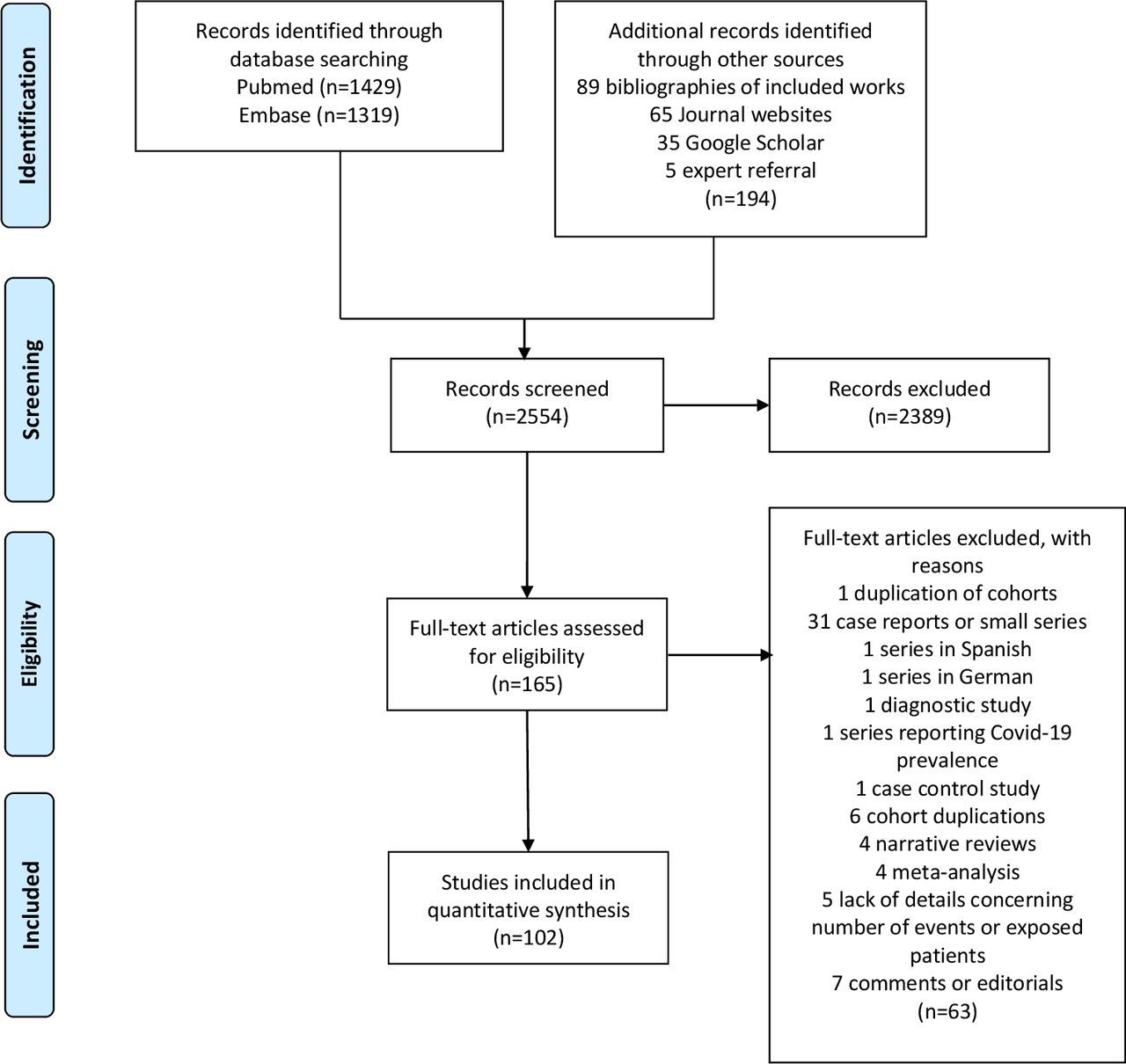
A total of 2554 articles were retrieved by the search terms. After reviewing titles and abstracts, 165 articles were selected for the full-text eligibility. Finally, 102 studies (64 503 patients) were included (figure 1).

Study selection.
Study characteristics
Among included studies, 81 series assessed COVID-19-related VTE and 20 studies reported ATE. The characteristics of the included studies are described in online supplemental table S1. The patient number varied from 12 to 12 630. Twenty-three (23%) studies were prospective; 74 (73%) included consecutive patients. Thirty-four (33%) studies were conducted in ICU. Two studies used electronic medical records to identify thrombotic events.17 18 Eligible studies ranged in size from 12 to 12 630 patients, while mean follow-up duration ranged from 8 to 86 days. The presence of DVT and PE was confirmed with ultrasonography and CT scan, respectively, although PE was confirmed using echocardiography in patients with high suspicion in two studies.7 17 Thirty-seven (36%) studies, mainly letters, did not report the method of VTE detection. The all-cause mortality varied from 0% to 64%. The rate of patients receiving pharmacological VTE prophylaxis ranged from 16% to 100%. The median MINORS quality score was 7 (range 1–12) (online supplemental table S2).
