Article Text

Abstract
Exhaled breath analysis has the potential to provide valuable insight on the status of various metabolic pathways taking place in the lungs locally and other vital organs, via systemic circulation. For years, volatile organic compounds (VOCs) have been proposed as feasible alternative diagnostic and prognostic biomarkers for different respiratory pathologies.
We reviewed the currently published literature on the discovery of exhaled breath VOCs and their utilisation in various respiratory diseases
Key barriers in the development of clinical breath tests include the lack of unified consensus for breath collection and analysis and the complexity of understanding the relationship between the exhaled VOCs and the underlying metabolic pathways. We present a comprehensive overview, in light of published literature and our experience from coordinating a national breathomics centre, of the progress made to date and some of the key challenges in the field and ways to overcome them. We particularly focus on the relevance of breathomics to clinicians and the valuable insights it adds to diagnostics and disease monitoring.
Breathomics holds great promise and our findings merit further large-scale multicentre diagnostic studies using standardised protocols to help position this novel technology at the centre of respiratory disease diagnostics.
- exhaled airway markers
- respiratory infection
Statistics from Altmetric.com
Introduction
Respiratory diseases remain among the leading causes of death worldwide.1 By 2030, WHO estimates that respiratory illnesses will account for about one in five deaths worldwide.2
Early, rapid detection and treatment of lung diseases remain a priority, which would improve patient care and personalised therapy.3 For years, existing technologies like lung function tools and blood biomarkers have played an important role in diagnosing and monitoring lung diseases. However, there remains an unmet need for point-of-care respiratory-specific biomarkers that can aid in advancing precision medicine in both acute and stable respiratory diseases.
The lungs are almost unique owing to their ability to provide biological samples, direct from the organ with every breath. The ability to capture and analyse this sample type is highly attractive, as it allows direct non-invasive measurement of ongoing metabolic processes.
Breathomics, a branch of metabolomics studying exhaled breath, is a steadily evolving field that focuses on understanding the nature of volatile organic compounds (VOCs) and their health-related uses. VOCs can be leveraged as diagnostic biomarkers owing to their potential to mirror pathological processes taking place locally in the lungs and systematically, via the blood circulation.4 Additionally, they offer a non-invasive platform that is repeatable and potentially personalised, via ‘breathprint’ signatures.5 Despite years of clinical trials, technical and statistical challenges have delayed further translation of this technology to a real-world clinical setting.
In this state-of-the-art review, we examine the current evidence, analytical challenges and future considerations of exhaled breath analysis in respiratory diseases.
Data sources and search criteria
For the purpose of this narrative review, a systematic search was conducted using the following evidence databases: (1) PubMed, (2) Medline and (3) EMBASE. The keywords and mesh terms used to complete the search included: ‘asthma’, ‘volatile organic compound(s)’, ‘exhaled breath’, ‘VOC’, ‘VOCs’, ‘origin of VOCs’, ‘electronic nose’, ‘eNose’, ‘chronic obstructive pulmonary disease’, ‘respiratory infections’, ‘lung cancer’, ‘airflow limitation’, ‘Emphysema’ and ‘chronic bronchitis’.
Published peer-reviewed, full-text articles concerning clinical studies using VOCs in a diagnostic or disease monitoring capacity were assessed for eligibility. The following study types were included: observational studies, cross-sectional, case–control and cohort, and randomised controlled trials. The references lists of included studies were scrutinised to identify further relevant studies.
The studies were assessed based on their methodology and published results. Key findings from these studies are presented in the relevant sections.
Historical perspective of breath analysis
Utilisation of exhaled breath VOCs for disease diagnostics dates back to ancient Greek civilisations where breath was used to diagnose various illnesses. For example, the fruity smell of diabetic ketoacidosis and the fishy smell of liver illnesses.6–8 These elementary smell detection tests can be considered as the foundation of breath analysis.
