Article Text

Abstract
End points that are repeatable and sensitive to change are important in pulmonary arterial hypertension (PAH) for clinical practice and trials of new therapies. In 42 patients with PAH, test–retest repeatability was assessed using the intraclass correlation coefficient and treatment effect size using Cohen’s d statistic. Intraclass correlation coefficients demonstrated excellent repeatability for MRI, 6 min walk test and log to base 10 N-terminal pro-brain natriuretic peptide (log10NT-proBNP). The treatment effect size for MRI-derived right ventricular ejection fraction was large (Cohen’s d 0.81), whereas the effect size for the 6 min walk test (Cohen’s d 0.22) and log10NT-proBNP (Cohen’s d 0.20) were fair. This study supports further evaluation of MRI as a non-invasive end point for clinical assessment and PAH therapy trials.
Trial registration number NCT03841344.
- primary pulmonary hypertension
- imaging/CT MRI etc
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Pulmonary arterial hypertension (PAH) is progressive, leading to right ventricular (RV) failure and death.1 Accurate measurement of RV function is important for assessment of disease severity and prognosis.2–4 Despite new therapies and improvements in survival,5 PAH remains a life-shortening condition. MRI is the gold standard for RV assessment,6 has prognostic value2 and predicts clinical worsening7 in PAH. A trial end point that is highly repeatable, is sensitive to treatment and predicts outcomes would be highly desirable.8 9 MRI has been proposed as a trial end point in PAH,8 9 however, there is limited data on repeatability and treatment effect size.
Methods
Patients
Patients with PAH who were treatment-naïve commencing therapy, prevalent undergoing escalation of therapy and clinically stable requiring no escalation of therapy, were recruited. See online supplemental file S1.
Supplemental material
Study investigations
Investigations performed at visit 1 included N-terminal pro-brain natriuretic peptide (NT-ProBNP), 6 min walk test (6MWT) and MRI. Follow-up visits 2 and 3 occurred approximately 6 months after study visit 1. Visits 2 and 3 occurred within 24 hours of each other (online supplemental figure S2).
Supplemental material
MRI acquisition and analysis
All MRI examinations were performed on either a 1.5 T GE HDx (GE Healthcare, Milwaukee, USA) whole body scanner using an 8-channel cardiac coil or a 3 T Philips Ingenia (Best, The Netherlands) whole body scanner using a 32-channel dStream torso coil (online supplemental file S1). Analysis of MRI was undertaken blinded to the patient’s data. RV parameters and pulmonary arterial flow were analysed on Qmass MEDIS suite (V.3.0.18.0, Medical Imaging Systems, The Netherlands) on short axis and phase contrast images, respectively. Regions of interest were drawn on the pulmonary artery and left atrium of the dynamic contrast-enhanced perfusion images to calculate first pass pulmonary transit time and full width at half maximum using in-house software (see online supplemental figure S3).
Supplemental material
Six min walk test and NT-ProBNP
The 6MWT was performed by a respiratory physiologist. NT-ProBNP analysis was performed on patient plasma samples using the Luminex 100/200 multiplex analyser using the cardiovascular marker kit (HCVD1MAG-67K Millipore) at the end of the study.
Statistical analysis
Repeatability was determined by the intraclass correlation coefficient (ICC) using a two-way mixed absolute agreement model with the average measure recorded. An ICC of ≥0.75 was considered excellent, 0.60–0.74 good, 0.40–0.59 fair and <0.40 poor. Mean difference and 95% CIs were presented where appropriate. Cohen’s d (calculated with the averaged SD, dav) was used to assess the standardised treatment effect size between visit 1 and visit 2.10 A Cohen’s d value of <0.20 was considered no change, 0.20–0.49 was considered fair change, 0.50–0.79 was considered a medium change and ≥0.80 was considered a large change. All analysis was performed on SPSS V.22 and GraphPad Prism V.16.
Results
Patients
Of 42 patients who completed the study, 16 were incident and treatment-naïve and initiated PAH therapy, 12 were prevalent and underwent an escalation of therapy and 14 were stable on therapy with no change in treatment occurring between the study visits.(online supplemental table S5).
Test–test repeatability (visits 2 and 3)
In patients with PAH, test–test repeatability was assessed between visits 2 and 3; 6MWT (ICC 0.987) and log10NT-ProBNP (ICC 0.772) had excellent repeatability. Of cardiac MRI metrics (table 1), all showed excellent repeatability. Data for MRI pulmonary flow and perfusion transit times are shown in table 1.