Supplemental material
Venous thromboembolism
The overall weighted frequency of COVID-19-related VTE was 14.7% (95% CI 12.1% to 17.6%, I2=94%; 56 studies; 16 507 patients; figure 2).4 5 15 17–68 The visual inspection of funnel plot and the Egger’s regression test (p<0.0001) were in favour of publication bias (online supplemental figure S1). VTE included PE (7.8%, 95% CI 6.2% to 9.4%, I2=94%; 66 studies; 23 117 patients; online supplemental figure S2)4–7 15 17–19 21–25 29 29–31 33 34 36–52 55 56 58 59 61 63–67 69–88 and leg DVT (11.2%, 95% CI 8.4% to 14.3%; I2=95%; 48 studies; 13 824 patients; online supplemental figure S3).4–7 15 17 18 22–25 29–31 33 34 36 37 41–45 48–51 55–58 60 61 64 65 67 69 72 85 89–98 Few PE events resulted from isolated subsegmental PE (1.5%, 95% CI 0.9% to 2.4%; I2=75%; 22 studies; 1391 patients; online supplemental figure S4),4 7 17 24 30 34 39 48 51 53 55–57 60 63 64 67 73 76 78 81 99 whereas distal DVT (10.9%, 95% CI 4.8% to 18.9%, I2=97%; 19 studies; 2421 patients; online supplemental figure S5)4 19 22 23 30 34 36 38 53 55 57 67 88–90 93 94 97 100 was more frequent than proximal DVT (4.8%, 95% CI 2.8% to 7.2%, I2=89%; 26 studies; 3735 patients; online supplemental figure S5).4 17 19 22 23 26 30 34 36 38 40 41 49 53 55–57 59 65 67 88–90 93 94 97 100 In subgroup analyses, the VTE prevalence was significantly higher in ICU cohorts than cohorts including mixed patients (23.2%, 95% CI 17.4% to 29.6%; I2=92%, vs 9.0%, 95% CI 6.9% to 11.4%; I2=95%; pinteraction<0.0001; figure 2 and table 1). Post hoc subgroup analyses retrieved similar interactions for PE (13.5%, 95% CI 9.5% to 18.1% vs 5.2%; 95% CI 3.9 to 6.7; pinteraction<0.0001; online supplemental figure S2), DVT (21.1%, 95% CI 13.8% to 29.5% vs 4.7%, 95% CI 2.9 to 6.8; pinteraction<0.0001; online supplemental figure S3) and proximal DVT (9.0%, 95% CI 3.5% to 16.6% vs 2.6%, 95% CI 1.2 to 4.5; pinteraction<0.0001; online supplemental figure S6). This relation between ICU admission and VTE prevalence was supported by metaregression analyses (table 2 and figure 3). In addition, the VTE prevalence was higher in multicentric versus monocentric series, in studies using systematic screening versus symptomatic testing (table 2 and online supplemental figure S7), in larger cohorts and in studies with high mean D-dimers values (table 2). Conversely, the VTE prevalence was not associated with the MINORS score, the proportion of patients receiving anticoagulation or the study design, and proportion of men (tables 2 and 3). The rate of ICU patients and systematic screening were significantly associated to VTE prevalence in multivariable metaregression (table 3).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material

Forest plot showing the pooled, weighted frequency of patients with venous thromboembolic events related to COVID-19 according to patient population. ICU, intensive care unit.

Metaregression of the VTE probability according to the rate of patients admitted in ICU. Circles indicate the design of studies included in the metaregression, black for studies testing symptomatic patients and grey for those using systematic screening. The size of the circles correspond to the study size. The red solid curve indicates the prediction of VTE prevalence. The red broken curves indicate the 95% CI of model prediction of VTE prevalence. ICU, intensive care unit; VTE, venous thromboembolism.