The 20th century witnessed remarkable achievements in the field of breath testing, notably in 1971 Nobel Prize winner Linus Pauling presented a gas chromatogram showing separation of volatile substances from human breath, subsequently describing 250 components in exhaled breath.9 It was not, however, until the mid-eighties when Gordon et al demonstrated the feasibility of analysing exhaled breath VOCs in early diagnosis of lung cancer.10 This early association of VOCs and human disease formed the foundation for the current use of breathomics in early diagnosis and stratification of lung diseases.
In the following years, exhaled breath analysis gained increasing attention as a tool for diagnosing various illnesses. The specific pathways for these VOCs are not fully understood, nonetheless, profound progress has taken place with analytical technologies and detection capabilities.
Volatile organic compounds
Each exhaled breath contains thousands of VOCs; a heterogeneous group of carbon-based chemicals characterised by a high vapour pressure resulting from a low boiling point at room temperature.
Each breath cycle consists of different breath phases, and breath samples are often captured from the phase involved in gaseous exchange. This is also known as the ‘end expiratory phase’ or ‘alveolar breath’, excluding the dead space.11 12 This can be achieved using ‘gated sampling’, a process by which fractions of breath are collected based on measured parameters.
VOCs can originate from the external environment (exogenous) or from internal metabolic processes (endogenous) (figure 1). The presence of abundant exogenous compounds in breath samples (ie, environmental contamination) represents a fundamental challenge in breath research. Exogenous VOCs are continuously introduced into the respiratory system and owing to the complex kinetics of gas exchange, these can result in the production of volatile by-products, via various interactions with airway microbiota and mucosal lining.13

This figure highlights the complex kinetic of gaseous exchange. Endogenous VOCs can originate from the lungs or distant organs, via systemic circulation. Exogenous VOCs are continuously introduced into the respiratory system which can result in the production of volatile downstream products. Breath samples containing endogenous and exogenous VOCs are analysed to generate clinically meaningful data. GC-MS, gas chromatography mass spectrometry; VOCs, volatile organic compounds.
Removal of exogenous VOCs may simplify analysis, but loses potentially useful signals and requires additional processing steps. For example, limonene, a widely used food additive and fragrance for cosmetic or cleaning products,14 is present in higher levels in patients with liver cirrhosis and those with hepatic encephalopathy symptoms.15
In essence, exogenous VOCs and environmental contamination should be given special consideration when analysing exhaled breath VOCs for discovery studies; it continues to be an area of great uncertainty and larger multicentre studies validating environmental exposomes should be carried out.
Breath collection and storage
VOCs are found in trace levels (mainly in parts per trillion to parts per billion range) which poses considerable analytical challenge to operators.16 Current technologies allow for hundreds of VOCs to be detected in each exhaled breath sample.
Breath collection is a key step in this process and sub-optimal sampling can introduce contaminants, lose potential markers or alter the balance of breath patterns. As a result, considerable effort has been put into improving and standardising sampling and preconcentration steps.
Breath sampling can either be direct, usually with point-of-care analysis, known as ‘online’ sampling; or indirect, with breath stored for lab-based analysis, known as ‘offline’ sampling. In both, careful attention needs to be paid to the choice of sampling process and analytic platform.
Collection bags made of Tedlar, polytetrafluoroethylene (PTFE) or foil have been widely used as receptacles for breath sample storage. Bags are attractive as they are a convenient, inexpensive and are disposable for potentially infectious samples,17 however, potential drawbacks are (1) compound degradation within collection bags, particularly when samples remain mixed with water vapour and (2) compound interactions within the bag product. Additionally, Steeghs et al18 tested the compatibility of Tedlar bags and highlighted two abundant compounds contaminating bag contents. A reproducible compound loss was also detected both during bag filling and at a later stage following storage. Important considerations and suggestions for bag handling have been published.17
Various direct breath collection devices have emerged over the last few years.19–21 One example is the Respiration Collector for In Vitro Analysis breath sampler (Owlstone Medical, Cambridge, UK), which is a handheld, portable device, designed to collect breath directly onto sorbent tubes that are then transferred for analysis.22 The portability of such devices allow for breath collection at the patient’s bedside.