Repeatability in all patients with PAH (ICC), and treatment effect size for patients with PAH initiating or escalating PAH therapy
Treatment effect size (visits 1 and 2)
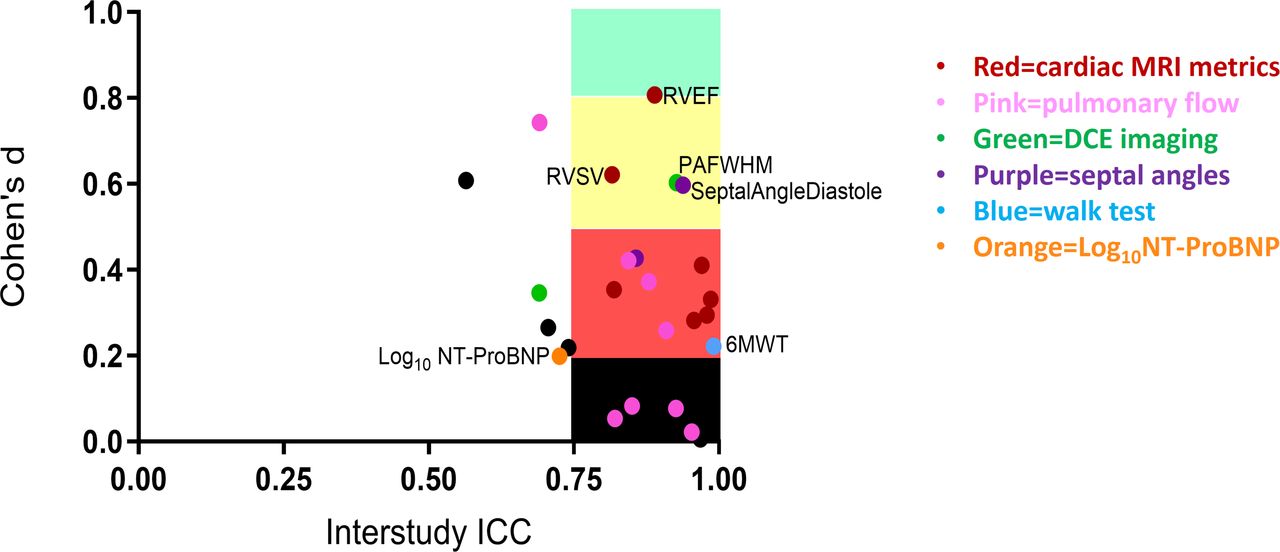
For all patients, initiating or escalating therapy (n=28), the only measurement with a large treatment effect size was RV ejection fraction (Cohen’s d 0.81). The 6MWT (Cohen’s d 0.22) and NT-ProBNP (Cohen’s d 0.20) demonstrated a fair treatment effect size (table 1). Figure 1 shows Cohen’s d values for the top three MRI end points, the 6MWT and NT-proBNP. Figure 2 shows ICC versus Cohen’s d value for all end points. In patients initiating PAH therapy, RV ejection fraction (Cohen’s d 0.99), diastolic septal angle (Cohen’s d 0.88) and peak pulmonary arterial flow velocity (Cohen’s d 0.92) had a large treatment effect size. In patients escalating therapy, RV ejection fraction, RV stroke volume and pulmonary arterial pulsatility had a medium effect size, whereas NT-ProBNP (Cohen’s d 0.02) and 6MWT (Cohen’s d 0.07) demonstrated no treatment effect (see online supplemental figure S4). The stable patient group showed either no or fair changes across all measured parameters (online supplemental table S6).
Supplemental material

Comparison of treatment effect size using Cohen’s d results in patients initiating and/or escalating pulmonary arterial hypertension (PAH) therapy. 6MWT, 6 min walk test; Log10NT-ProBNP, log to base 10 N-terminal pro-brain natriuretic peptide; RV, right ventricular.

{kind=link}
{kind=link}
Cohen’s d versus interstudy intraclass correlation coefficient (ICC) for study measurements. DCE, dynamic contrast-enhanced imaging; Log10NT-ProBNP, log to base 10 N-terminal pro-brain natriuretic peptide; PAFWHM, pulmonary arterial full width at half maximum; RVEF, right ventricular ejection fraction; RVSV, right ventricle stroke volume; 6MWT 6 min walk test. ICC >0.75=excellent repeatability. Cohen’s d value of <0.20 was considered no change, 0.20–0.49 was considered fair change, 0.50–0.79 was considered a medium change and ≥0.80 was considered a large change.