Subgroup analysis to explore heterogeneity in estimate of VTE prevalence
Metaregression to explore heterogeneity in estimate of venous thromboembolism prevalence
Mutivariable analysis of 47 studies reporting prevalence of venous thromboembolism
Arterial thromboembolism
The weighted frequency of ATE was 4.0% (95% CI 2.0% to 6.5%, I2=95%; 19 studies; 8249 patients),7 17 18 27 36 39 47 50 51 53–55 61 65–67 88 101 102 including myocardial infarction/acute coronary syndrome (1.1%, 95% CI 0.2% to 3.0%, I2=96%; 16 studies; 7939 patients),7 17 18 39 47 50 51 53 55 61 65 66 88 101–103 ischaemic stroke (1.6%, 95% CI 1.0% to 2.2%, I2=93%; 27 studies; 40 597 patients)7 18 27 36 39 42 45 47 50 51 53 55 61 65–67 101 102 104–112 and other ATE (0.9%, 95% CI 0.5% to 1.5%; I2=84%; 17 studies; 20 139 patients)7 17 18 27 47 50 51 53 55 61 65–67 88 101 102 106 (figure 4). The visual inspection of funnel plot and Egger’s regression test (p=0.008) were in favour of publication bias (online supplemental figure S1). Subgroup analyses (online supplemental table S3) and metaregression (online supplemental table S4) failed to identify other factor explained heterogeneity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing the pooled, weighted frequency of patients with ATE. Others included visceral and limb ischaemia. ACS, acute coronary syndrome; ATE, arterial thromboembolic event; MI, myocardial infarction.
Discussion
The present meta-analysis showed a high prevalence of VTE in patients with COVID-19, especially for those admitted to the ICU. The prevalence of ATE was also substantial, although the low number of studies reporting this outcome among patients with COVID-19 limited precise estimates of the ATE risk according to patients’ characteristics. Taken together, these observations suggest that systemic inflammation, traditional predisposing factors for VTE, as well as potential SARS–CoV2–COVID-19 endothelium interaction likely predispose to VTE and ATE in patients with severe COVID-19. Therefore, physicians should be aware of these complications and remain vigilant for signs of VTE and ATE in the context of the current pandemic.
With the number of identified COVID-19 cases increasing worldwide, it has become clear that infected patients may present in a number of ways. Early observational studies suggested that virtually all patients had parenchymal abnormalities on chest CT.113 Interestingly, however, pulmonary vascular thickening were also frequently observed in COVID-19 compared with non-COVID-19 pneumonia, implying a potential tropism of the virus for the pulmonary vasculature.114 This is not surprising since the SARS-CoV-2 interacts with its functional receptor from the host cells, the ACE 2 receptor,115 also present on the surface of endothelial cells of virtually all organs, but predominantly within the heart, lungs and kidneys.116 Consistently, diffuse lymphocytic endotheliitis, endothelial dysfunction and apoptosis resulting from direct viral infection have been reported within the lungs and other organs.117 Subsequently, observational studies suggested that VTE was common among patients with COVID-19 admitted to the ICU as well as a common autopsy finding following COVID-19-positive deaths despite systematic thrombosis prophylaxis.118
The present meta-analysis is consistent with these early descriptions. Interestingly, however, the VTE prevalence varied widely between included series. A major cause of these fluctuations was the study design: patients admitted to the ICU had a twofold increased risk of VTE compared with those admitted on general wards.14 99 Not surprisingly, asymptomatic screening was also associated with a higher VTE prevalence compared with symptomatic testing only. Other risk factors associated with VTE reported in series included increasing age,15 lymphopenia,15 34 male sex,14 34 increased D-dimer,15 34 60 99 increased activated partial thromboplastin time,15 invasive mechanical ventilation,14 as well as high levels of plasma factor VIII activity60 and factor Willebrand antigen.60 Interestingly, the exact mechanisms resulting in PE in severe COVID-19 have been questioned. Indeed, disseminated intravascular coagulation, a condition characterised by the generation of microthrombi in different organs, including the pulmonary circulation,119 has been frequently reported in non-survivors of COVID-19.120–122 Pulmonary microthrombi were also reported at lung dissection from critically ill patients with COVID-19.2 This is in line with the immunothrombosis model, which highlights the bidirectional relationship between the immune system and thrombin generation during severe infection123 and the pathogenesis of acute respiratory distress syndrome.124 The mechanisms involved in COVID-19-related thrombosis nonetheless remain unclear and may include, in addition to classical pulmonary thromboemboli, intravascular coagulopathy,1 118 125 126 systemic and endothelial inflammation promoting factor Willebrand antigen, fibrinogen and factor VIII activity,51 immune-mediated damage by antiphospholipid antibodies51 127 and hypoxaemia-induced vascular occlusion.51 128