Sorbent tubes are commonly used for trapping and transporting VOCs from breath samplers to analytical devices, offering significant cost and logistical advantages.23 Sampling onto sorbent tubes is usually carried out using a calibrated pump where air is drawn through the tube at a constant rate and as the breath sample passes through the tube, compounds are collected on the absorbent inside.
A common concern with this method is that sorbents can retain moisture, given the high water vapour content in breath, which can negatively affect the quantitative capture of some analytes. In an attempt to overcome this problem, samples can be dry purged where a pure inert gas is passed through the sorbent tube to eliminate any additional trapped moisture while retaining analytes.24
VOCs are released from the tube for analysis using a process known as thermal desorption. Samples are heated to allow for sample extraction from the absorbent interior onto a pre-cooled trap, before further desorption into the analytical system. This offers numerous benefits including concentration enhancements, amplifying detection limits and eliminating unwanted analytical interferences.25
Other considerations when undergoing breath collection include the time of day. Wilkinson et al26 demonstrated a circadian variability in a proportion of exhaled VOCs over a 24-hour period with differential patterns of VOC release in asthmatics compared with healthy breath.
Breath analysis
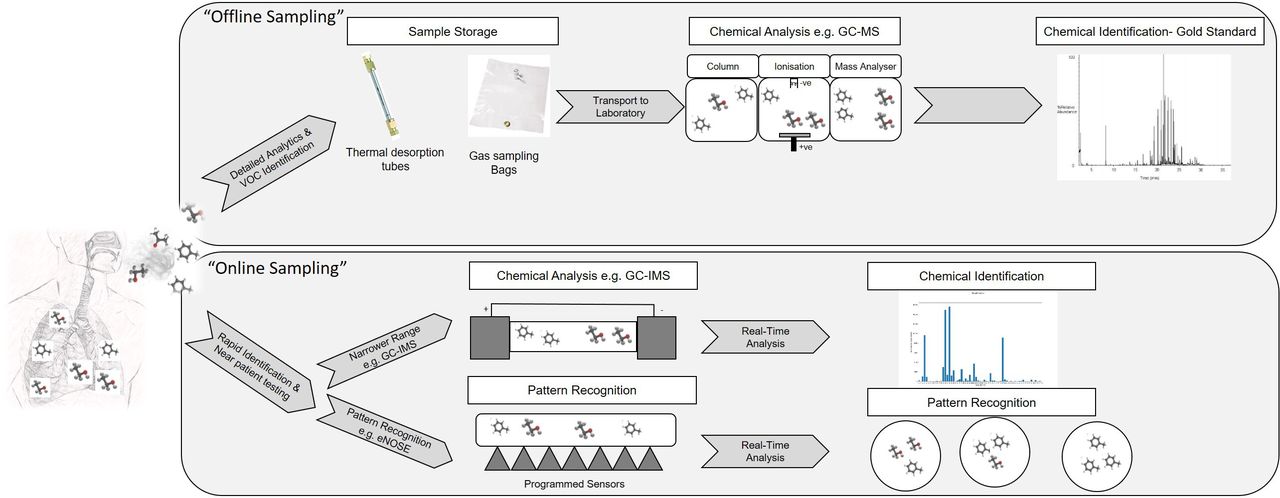
There are a number of technologies that can be used to analyse breath samples. Broadly these can be divided based on offline and online sampling techniques (figure 2).

{kind=link}
{kind=link}
Exhaled breath VOCs can be analysed using offline or online technologies. Offline technologies, currently considered gold standard, involve storing samples in a sorbent tube or collection bag prior to injecting them to an analytical instrument (eg, GC-MS). Online technologies involve direct introduction of breath samples to analytical instruments for analysis, negating the need for sample collection and storage. Online technologies require less analytical instrument time and technical skills and results can be obtained immediately, however, they lack the ability to identify compounds with high fidelity which limited its applications. GC-MS, gas chromatography mass spectrometry; VOCs, volatile organic compounds.
