Article Text

Statistics from Altmetric.com
TM
A 45-year-old Caucasian woman was referred for investigation of recurrent chest infections. She had been treated over the previous 9 months for recurrent symptoms characterised by intermittent episodes of dyspnoea, cough productive of green sputum and pleuritic chest pain. Systemic enquiry was unremarkable; specifically, she had not experienced any weight loss or anorexia.
On each episode, oxygen saturations were >94% and heart rate was <100 beats/min, with a single occurrence of a low-grade fever (37.8°C). The white cell count peaked at 10.59×108 (neutrophils 8.82, eosinophils 0.18, lymphocytes 0.89), and her C reactive protein remained consistently within normal lab ranges. She was not anaemic. Liver, kidney and bone profiles were all within normal limits.
Each course of antibiotics would lead to transient improvement in cough, but the pleuritic chest pain and breathlessness remained unchanged.
EOB
Her medical history included myasthenia gravis (1991), neuromyelitis optica (2009), non-alcoholic steatosis, hypertension, obesity (body mass index 48.7 kg/m2), hypothyroidism and obstructive sleep apnoea. Surgical history included thymectomy (1993) and a gastric bypass (2010).
She worked in retail with no occupational exposures. She had never smoked and was teetotal. Her exercise tolerance had deteriorated over the preceding 12 months, from being unlimited to 50 m, due to a combination of dyspnoea and fatigue. She did not garden or tend soil, and had two cats in good health. She had no childhood respiratory illnesses. She lived with her young family in a suburban area and had no recent history of foreign travel. There was no personal or contact history of tuberculosis (TB).
Medications included prednisolone, mycophenolate, lamotrigine, topiramate, lisinopril, venlafaxine, levothyroxine, omeprazole and pregabalin.
Spirometry demonstrated an forced expiratory volume in 1 s of 1.9 litre (70% predicted) with forced vital capacity of 2.2 litre (72%predicted), similar to her results in the previous year. A contrast-enhanced CT scan of the thorax was arranged.
FVG
The CT showed dense consolidation in the middle lobe (ML) with associated patchy ground-glass opacity, nodularity and a tiny right pleural effusion (figure 1A). There was no underlying bronchiectasis. The consolidation was visible on the scout image and was not present on the normal chest radiograph in the previous 2 months. Given the predominantly infective clinical picture, it was felt appropriate to repeat a chest radiograph at 6 weeks, following antibiotic therapy.
{kind=link}
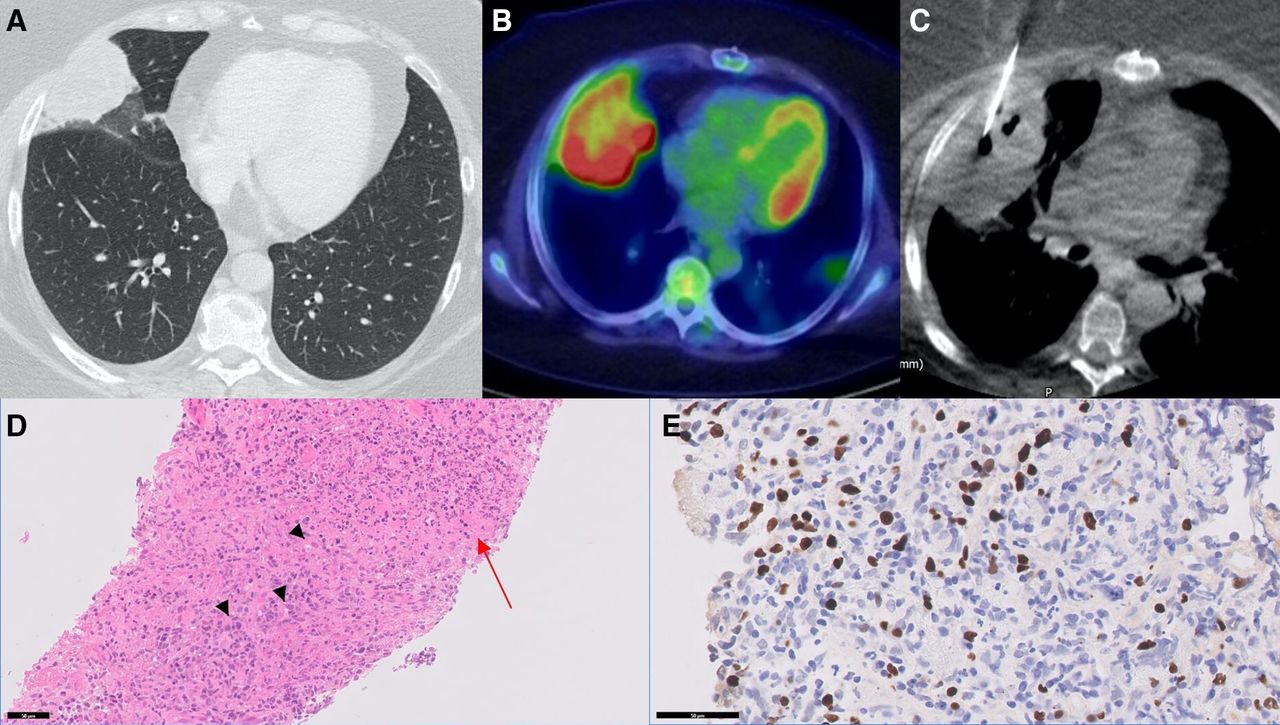