Discussion
Investigations used to monitor disease severity in patients with PAH, namely 6MWT distance, NT-ProBNP level and MRI metrics, had excellent repeatability. In contrast, only MRI (RVEF) demonstrated a large treatment effect size in patients initiating or escalating therapies, whereas for the 6MWT and NT-ProBNP the treatment effect sizes were fair.
As observed in previous clinical trials1 and highlighted at the 6th World Symposium,9 all metrics evaluated in patients with PAH escalating therapy had a lower treatment effect size compared with treatment-naïve patients initiating therapy. This represents a challenge when studying the effects of new therapies in PAH where the standard of care is combination treatment.1 Importantly, MRI was still able to detect a medium treatment effect size in patients receiving background PAH therapy. Due to the large cost of conducting PAH therapy trials, strategies to reduce the size of studies and their duration using a surrogate end point that is repeatable and has a large treatment effect size would be highly desirable.9
This study has a number of limitations including the small sample size and the lack of comparison with invasively measured pulmonary haemodynamics. Nonetheless, we have demonstrated in this exploratory study that MRI, the gold standard for RV function assessment, detects a larger treatment effect than the 6MWT or NT-proBNP. This may reflect the ceiling effect of the 6MWT and the effect of comorbidities (including chronic kidney disease) that may influence 6MWT distance and NT-proBNP levels. MRI metrics predict clinical worsening7 and mortality2–4 fulfilling many of the criteria of a surrogate end point.9 Given that pulmonary haemodynamics are commonly used in early phase PAH studies,1 a direct comparison of MRI metrics and pulmonary haemodynamics, to detect longitudinal change following PAH therapy, is now required if MRI imaging is to be considered a primary end-point for PAH therapy trials.8 9
This study demonstrates the high repeatability of MRI metrics in PAH and the large treatment effect size support further evaluation of MRI as a non-invasive endpoint in PAH therapy trials.
Ethics statements
Ethics approval
Ethical approval was obtained and patients provided written consent.
Acknowledgments
The authors would like to thank Elizabeth Berry for her help with study logistics, data analysis and manuscript quality checks, and for taking an active role on the steering committee. The authors would like to thank Amanda Creaser-Myers, Sara Walker, Kathryn Birchall and Mercy Korley for their assistance with the patient consenting process and taking blood samples. The authors would like to thank Jennifer Rodgers for help with database management and with administrative support. The authors would like to thank Dave Capener who acquired the MRI images for several of the cases. The authors would like to thank Charlie Elliot and Athaniosis Charalampopoulos for aiding study recruitment. The authors would like to thank Martin Brook for his help with MRI scan management. The authors would like to thank Jim Lithgow for his assistance with research governance approvals. The authors would like to thank the late Susie Fowles who was integral to the set up of the study, set up of the steering committee and had a major role in the development of the study protocol. Finally, the authors would also like to thank Carl Burgess, the patient representative, who actively contributed to the study design and execution through participation in the steering committee and also contributed expertise and practical assistance with data management.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was published Online First. Affiliations for FW and AC have been updated.
Contributors AJS, FW, JMW, AC, LK, DGK conceived the idea for the study. MC, MA, DGK, RC, AJS supported patient recruitment. AJS, JMW, DGK, AM, PH, LS devised the MRI protocol. AJC, CO, PH, LS analysed the MRI studies. FA, AM, CJ, PH, PG performed data quality control checks. MA performed the walk tests and FA, JP, AL performed the lab analyses. MC, LK, SA, AR, PG, AJS, YS, FS, PH, LS supported the data collation and analysis. Statistical analysis was performed by MC, SA, AJS, FA, LS, LK. All authors contributed to the drafting of the manuscript. All authors approved the final version of the manuscript.
Funding This study was funded by GlaxoSmithKline (contract number COL100041816) and Wellcome Trust (205188/Z/16/Z and 206632/Z/17/Z). PH is funded by a research grant from GlaxoSmithKline (BIDS3000032592).
Competing interests FW, LK and AC are employees and shareholders of GlaxoSmithKline. AS is the principal investigator for the collaborative research grant from GlaxoSmithKline that funded this study. AS has undertaken consultancy work for General Electric and Actelion Pharmaceuticals. RC has received fees for lecturing and participation in advisory boards, from Actelion, Bayer, GSK and MSD. DGK has received fees for lecturing and participation in advisory boards, from Actelion, Bayer, GSK and MSD and fees for participation in Steering Committees for Actelion.
Provenance and peer review Not commissioned; externally peer reviewed.