Offline technologies
Offline technologies are considered the gold standard techniques for breath analysis and include:
Gas chromatography mass spectrometry (GC-MS) is the the most common chromatographic technique, allowing for compound separation and identification based on both retention time and mass spectra matching.27 Gas chromatography comprises two main phases (1) the mobile phase: the vaporised sample is carried in an inert gas (eg, helium) at a predetermined speed which is then passed through a chromatographic column and (2) the stationary phase: compounds are separated based on the strength of interaction between the molecules and the column; with the time taken for it to pass through the column known as retention time. Despite being highly sensitive and reproducible, complex presample processing, prolonged analysis time and expert knowledge requirement has hampered its use in a wider clinical setting. A number of studies have emerged over the years using GC-MS to examine specific VOCs for lung pathologies,28–30 however, the lack of standardisation and methodological platforms limited further exploration of this technology in wider multicentre comparison studies.
Comprehensive two-dimensional GC-MS (GC ×GC MS) is a multidimensional gas chromatography technique where the addition of an extra column provides superior separation over conventional GC-MS.31 As the analytes elute from the primary column, they are modulated onto a secondary column. This shorter secondary column leads to further separation allowing peaks with similar volatility, which could not be separated adequately with one-dimensional chromatography, to be separated by another mechanism. This is particularly helpful in complex matrices like breath samples.31–33 As the technique is more advanced, it has a higher initial capital cost compared with traditional GC-MS and requires more specialist skills to operate.
Online technologies
Online technologies involve direct introduction of breath samples into analytical instruments for analysis, negating the need for sample storage. As online technologies often require less analytical time results can be obtained immediately and, owing to their portability, they offer a potential for point of care testing. However, this means any chromatographic separation and analytical detector are often simplified, reducing the ability to identify compounds with high fidelity. This, and the lack of data processing parameters, limits its applications to proof-of-concept benchmarking studies and validation studies.34
Common examples of these technologies include:
GC ion mobility spectrometry
First described by McDaniel in the 1950s, ion mobility spectrometry (IMS) is an analytical technique that separates and identifies ionised molecules in the gas phase based on their mobility in a carrier buffer gas,35 it can detect VOCs down to ultratrace levels (ng/l to pg/l range) without the need for pre-concentration, visualising VOCs in a 3D IMS chromatogram. Without identifying individual chemical components, IMS recognises peak patterns that can be used for disease recognition. Its simplicity and easy patient interface allowed its utilisation in few studies in the last decade.36–39
Proton-transfer-reaction mass spectrometry (PTR-MS): PTR-MS has the capability of real-time analysis: it is considered one of the fastest analytical techniques with a typical time resolution of <100 ms. VOCs are ionised by transferring a proton from the reagent ion, hydronium, to any molecules with a suitable proton affinity, which are then separated in the mass spectrometer. Despite its speed the lack of pre-concentration can limit sensitivity and the absence of chromatographic separation limits its ability to definitively identify compounds compared with GC-MS.
Electronic nose technology
Loosely mimicking human olfaction, electronic noses (eNose) are made of multiple array sensors programmed to recognise different odours and comparing them to preprogramed patterns.40 Array sensors convert chemical input (breath samples) into electrical signals.41 eNoses do not contribute to individual compound identification, instead disease separation occurs through recognition of different breath profiles, also known as ‘breath prints’ or ‘breath signatures’ using pattern recognition algorithms.
Unlike GC-MS, analysis eNoses do not require highly skilled operators, and has a relatively quick operational time (results within minutes), with lower technical costs. Its readily implementable nature makes it more suited for point of care clinical testing compared with other offline technologies.7 However, there are some disadvantages compared with mass spectroscopy, mainly the inability to identify named compounds in complex mixtures, making it impossible to link back to metabolic processes and mechanistic pathways.42 Additionally, the breath signatures are highly influenced by environmental factors and water vapour, so considered to be less rigorous.7
Several diagnostic studies have been carried out using eNoses in airway disease43–46 and lung cancer47–49 with good discriminatory power. Furthermore, Plaza et al50 described the ability of breath signatures in stratifying different phenotypes of asthma based on their sputum granulocytic count.