Importantly, a recent study suggested that the pre-emptive anticoagulation with heparin was associated with decreased mortality among patients with significant sepsis-induced coagulopathy or markedly elevated D-dimer levels.129 Whether these beneficial effects were related to non-anticoagulant properties of heparin, including its anti-inflammatory,130 antiviral131 and protective effects on the pulmonary endothelium, remained unknown.132 As recognised by the authors, however, this retrospective study was subjected to bias, and its results were not replicated in subsequent studies, suggesting that conventional thromboembolic prophylaxis or therapeutic anticoagulant had limited effects on VTE risk in patients with severe COVID-19.5 99 Moreover, while the prevalence of VTE and ATE appears substantial, a previous series of 113 patients with severe sepsis and septic shock hospitalised in the ICU reported a VTE prevalence of 37.2%.133 Consistently, the prevalence of VTE for patients receiving thromboprophylaxis while hospitalised on general wards for other medical illnesses,134 135 as well as the ATE risk of patients with community-acquired pneumonia,136 137 was somewhat similar to that observed in patients with COVID-19 in the present meta-analysis. In the context of the increased risk of bleeding138 and previous negative trials of endogenous anticoagulants in sepsis,139 these indirect comparisons question the recent recommendations for an early therapeutic anticoagulation for patients with sepsis-related coagulopathy in the context of severe COVID-19.8 9 As a result, the efficacy, dosage and characteristics of patients most suitable for high-prophylactic doses or systemic anticoagulation remain to be demonstrated in prospective controlled studies before they become standard of care in patients who may also be at increased bleeding risk.4 17 48 50 85 99
The present study has some limitations. First, we only partially explained the high level of heterogeneity across studies for VTE. In other words, the estimates of VTE rate cannot be used to compute the individualised risk of a given patient admitted in the general ward or the ICU. Second, the prevalence may have been overestimated due to design, sampling, measurement, confounder and information biases. For example, follow-up duration was limited to the first few weeks following ICU admission, which is associated with the highest thrombotic risk.34 53 A high number of CT scans were also likely performed for COVID-19, with PE events being potentially observed as an incidental findings only. The increasing awareness about the association between COVID-19 and VTE–ATE may have also lowered the physicians’ threshold for ordering imaging studies, especially in case of suspected PE in patients in the ICU. Although sensitivity analyses excluding the two studies17 64 reporting potential PE using echocardiography yielded similar estimates for PE prevalence (data not shown), this method may have inflated the number of true PE in the context of ICU. Conversely, patients spuriously diagnosed as having COVID-19 may have been included, leading to potential underestimation of the true prevalence of thrombotic events if their conditions were associated with a lower risk of thrombosis. Third, given the high mortality in patients in the ICU, crude estimates may have biased thrombosis prevalence in patients in the ICU,140 unless competing risk is modelled as reported in three studies.18 34 53 Fourth, an assessment of the methodological quality showed deficiencies in most included studies. Accordingly, many of the studies were retrospective, combined with other limitations and could thus have led to overestimation of the true VTE–ATE prevalence. Finally, we could not exclude publication bias, given the results of Egger’s regression test and funnel plot, although the asymmetry of funnel plot may be related to the smaller ICU cohorts being at increased risk of VTE.141
In conclusion, patients admitted in the ICU for COVID-19 appear to have a high risk of VTE. Physicians should therefore have a high index of suspicion, especially in patients with some dissociation between relatively well-preserved lung mechanics and significant hypoxaemia. However, the optimal management for VTE prevention and treatment remains to be defined. Moreover, further studies are also needed to determine the specific effects of COVID-19 on the risk of ATE and VTE, especially in less severe forms of the disease.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LaurentBertole1
SP and J-CL contributed equally.
Correction notice This article has been corrected since it was published Online First. Affiliations for LB have been updated.
Contributors BKT, SM, SP and J-CL designed the study. BKT and J-CL performed study selection. BKT, J-CL and SM extracted data from selected studies. J-CL and SM performed the statistical analysis. SM, BKT, J-CL, AF, YD and SP analysed the data. This first draft was written by BKT, SP and J-CL. J-CL is the guarantor. All authors contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LB reports grants and personal fees from Sanofi; grants, personal fees and non-financial support from Leo-Pharma; personal fees and non-financial support from Aspen; grants, personal fees and non-financial support from BMS/Bfizer; grants, personal fees and non-financial support from Bayer during the conduct of the study. CG has received grants from Bayer and BMS/Pfizer. YD has received grants/research support from Bayer, Baxter, Baxalta, Novo Nordisk, CSL Behring, LFB, Pfizer, LeoPharma, Octapharma and Stago; and an educational grant from Takeda and honoraria from Bayer, Baxter, Novo Nordisk, CSL Behring, Sobi and Octapharma. SP reports grants from Actelion, AstraZeneca and Resverlogix outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Data have been provided in the figures and tables.
Linked Articles
- Airwaves