(A) Contrast-enhanced CT of the thorax (lung window) showing mass-like consolidation in the right ML with surrounding volume loss. (B) PET-CT scan showing extremely FDG-avid part necrotic mass-like consolidation in the right ML. (C) Four 18 G biopsy specimens were taken from the lateral/pleural as well the posterior aspect of the mass, which was seen to be avid on recent PET-CT. (D) Digital photomicrograph of the lung biopsy showing widespread infiltration by large atypical lymphocytes, associated with an infiltrative angiocentric pattern and extensive necrosis of the lung parenchyma in other areas. These cells were pan-cytokeratin negative, B-cell marker CD20 and CD79a positive on immunostaining and demonstrated a high proliferative rate on Mib-1 staining. Areas of haemorrhagic necrosis (red arrow) and a diffuse infiltrate of enlarged atypical lymphocytes (black arrowheads) (H&E, original magnification ×400). (E) Digital photomicrograph of the lung biopsy following EBER in situ hybridisation, showing brown nuclear staining on EBV+infected lymphocytes (counterstain haematoxylin, original magnification ×200). EBER, EBV-encoded RNA EBV, Epstein-Barr virus; FDG, fluorodeoxyglucose; ML, middle lobe; PET-CT, positron emission tomography–CT.
This showed persistent ML collapse, so a repeat contrast CT scan was arranged.
The CT now showed progression of the mass-like consolidation in the ML with a large area of non-enhancement within and mass effect on the surrounding lung suggesting malignancy. The surrounding bronchial wall thickening, ground-glass change and nodularity had completely resolved following treatment. The pleural effusion had slightly increased in size, but there was no pleural thickening, enhancement or nodularity. There was no significant abnormal thoracic, abdominal or pelvic lymphadenopathy.
NMR
At this stage, the differential included lung malignancy, but given the history of immunosuppression, atypical infections, including fungi and TB, were considered. Despite the history of myasthenia gravis, the prior thymectomy made a thymoma unlikely. Lymphoma and sarcoidosis were also in the differential, but the absence of classic radiological features such as lymphadenopathy, perifissural and bronchovascular nodularity made these less likely. Percutaneous ultrasound-guided lung biopsy was performed to exclude a rapidly progressive lung malignancy.
TM
Microbiological testing on the tissue biopsy, including gram and Ziehl-Neelsen staining, culture for fungi, mycobacteria and nocardia were all negative. Histopathological examination including immunostaining showed necrotic tissue only with no diagnostic features of malignancy. Special stains for fungi and mycobacteria were negative.
Following this negative biopsy, a bronchoscopy was performed. No endobronchial lesion was identified. Bronchoalveolar lavage (BAL) and brush samples from the ML were taken. The cultures isolated Aspergillus fumigatus and Streptococcus viridans. Mycobacterial culture was negative. The BAL fluid cytology showed abundant mixed inflammatory cells only, but the bronchial brush samples contained sheets of malignant cells with enlarged nuclei, prominent nucleoli and mitotic activity.
EOB
Given her symptom recurrence, rise in inflammatory markers and the microbiological isolates, the patient was admitted for intravenous antibiotics. A diagnostic aspirate of the left-sided pleural effusion was undertaken. The fluid was cloudy and straw-coloured, and biochemistry revealed pH 7.28, glucose 5.9 (serum glucose 6.0), protein 39 and LDH 465, going against pleural infection. Cytology showed scattered lymphocytes and macrophages with no malignant cells. Gram-stain and culture were negative. Three days into her admission, she was improving and was discharged to complete a 1-week course of intravenous antibiotics at home.
NMR
Almost 3 months into her investigation, the concern was that she had a progressing yet still undiagnosed malignancy. We proceeded to a PET-CT plus repeat guided lung biopsy. A full viral serology, immunoglobulin and autoimmune screen were also done. Aspergillus IgE and IgG were negative. The autoimmune screen and HIV serology were negative. Hepatitis C antibody, cytomegalovirus IgM, toxoplasma IgM and hepatitis B surface antigen were all negative. Epstein-Barr virus (EBV) IgG was positive. Given the diagnostic difficulty, we agreed that surgical lung biopsy would be indicated if repeat core biopsy of any fluorodeoxyglucose (FDG)-avid areas was non-diagnostic.
FVG
The PET-CT scan showed a further increase in size of the ML mass-like consolidation (maximum diameter 11 cm) with extensive FDG-avidity and a large area of central necrosis (figure 1B). There was a broad area of contact with the pleura but no evidence of chest wall invasion. A number of FDG-avid nodules were seen in the lower lobes and subpleural, right hilar and subcarinal regions. There were mildly FDG-avid small right hilar and subcarinal nodes.
MMcC/GDT
Histology of the second lung biopsy (figure 1D) showed a diffuse pleomorphic and high-grade lymphocytic infiltrate expanding and replacing the lung interstitium, accompanied by an angiodestructive pattern of necrosis. The cells had a raised proliferative rate on Mib-1 immunostaining. The infiltrate was diffusely immunopositive for the B-cell markers, CD20 and CD79a, with individual cells also CD30 positive on immunostaining, although no classical Hodgkin-Reed-Sternberg-like cells were seen. There was a dense background reactive CD3+ T cell and CD68+ histiocytic infiltrate. In situ hybridisation (EBV-encoded RNA (EBER)) for EBV (figure 1E) was strongly positive on a high proportion of the B cells, quantitated at >50 cells per high-powered field.
The features were those of a high-grade EBV+ve B-cell lymphoma within the lung, with the morphology and immunophenotype of lymphomatoid granulomatosis (LyG) (grade 3).
TM
The patient underwent six cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone chemotherapy for B-cell lymphoma. Maintenance therapy for neuromyelitis optica was switched from mycophenolate to rituximab. A restaging CT showed a mixed response. The ML mass became cystic with a small solid element, and there was persistent lymphadenopathy. The patient was deemed to be in a good partial remission. No further treatment was planned and she remained under regular review.
EOB
LyG is an angiocentric and angiodestructive lymphoproliferative disease composed of malignant B cells infected with the EBV virus, on a background of intermixed reactive T cells. It was first described by Liebow in 1972.1 It is a multicentric disease commonly associated with primary or secondary immunodeficiency states, predominantly involving the lung but also the skin, kidney and central nervous system. The median age of the patients is 46–48 years with male predominance (2:1). Fever, dyspnoea and cough are typical presenting features, sometimes including chest pain and weight loss.2 LyG is rare with an unknown prevalence, but it is usually progressive and fatal, with the largest studies indicating mortality rates ranging from 63% to 90% at 5 years.
Characteristic CT features include peribronchovascular distribution of nodules, coarse irregular opacities, small thin-walled cysts and conglomerating small nodules. Large masses (such as in our case) and occlusion of large vessels occasionally occur.3 Generally, the infiltrates in the lung are characteristically more patchy and variable than a solid high-grade B-cell lymphoma such as a diffuse large B-cell lymphoma (DLBCL). In cases presenting with typical peribronchovascular nodularity, histopathological examination shows that the nodules are caused by intravascular and perivascular infiltration by atypical lymphoid cells.
GDT
On this patient’s biopsy the infiltrate demonstrated several pathognomonic features of LyG with a pleomorphic lymphocytic infiltrate, expanding and distorting the alveolar walls, in an angiocentric and angiodestructive pattern associated with resultant necrosis.4 The malignant lymphoid cells were pleomorphic B cells, CD20/CD79a+ highly proliferative set in a dense background of reactive T cells and monocyte/histiocytes. They expressed variable CD30 (but not other markers of a Hodgkin’s disease infiltrate) and were EBV+ve on EBER in situ hybridisation. The grading is based on the number of EBV+ve cells and degree of cellular atypia and, in this case, was grade 3 due to abundant EBV, atypia and necrosis. LyG is one of a number of EBV+ lymphoproliferative disorders affecting the lung, such as EBV+ve DLBCL, Castleman’s disease or EBV+ve lymphoproliferative disorders in the post-transplant or immunocompromised patient.5
The workup of these cases is critically dependent on immunostaining, so obtaining a biopsy is essential for tissue and any subsequent fluorescence in situ hybridisation (FISH) analysis or PCR testing. These are difficult on scanty endobronchial brush specimens, even if they are EBV+ve, as the material is usually consumed in making the standard slides for cytological examination. Other cytological specimens, such as the pleural fluid in this case, can be used for immunostaining by spinning the specimen down and making a cell block, but biopsy remains the key for diagnosis.
EOB
The treatment strategy for LyG is usually chosen based on underlying immunosuppression, presence and severity of symptoms, extent of extrapulmonary involvement and histopathological grade. Patients on immunosuppressive medication should stop them, wherever possible. For low-grade LyG (grade 1 or 2), serial clinical reviews and chest CT are reasonable (approximately 20% achieve spontaneous remission). Symptomatic patients, those with more extensive disease, especially extrapulmonary involvement, should be referred to a haemato-oncologist for consideration of immunochemotherapy. In general, treatment options follow those for DLBCL. The clinical course is variable, ranging from indolent to progression to large B-cell lymphoma. In most aggressive cases, mean survival is approximately 18 months. In one large series, treatment of grade 3 disease resulted in progression-free survival of 44% (median follow-up 32 months).6
NMR
This was a difficult case to diagnose but highlights the importance of repeated assessment and imaging. In retrospect, the original consolidation had significant mass-like features in evolution, and it is not clear if the associated effusion was truly malignant or associated with an incidental infection.
The key investigation that advanced the case was the PET-CT scan, which allowed differentiation of the central necrotic area from the FDG-avid periphery, which was targeted for biopsy. In the presence of lack of response to treatment and progressive radiology, the case highlights the importance of a multidisciplinary team and liaison with fellow specialists. Although a rare diagnostic entity, representing less than 1% of non-Hodgkin’s lymphoma and approximately 0.5%–1.0% of primary pulmonary malignancies, pulmonary lymphoma (and its variants, including LyG) should be on the differential diagnosis of consolidation, which is lobar and not behaving in a clinically usual way for bacterial infection or inflammation (such as organising pneumonia), particularly when patients are on an immunosuppressive medication.
Footnotes
Twitter @BedawiEihab
Contributors EOB and NMR conceived the report. FVG reviewed the radiology. GDT and MMcC reviewed the histology. EOB, TM and GDT drafted the manuscript. All authors reviewed and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note The patient sadly passed away recently due to COVID-19. Written consent was kindly provided by their next of kin.