As described, eNose technology has the potential to make a powerful screening tool for various pulmonary diseases. Further largescale pragmatic clinical trials are required to further validate this. The limited sensor stability, inability to calibrate and the difficulty in mass generating identical sensors have hindered further translation of this technology to a real-world clinical setting.
Headspace analysis
Headspace refers to the volume of gas directly above and in contact with a biological sample. Headspace has been used as a VOC source for a number of solid and liquid samples. For headspace analysis purposes, samples are usually kept within sealed glass vials that are either heated or air is driven over them to stimulate VOC release out of samples. Once stabilised, the gas within the vial is then collected or directly transferred to instruments for analysis.
Although still in the early stages of development, headspace analysis has been used to investigate compounds from bacteria implicated in ventilator-associated pneumonia51 and the identification of more specific organisms such as Escherichia coli, Pseudomonas aeruginosa and Aspergillus fumigatus,52–54 with promising results.
In vitro breath analysis adds to the growing body of evidence supporting the use of headspace VOC analysis in clinical practice, however, it faces many challenges including sample degradation requiring standardised protocols for sample storage and treatment.
VOCs in respiratory disease
Exhaled breath of healthy individuals contains a wide range of VOCs at varying concentrations. These compounds include, but are not limited to, hydrocarbons, ketones, aldehydes and alcohols.55 A breakdown of the various functional groups and their structure formulas are highlighted in (online supplemental table 1). The content and concentrations of these VOCs vary depending on the underlying metabolomic pathways during health and disease states as well as environmental interferences.
Supplemental material
It was not until advanced analytical techniques were introduced in the 1990s that a complete set of human breath profile had emerged for the first time.56 Hydrocarbons were one of the first discovered compounds in human breath, dating back to 1963 Ram Chandra and Spencer reported unexpected ethylene levels in exhaled human breath that were not thought to be solely attributable to gut flora.57 This was later believed to be associated to disease state when small chain hydrocarbons, which were thought to be a direct result of lipid peroxidation, were identified in exhaled breath.58
Exhaled breath VOCs analysis has been utilised in a variety of respiratory conditions, including:
Airway diseases
Asthma and chronic obstructive pulmonary disease (COPD) are two of the most common respiratory diseases affecting millions of people.59 The utilisation of VOCs in airways disease is promising, although to date there are no definitive diagnostic breath signatures for either disease to aid disease classification. Numerous studies have evaluated the use of exhaled VOCs in diagnosing and phenotyping airways diseases, with the most commonly identified compounds belonging to carbonyl-containing groups (ie, aldehydes, esters and ketones) and hydrocarbons (ie, alkanes, alkenes and monoaromatics).60–62
In one of the largest exhaled breath studies in asthma, Schleich et al63 were able to successfully classify 521 asthmatic patients into three groups based on their sputum granulocytic cell count, potentially offering surrogate biomarkers for eosinophilic and neutrophilic asthma.
Exhaled breath VOCs have been shown to successfully separate asthma and COPD,64 65 breath signatures using eNoses have been shown to do the same based on clinical and inflammatory characteristics rather than disease diagnosis.66
Basanta et al67 investigated the relationship between exhaled breath VOCs and existing indices of inflammation and described in great detail the ability of GC-ToF-MS in discriminating patients with COPD based on inflammatory cells into eosinophilic and neutrophilic subgroups, this particularly relevant in precision medicine and assessment of treatment response .
Exhaled breath analysis shows a promise in enhancing our knowledge of the pathogenic pathways driving airway diseases. The use of VOCs as stratification biomarkers in this diverse patient population has the potential to transform the care we offer. Further progression towards a real-world clinical translation will highly depend on the implementation of large-scale, well-powered, multicentre clinical studies.
VOCs in respiratory infections
The treatment of microbial respiratory infections is an obvious target for breathomics, as early and accurate identification of causative organisms can be challenging, particularly in patients with severe infections.68 Micro-organisms produce a wide variety of volatile metabolites, which can be released in the stable state or when the cell is disrupted in cases of infection69–71; these volatiles can serve as a biological marker of microbial presence and have the potential to enhance the diagnostic process, improving clinical outcomes.72
The presence of distinct VOC profiles in pneumonia has been demonstrated by multiple studies,73–75 however, none have established sufficient granularity to accurately diagnose pneumonia based on a single breath test. A systematic review by van Oort et al76 outlined nitric oxide (NO), among others, as a potential diagnostic biomarker; though this is thought to be less specific as various other respiratory conditions drive altered NO bioactivity during disease state.77
Boots et al78 examined two hundred samples of bacterial headspace (defined as the area of gas directly surrounding a sample) from four different microorganisms (E. coli, P. aeruginosa, Staphylococcus aureus and Klebsiella pneumoniae) and demonstrated a highly significant difference in VOC occurrence of different bacterial cultures, Additionally, they demonstrated separation between methicillin-resistant and methicillin-sensitive isolates of S. aureus potentially translating to a valuable diagnostic tool in medical microbiology.
There is an urgent unmet need for a rapid and accurate test to diagnose tuberculosis, owing to the high diagnostic delay.79 80 Breath analysis has the potential to diagnose TB with moderate accuracy81 through the detection of specific VOCs produced by Mycobacteria,82 83 however, implementing VOCs as standard diagnostic tools will require further developments.
Cystic fibrosis (CF) is a growing area of interest in respiratory medicine, several studies have examined the role of exhaled breath VOCs in CF patients; Kramer et al84 demonstrated a proof-of-concept approach to using exhaled VOCs for the rapid identification of infectious agents in CF patients with lower respiratory tract infections.
The 2-aminoacetophenone (2-AA) was assessed for its specificity to P. aeruginosa in 29 CF patients and its suitability as a potential breath biomarker using GC-MS.85 The 2-AA was detected in a significantly higher proportion of subjects colonised with P. aeruginosa (93.7%) than both the healthy controls (29%) and CF patients not colonised with P. aeruginosa (30.7%) indicating that (2-AA) is potentially a promising breath biomarker for colonisation.
Breath analysis has the potential to be positioned in both the diagnostic and therapeutic work flows of respiratory infections, guiding early diagnosis and judicious antimicrobial use.
VOCs in lung cancer
Lung cancer has a poor prognosis, mostly due to the lack of symptoms and late presentation. While screening with CT has been introduced, the ability to diagnose through breath would likely lead to significant clinical impact, with considerably less radiation exposure to patients.86
Metabolic changes within cancer cells can lead to significant changes in volatile breath profile.87 Over the years, this has been explored as a potential avenue for early detection and diagnosis of lung cancer.88–91
One of the first studies to use VOCs in lung cancer was carried out by Gordon et al10, they reported a GC-MS profile of exhaled breath profile of 12 samples from lung cancer patients and 17 control samples with almost complete differentiation between the two groups.
Bajtarevic et al89 expanded on this to include an additional analytical instrument, using both PTR-MS and solid phase microextraction with subsequent GCMS, with a larger sample size (220 lung cancer patients at different stages of illness and 441 healthy volunteers), they reported that the three main compounds appearing in everybody’s exhaled breath (isoprene, acetone and methanol) were found at a slightly lower concentration in lung cancer patients compared with healthy volunteers using PTR-MS, additionally, the sensitivity of detection of lung cancer volatiles in breath based on the presence of four different compounds was only 52%, going up to 71% when including 15 compounds. The compounds identified were mainly alcohols, aldehydes, ketones and hydrocarbons.
Dragonieri et al48 adopted a different approach by using eNose and was able to discriminate breath profiles of 30 subjects with non-small cell lung cancer from patients with COPD and healthy volunteers, with modest accuracy.
The aforementioned studies have formed the foundation for large scale clinical trials evaluating the use of exhaled breath VOCs in patients with a clinical suspicion of lung cancer.92 Further results of large scale trials are eagerly anticipated.
VOCs in other respiratory conditions
Exhaled breath VOCs have been used in various other respiratory illnesses, nearly 90% of 25 patients with Pneumoconiosis were discriminated by their breath profile (receiver operator characteristic area under the curve (ROC-AUC) 0.88).93
Several studies examined the role of exhaled VOCs in interstitial lung disease (ILD), Yamada et al39 described five characteristic VOCs in the exhaled breath of IPF patients, using multicapillary column IMS. Of the five VOCs, four were identified as p-cymene, acetoin, isoprene and ethylbenzene. Further work in ILD was carried out using IMS, which seems to be a promising technique in discriminating patients with ILD from healthy controls.94 eNose sensors were used in patients with obstructive sleep apnoea, breath prints changed dramatically after a single-night continuous positive airways pressume (CPAP) and changes conformed to two well-distinguished patterns indicating that exhaled breath prints can potentially qualify as a surrogate index of response to and compliance with CPAP.95
The most clinically relevant volatile compounds are listed in (online supplemental table 2) along with the corresponding analytical technologies and reported concentration changes.
Supplemental material
Clinical implementation
The non-invasive nature, low patient burden and ability to directly sample from the target organ, makes the adoption of breathomics in real-world clinical practice an attractive prospect. However, clinical implementation has proved more challenging. The majority of reported breath studies so far have been small in size, single-centred and with no external validation. Nonetheless, several papers have assessed the feasibility of breath sampling in various clinical settings, including outpatient clinics,61 96 acute admission units,97 98 and intensive care units,74 99 with promising results.
External validation of breath biomarkers in independent populations is considered instrumental as it produces reliable predictions that can be reproduced in other clinical settings. The lack of external validation has created significant reporting challenges. From our review, there is little overlap between biomarkers reported by various groups which can be partially explained by the differences in methodology and reporting tools. The first step towards establishing a breathomics platform in clinical settings would be to regulate practices, including agreed common standardised operating procedures for breath collection, storage and analysis.
Clinical implementation of breathomics is thought to be particularly relevant amidst the ongoing COVID-19 pandemic. SARS-CoV-2 infection has been reported to cause a multitude of symptoms that affect several organs and systematic metabolism resulting in altered volatile metabolite distribution. Additionally, the rapid detection of COVID-19 specific VOC panel is thought to be particularly rewarding if tuned to assess the negative predictive value; this can be used to screen large populations (eg, airports, schools) as a first line test in ruling-out rather than ruling-in test, and to determine which individuals need further testing. This will enable rapid decision making as well as provide complementary information that will strengthen disease diagnostics.
Challenges and future considerations
Current analytical technologies have demonstrated an innovative ability to separate and detect a wide range of exhaled breath VOCs, however, the implementation of these techniques in a real world clinical setting faces considerable chemical and analytical barriers. One of the major unresolved challenges is that of environmental contamination and their interference with exhaled breath VOCs, there is still no unified consensus on how to tackle this issue; as relevant as it is to subtract environmental VOCs,100 it is crucial to take all molecular breath interactions into consideration when generating a diagnostic breath matrix. Standardised protocols should be instated for breath collection, analysis and reporting to guide future studies and allow a transparent analytical comparability across sites.
The availability of multiple analytical platforms with contrasting performance measures adds to the complexity of standardising biomarker discovery protocols. The choice of technology comes down to device availability and study budget, however, discovery studies are carried out using devices with the ability to separate and detect compounds with higher sensitivity and established robustness like (GC-MS). Although considered gold standard, GC-MS devices are considered highly complex for the non-experienced and are time consuming, making them less desirable in a real-world clinical setting. Sensor array-based technologies are much easier to use but are usually spared for when studies are aiming to distinguish between breath profile without the need for named compounds.
Analysis of breath matrices is highly complex, the combination of large variables and a relatively small sample size has led to various analytical challenges, the the most common being that of ‘overfitting’. With overfitting, usually owing to a limited sample size, the whole dataset is used to train and validate discovery prediction models, as opposed to having separate discovery and replication datasets, this results in a falsely optimistic models that can’t be generalised to the entire population. Ideally, this is overcome by training prediction models in a distinct dataset that is separate to and independent from the validation dataset, currently considered the gold standard method.101 102
Exhaled breath biomarkers are envisaged to have a crucial role as point-of-care tests in emergency departments and primary care clinics, however, to our knowledge no major studies have been completed in these settings. To date, biomarker discovery studies have mostly been small in size and confined to single centres. With few exceptions,103–105 the majority of the published breath discovery studies have been carried out in the stable disease state or at an outpatient clinic level. Further large-scale trials targeting acute disease states are required to properly evaluate the reliability of these breath tests and to formally assess the replicability in a real-world clinical setting.
Exhaled VOCs can provide valuable insight into the metabolic processes in the human body beyond the lungs, this can further expand our understanding of the common respiratory metabolic traits, translating into improved patient-centred diagnostics and therapeutic measures. Only when the aforementioned challenges are addressed, can the value of breath technology be fully appreciated.
Conclusion
Exhaled breath analysis possesses an inherit appeal that has been explored by scientists and clinicians for many decades. The lack of consistency in trial outcomes among other challenges have hindered faster translation of this technology into a real-world clinical setting. Considerable effort has been invested over the last few years to address these issues but exhaled breath analysis is still far from clinical implementation. In this state-of-the-art review, we presented a comprehensive critique of the published literature and highlighted some of the key challenges and ways to overcome them.
Looking at the current state of the field compared with where it was 10 years ago predicts an encouraging future for exhaled breath analysis that can potentially revolutionise healthcare and point-of-care diagnostics.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the entire EMBER team for supporting this project. The following respondents opted to have their name acknowledged: Ananga Sundari, Beverley Hargadon, Sheila Jones, Bharti Patel, Asia Awal, Rachael Phillips, Teresa McNally, Clare Foxon, (University Hospitals of Leicester). Dr Matthew Richardson, Professor Toru Suzuki, Professor Leong L Ng, Dr Erol Gaillard, Dr Caroline Beardsmore, Professor Tim Coates, Dr Robert C Free, Dr Bo Zhao, Rosa Peltrini, Luke Bryant (University of Leicester). Dorota Ruszkiewicz (Loughborough University)
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Greening_COPD
Collaborators EMBER Consortium. Ananga Sundari; Beverley Hargadon; Sheila Jones; Bharti Patel; Asia Awal; Rachael Phillips; Teresa McNally; Clare Foxon; Dr. Matthew Richardson; Prof. Toru Suzuki; Prof. Leong L Ng; Dr. Erol Gaillard; Dr. Caroline Beardsmore; Prof. Tim Coates; Dr. Robert C Free; Dr. Bo Zhao; Rosa Peltrini; Luke Bryant; Dorota Ruszkiewicz;
Contributors WI and NG conceived the presented review. WI took the lead in writing the manuscript with support from NG and LC. All authors, including RC, MJW, DS, PSM, PT, CB and SS contributed to the writing, reviewing and editing of the manuscript.
Funding This review was funded by the Medical Research Council (MRC), Engineering and Physical Sciences Research Council (EPSRC) Stratified Medicine Grant for Molecular Pathology Nodes (Grant No. MR/N005880/1) and Midlands Asthma and Allergy Research Association (MAARA), supported by the NIHR Leicester Biomedical Research Centre and the NIHR Leicester Clinical Research Facility. NG is funded by an NIHR Fellowship (pdf-2017-10-052).
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves