Article Text

Abstract
Background Vitamin D may regulate the innate immune system, and randomised controlled trials suggest a beneficial effect of vitamin D supplementation against acute respiratory tract infections. By using a Mendelian randomisation approach, we tested the hypothesis that low 25-hydroxyvitamin D is associated with increased risk of bacterial pneumonia in observational and genetic analyses.
Methods We genotyped 116 335 randomly chosen white Danes aged 20 to 100 from the Copenhagen City Heart Study and Copenhagen General Population Study for plasma 25-hydroxyvitamin D decreasing genetic variants around CYP2R1 (rs117913124, rs12794714 and rs10741657), DHCR7 (rs7944926 and rs11234027), GEMIN2 (rs2277458) and HAL (rs3819817). Information on plasma 25-hydroxyvitamin D was available on 35 833 individuals. Individuals were followed from 1981 through 2018 for hospital diagnoses of bacterial pneumonias.
Results During up to 38 years follow-up, we observed 6342 bacterial pneumonias in observational analyses and 13 916 in genetic analyses. In observational analyses, multivariable adjusted HR for bacterial pneumonias was 1.27 (95% CI: 1.16 to 1.40) for individuals with 25-hydroxyvitamin D<25 nmol/L compared with those with ≥25 nmol/L. In genetic analyses, the OR for bacterial pneumonia per 10 nmol/L lower plasma 25-hydroxyvitamin D was 1.12 (95% CI: 1.02 to 1.23) in Wald’s ratio, 1.12 (95% CI: 1.04 to 1.20) in inverse-variance weighted, 1.63 (95% CI: 0.96 to 2.78) in MR-Egger and 1.15 (95% CI: 1.05 to 1.26) in weighted median instrumental variable analysis. This association was strongest for genetic variants around CYP2R1. There was no observational or genetic evidence to support that 25-hydroxyvitamin D is associated with risk of urinary tract infections, skin infections, sepsis or gastroenteritis, which were used as negative control outcomes.
Conclusions Low vitamin D is associated observationally and genetically with increased risk of bacterial pneumonias.
- pneumonia
- clinical epidemiology
- respiratory infection
- bacterial infection
- innate immunity
Data availability statement
Data are available upon reasonable request. Additional data regarding technical details, statistical code and derivative data are available from the corresponding author. Data access for further analyses is possible through direct collaborative agreement or through locally managed access arranged through the study’s principal investigator.
Statistics from Altmetric.com
Key messages
What is the key question?
This study was designed to answer whether low plasma vitamin D is a causal factor in bacterial pneumonias by using a Mendelian randomisation approach.
What is the bottom line?
By using a Mendelian randomisation approach in two population-based cohorts with >110 000 individuals and up to 38 years of follow-up, low plasma vitamin D is associated observationally and genetically with increased risk of bacterial pneumonias, but not with risk of urinary tract infections, skin infections, sepsis or gastroenteritis.
Why read on?
This is the first study that investigates the causal association of vitamin D with bacterial pneumonias alone using genetic evidence.
Introduction
The proposed role of vitamin D in human health has been extended well beyond calcium and bone homoeostasis to now include regulation of the innate immune system.1 2 Accordingly, observational studies have found that low plasma 25-hydroxyvitamin D concentrations are associated with increased risk of respiratory tract infections in adults, children and infants.3–9 Nevertheless, randomised controlled trials investigating effect of vitamin D supplementation against respiratory tract infections have found conflicting results.10–23 However, a systematic review and meta-analysis comprising 11 321 participants and including all randomised controlled trials with vitamin D supplementation of any duration against acute respiratory tract infections showed a beneficial effect.24 To our knowledge, no study has attempted to investigate the causal association of vitamin D with bacterial pneumonias alone using genetic evidence.
A Mendelian randomisation analysis takes advantage of natural randomisation and uses genetic variants as proxies of modifiable exposures.25 Since alleles are randomly distributed at conception, genetic variants should not be associated with potential confounders, and since genes are present at birth, genetic analyses are not susceptible to reverse causation. Thus, causal inferences can be made using such a study design akin to randomised controlled trials. Indeed, genetic variants have been identified that specifically lead to lifelong lower plasma 25-hydroxyvitamin D concentrations,26–29 providing an ideal framework to assess low 25-hydroxyvitamin D as a causal risk factor for bacterial pneumonias. In such a Mendelian randomisation framework, instruments or genetic variants known to be associated with plasma 25-hydroxyvitamin D are tested for their association with bacterial pneumonia. From this, it may be possible to show that 25-hydroxyvitamin D is causal of bacterial pneumonia under a number of key assumptions. The assumptions are that the genetic variants are associated with 25-hydroxyvitamin D, are only associated with bacterial pneumonia through 25-hydroxyvitamin D and are independent of confounders of the association of plasma 25-hydroxyvitamin D with bacterial pneumonia.
By using a Mendelian randomisation approach, we tested the hypothesis that low 25-hydroxyvitamin D is associated with increased risk of bacterial pneumonia in observational and genetic analyses. For this purpose, we used two population-based cohorts with >110 000 individuals and up to 38 years of follow-up.
Methods
Study populations
The Copenhagen City Heart Study is a population-based prospective cohort study initiated in 1976 to 1978, with follow-up examinations in 1981 to 1983, 1991 to 1994 and 2001 to 2003.30 All individuals in Denmark are assigned a unique identification number at birth or immigration (Central Person Registration number) and recorded in the national Danish Civil Registration System. Individuals aged 20 to 100 were randomly selected and invited from the national Danish Civil Registration System to reflect the white adult general population of Danish descent (an individual is registered as of Danish descent in the national Danish Civil Registration System if the person and both parents are born in Denmark and have Danish citizenship). At study entry, all individuals completed a questionnaire, underwent a physical examination and gave blood for biochemical and genetic analyses (1991 to 1994 and 2001 to 2003 examinations only). In observational analyses, we included 10 272 individuals with plasma 25-hydroxyvitamin D measurements from the 1981 to 1983 examination. In genetic analyses, we included 9536 individuals from the 1991 to 1994 and/or 2001 to 2003 examinations with information on all genotypes. Of these, 5597 had information on both plasma 25-hydroxyvitamin D measurements and all genotypes.
The Copenhagen General Population Study is a population-based prospective cohort study initiated in 2003 with ongoing enrolment, recruited and examined as the Copenhagen City Heart Study but from different parts of Copenhagen.30 In observational analyses, we included 25 561 individuals, with plasma 25-hydroxyvitamin D measurements. In genetic analyses, we included 106 799 individuals with information on all genotypes. Of these, 25 410 had information on both plasma 25-hydroxyvitamin D measurements and all genotypes.
No individual appeared in more than one study. For the Copenhagen City Heart Study, the response-rate was 72% in the 1976 to 1978 examination, 63% in the 1981 to 1983 examination, 61% in the 1991 to 1994 examination and 50% in the 2001 to 2003 examination. Non-responders versus responders in the 1976 to 1978 examination were more often men (52% vs 46%) and slightly older (median age: 55 vs 54 years). Similar differences could be observed between non-responders and responders for the subsequent examinations: 53% vs 45% and 61 vs 58 years in the 1981 to 1983 examination, 45% vs 44% and 63 vs 61 years in the 1991 to 1994 examination and 43% vs 43% and 67 vs 62 years in the 2001 to 2003 examination, respectively. For the Copenhagen General Population Study recruiting in 2003 to 2015, response rate was 43%. Non-responders versus responders were more often men (48% vs 45%) and slightly younger (median age: 56 vs 58).
Plasma 25-hydroxyvitamin D measurements
Measurements of plasma 25-hydroxyvitamin D using the DiaSorin Liaison 25(OH)vitamin D Total Assay, a direct competitive chemiluminescence immunoassay, were conducted blind to information on outcome and genotypes.30 For the Copenhagen City Heart Study, plasma samples were collected in 1981 to 1983 (n=10 272) and stored at −20°C for approximately 30 years before measurement. For the Copenhagen General Population Study, plasma samples were either collected in 2004 to 2005 (n=12 506) and stored at −80°C for approximately 5 years before measurement or in 2009 to 2011 (n=13 055) for measurement on fresh samples. Assay precision was tested daily, while assay accuracy was tested monthly using an external quality control programme (Vitamin D External Quality Assessment Scheme (DEQAS)). The inter-assay coefficient of variance was 10% for low concentration control (∼40 nmol/L) and 8% for high concentration control (∼135 nmol/L).
Genotypes
Genotyping using TaqMan assays was conducted blind to information on outcome and plasma 25-hydroxyvitamin D concentrations.30 Specific genotypes for plasma 25-hydroxyvitamin D concentration were selected as those having the strongest and largest association in genome-wide association studies,26 29 we chose genetic variants around CYP2R1 (rs12794714 and rs10741657) and DHCR7 (rs7944926 and rs11234027), as they are expected to influence biologically active plasma 25-hydroxyvitamin D concentrations via either synthesis of pre-vitamin D from 7-dehydrocholesterol in the skin or conversion of vitamin D to 25-hydroxyvitamin D in the liver. We on purpose did not genotype for variants in the vitamin D binding protein, as such variants will influence the amount of 25-hydroxyvitamin D transported in plasma rather than differences in biologically active plasma 25-hydroxyvitamin D. Recently, three additional genotypes for plasma 25-hydroxyvitamin D concentration were identified in genome-wide association studies; a rare genetic variant located around CYP2R1 (rs117913124) and two frequent genetic variants around GEMIN2 (rs2277458) and HAL (rs3819817),27 28 which we also genotyped. Call rates were >99% after two reruns.
Bacterial pneumonias
Bacterial pneumonias (International Classification of Diseases (ICD)-8: 481xx to 486xx and ICD-10: A481, J13 to J16, J170, J18) were defined as acute emergency department visits and hospital admissions with the mentioned primary diagnosis. Information was obtained from the national Danish Patient Registry, which records all public and private hospital contacts in Denmark, recorded from baseline until 13 December 2018. Diagnoses recorded in the registry are made by medical doctors according to national law. Denmark used the ICD-8 until 1 January 1994 and proceeded directly to ICD-10 after this date. As negative control outcomes, we included urinary tract infections, skin infections, sepsis and gastroenteritis.31
By using the unique Central Person Registration number provided to everyone in Denmark at birth or immigration and linking it with the national Danish Patient Registry, no person was lost to follow-up, and individuals who emigrated were censored at the date of emigration (n=137 in observational analyses and n=538 in genetic analyses).
Potential confounders
Body mass index (BMI) was calculated as measured weight divided by measured height squared (kg/m2). Smoking status was defined as never, former or current smoking. Cumulated tobacco consumption was calculated in pack-years based on information on age at smoking initiation and cessation (or for current smokers until age at baseline examination), duration of tobacco consumption and amount of consumed tobacco in form of number of daily consumed cigarettes, cheroots and cigars and grams of weekly consumed pipe tobacco: a pack-year was defined as 20 cigarettes or equivalent smoked daily for a year. Alcohol consumption was self-reported in units per week (1 unit=12 g). Estimated glomerular filtration rate (eGFR) was calculated from serum creatinine measured using standard hospital assays. Chronic disease at baseline included diabetes mellitus, ischaemic heart disease, chronic obstructive pulmonary disease (COPD) and cancer. Diabetes at baseline was based on self-report, non-fasting plasma glucose >11 mmol/L, use of antidiabetic medication and/or previous inpatient/outpatient hospital contacts due to diabetes (ICD-8: 249 to 250 and ICD-10: E10 to E14), obtained from the national Danish Patient Registry. Ischaemic heart disease (ICD-8: 410 to 414 and ICD-10: I20 to I25) and COPD (ICD-8: 491 to 492 and ICD-10: J41 to J44) at baseline were based on inpatient/outpatient hospital contacts, obtained from the national Danish Patient Registry. Cancer at baseline, excluding non-melanoma skin cancer cases, was obtained from the national Danish Cancer Registry.
Statistical analyses
Deviation from Hardy-Weinberg equilibrium was investigated using the χ2-tests; deviation may suggest genotyping or population sampling errors, but we observed none. Associations with potential confounders were investigated using linear and logistic regression models, as appropriate. Associations between the genotypes and plasma 25-hydroxyvitamin D were investigated using linear regression models; we evaluated the strength of the genotypes as instruments by examining the F-statistic and R2: a high F and/or R2 indicates sufficient strength to ensure statistical reliability of the risk estimates.32 Kaplan-Meier estimator was used to determine cumulative prevalence of bacterial pneumonias with log-rank test. Cox proportional hazard models were used to determine risk of bacterial pneumonias. Multiple failure-time analysis was carried out to investigate risk of recurrent events using the method proposed by Andersen and Gill.33 Wald’s test was used to assess interaction on risk of bacterial pneumonias. We used age as the underlying timescale (=age adjusted) with left truncation (=delayed entry) at study examination. Observational analyses were adjusted for age, sex, seasonal variation of 25-hydroxyvitamin D (by adjusting for month and year of blood sampling), birth year, cohort, BMI, smoking status, cumulative tobacco consumption, alcohol consumption, eGFR and chronic disease at baseline (diabetes, ischaemic heart disease, COPD and cancer). Genetic analyses were adjusted for age, sex, birth year and cohort, as genetic analyses generally are not prone to confounding. In order to estimate the causal effect of plasma 25-hydroxyvitamin D on bacterial pneumonia, we used instrumental variable analysis with individual level data, accounting for partial overlap and methods designed to be robust to some violations of the assumptions for Mendelian randomisation analyses, that is, inverse-variance weighted, MR-Egger and weighted median estimators.34 35 All instrumental variable analyses were carried out using single events, that is, first event, as methodology for investigating recurrent events has not been developed yet. The causal effect was estimated by including genetic variants that were not prone to weak instrument bias (sufficiently high F-statistic and R2) in accordance with previous recommendations.32 36 However, instrumental variable analysis was repeated by also including all genetic variants. In a sensitivity analysis, we investigated the associations in the UK Biobank through GeneAtlas.37 38 However, UK Biobank had a different outcome definition (influenza and all pneumonia combined) from the one used in the present study, as bacterial pneumonia alone was not available. In another sensitivity analysis, we combined genetic variants around CYP2R1 to create unweighted and weighted genetic risk score, since most of the association seemed to be driven through these genotypes; only internal weighted risk scores could be calculated as genome-wide association studies did not report results necessary to calculate externally weighted risk score.26–29 Since information on potential confounders was 99.9% complete, we performed multivariate imputation using chained equations to fill out the missing values in the observational analyses; however, results were similar without the use of imputation. We used Stata/SE 13.1 for Windows.
Results
We had 35 833 individuals in observational analyses and 116 335 in genetic analyses (figure 1 and table 1). Plasma 25-hydroxyvitamin D concentrations were associated with all potential confounders (online supplemental table S1). In contrast, the genotypes for 25-hydroxyvitamin D were not associated with any potential confounders (online supplemental table S2) but as expected associated with plasma 25-hydroxyvitamin D concentrations in a dose-dependent manner (online supplemental figure S1), illustrating that such genotypes can be used as largely unconfounded instruments to assess the association of genetically determined low 25-hydroxyvitamin D with risk of bacterial pneumonias by using a Mendelian randomisation approach. Among the genotypes, GEMIN2 rs2277458 and HAL rs3819817 had F-statistic <10 and R2 <0.1%, suggesting that these genotypes may be weak instruments (online supplemental figure S1).
Supplemental material

Flowchart depicting samples used in observational and genetic analyses.
Potential confounders in observational and genetic analyses in individuals in the general population
In the Copenhagen City Heart Study, median follow-up was 21 years (up to 38 years) for the observational analyses and 18 years (up to 27 years) for the genetic analyses. In the Copenhagen General Population Study, corresponding values were 8.8 years (up to 14 years) and 9.3 years (up to 15 years), respectively. During follow-up, we observed 6342 bacterial pneumonias in the observational analyses and 13 916 in the genetic analyses.
Observational analyses
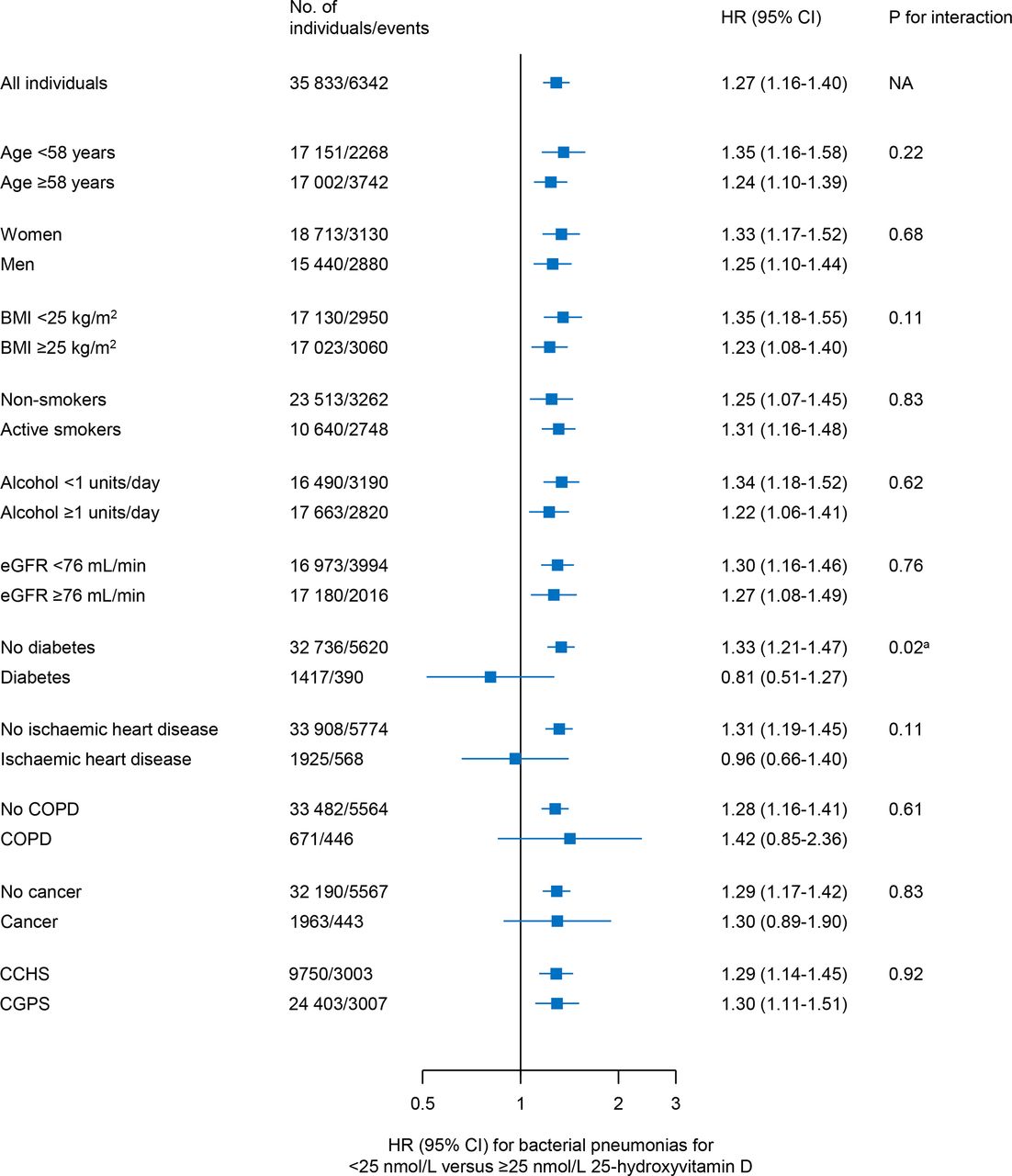
Individuals with 25-hydroxyvitamin D<25 nmol/L had an increased risk of bacterial pneumonias compared with those with 25-hydroxyvitamin D≥25 nmol/L in the Copenhagen City Heart Study and Copenhagen General Population Study, both in combined and separate analyses (figure 2). Compared with individuals with 25-hydroxyvitamin≥25 nmol/L, the multivariable adjusted HR for bacterial pneumonias was 1.27 (95% CI: 1.16 to 1.40) in individuals with 25-hydroxyvitamin D<25 nmol/L. This risk estimate was largely similar in subgroup analyses without evidence of interaction, including in the two studies separately (figure 3).

Cumulative prevalence and risk of bacterial pneumonias according to plasma 25-hydroxyvitamin D concentration in individuals in the general population. Cumulative prevalence from Kaplan-Meier estimator, and risk estimates obtained from Cox regression models with multiple failure-time analysis according to Andersen and Gill adjusted for age (as timescale), sex, seasonal variation of 25-hydroxyvitamin D, birth year, cohort, body mass index, smoking status, cumulative tobacco consumption, alcohol consumption, estimated glomerular filtration rate, chronic disease at baseline (diabetes, ischaemic heart disease, chronic obstructive pulmonary disease and cancer).
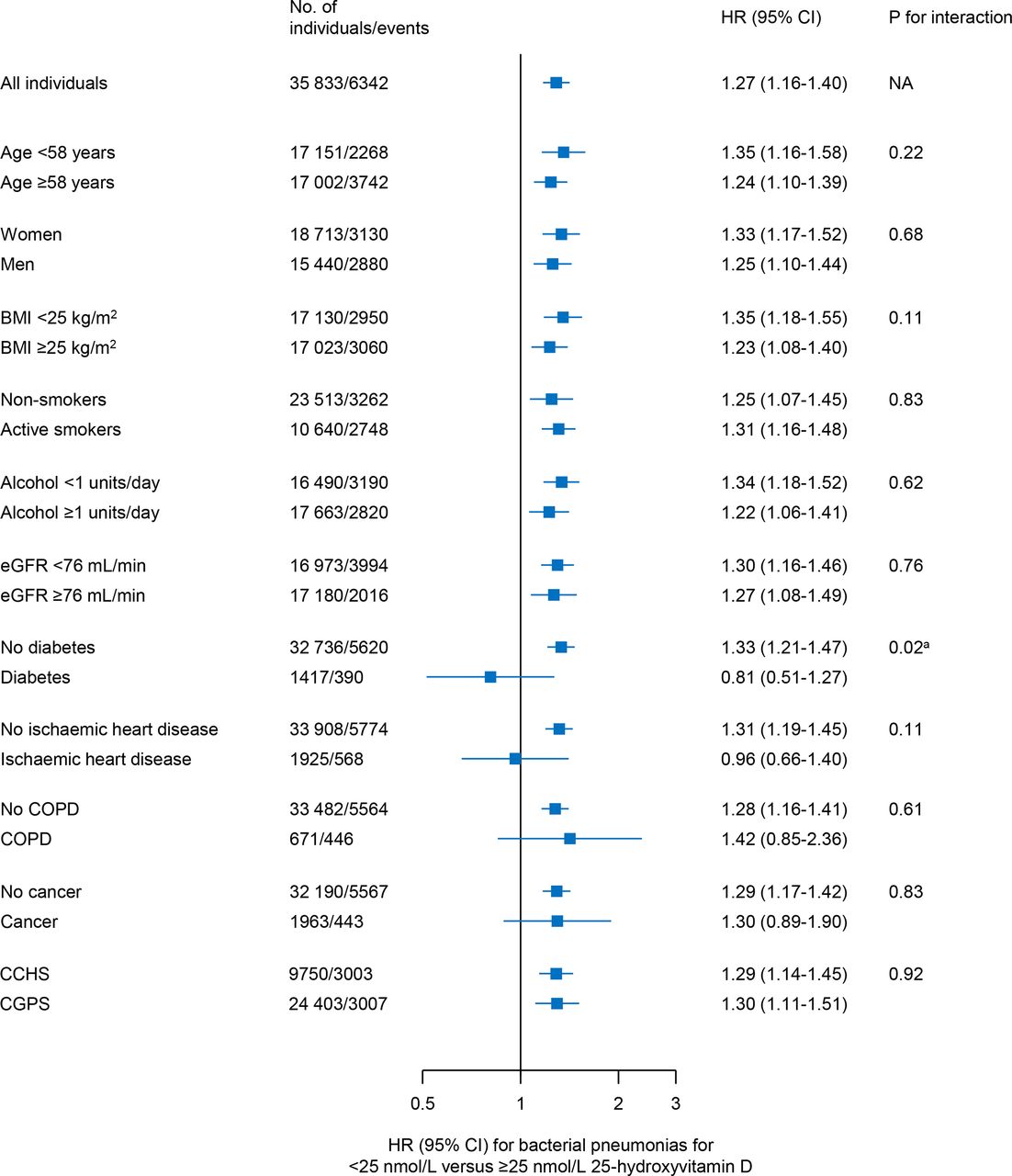
Risk of bacterial pneumonias in different subgroups according to plasma 25-hydroxyvitamin D concentration in individuals in the general population. Risk estimates obtained from Cox regression models with multiple failure-time analysis according to Andersen and Gill adjusted for age (as timescale), sex, seasonal variation of 25-hydroxyvitamin D, birth year, cohort, body mass index (BMI), smoking status, cumulative tobacco consumption, alcohol consumption, estimated glomerular filtration rate (eGFR), chronic disease at baseline (diabetes, ischaemic heart disease, chronic obstructive pulmonary disease (COPD) and and cancer), as appropriate. P for interaction obtained from Wald’s test. Number of individuals vary slightly in the subgroup analyses due to availability of data. Chosen cut-off values for age, BMI, alcohol and eGFR represent median values. Based on the Copenhagen City Heart Study (CCHS) and Copenhagen General Population Study (CGPS) if not otherwise stated. Risk estimates for the CCHS and CGPS vary slightly from figure 1, as complete case analysis has been used here.
Compared with individuals with 25-hydroxyvitamin≥50 nmol/L, multivariable adjusted HRs for bacterial pneumonias were 0.95 (95% CI: 0.88 to 1.103) in those with 25 to 49.9 nmol/L, 1.19 (95% CI: 1.06 to 1.32) in those with 12.5 to 24.9 nmol/L and 1.51 (95% CI: 1.25 to 1.81) in those with <12.5 nmol/L 25-hydroxyvitamin D (figure 4). No clear associations were observed between 25-hydroxyvitamin D concentrations and risk of urinary tract infections, skin infections, sepsis or gastroenteritis (all p values for trend ≥0.05); however, 95% CIs for HRs did not overlap with 1.0 in individuals with plasma 25-hydroxyvitamin D<12.5 nmol/L for skin infections and 12.5–24.9 nmol/L for sepsis.

Risk of bacterial pneumonias and other infections according to plasma 25-hydroxyvitamin D concentration in individuals in the general population. Risk estimates obtained from Cox regression models with multiple failure-time analysis according to Andersen and Gill adjusted for age (as timescale), sex, seasonal variation of 25-hydroxyvitamin D, birth year, cohort, body mass index, smoking status, cumulative tobacco consumption, alcohol consumption, estimated glomerular filtration rate, chronic disease at baseline (diabetes, ischaemic heart disease, chronic obstructive pulmonary disease and cancer). Based on the Copenhagen City Heart Study and Copenhagen General Population Study.
Genetic analyses
Each 25-hydroxyvitamin D decreasing allele in CYP2R1 rs12794714 and CYP2R1 rs10741657 was associated with higher risk of bacterial pneumonias but not of other infections (figure 5). Other genotypes were not associated individually with higher risk of bacterial pneumonias or other infections; however, individuals with genetic variation in GEMIN2 rs2277458 had a reduced risk of sepsis and gastroenteritis.
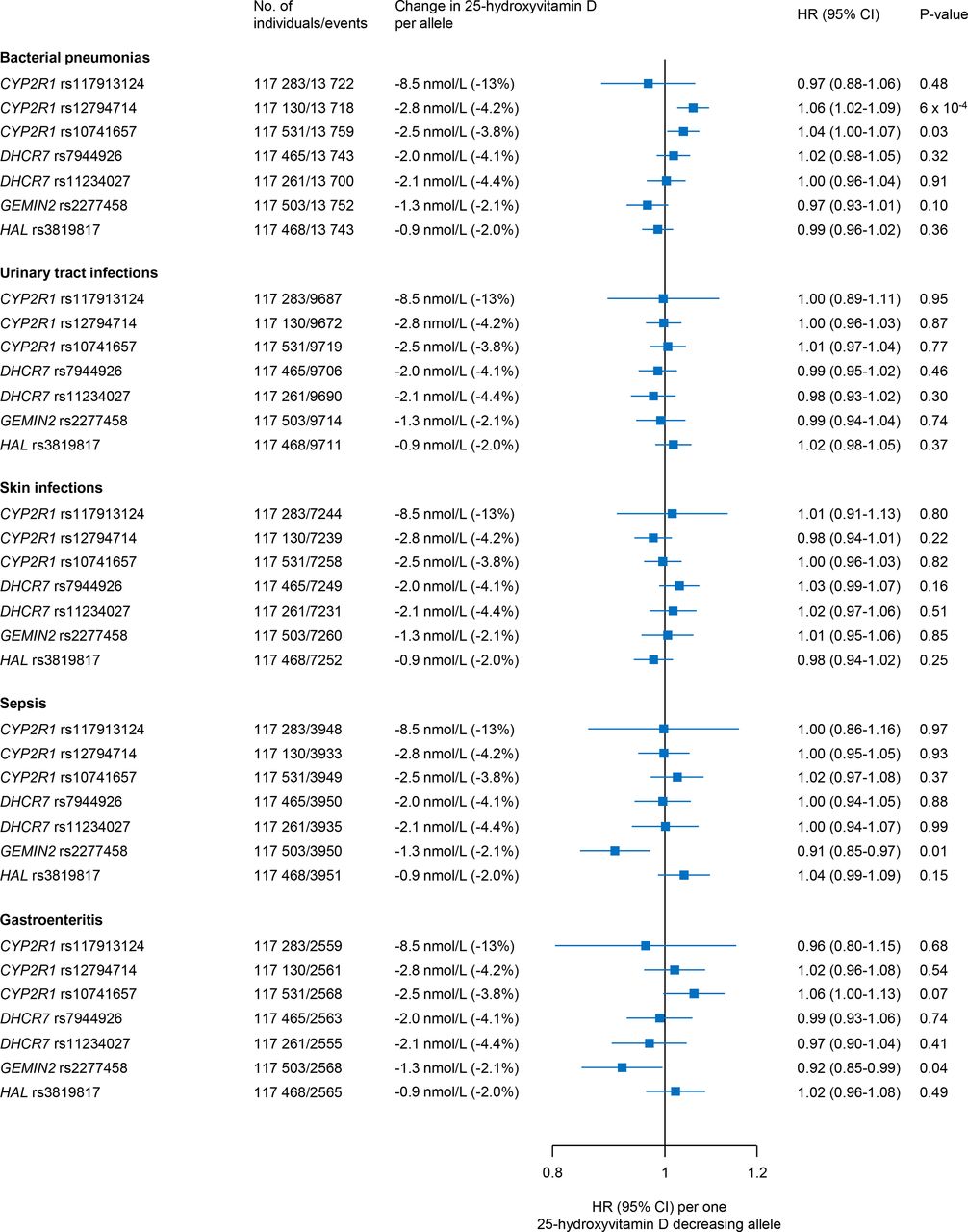
Risk of bacterial pneumonias and other infections according to 25-hydroxyvitamin D decreasing genotypes in individuals in the general population. Risk estimates obtained from Cox regression models with multiple failure-time analysis according to Andersen and Gill adjusted for age (as timescale), sex, birth year and cohort. Based on the Copenhagen City Heart Study and Copenhagen General Population Study.
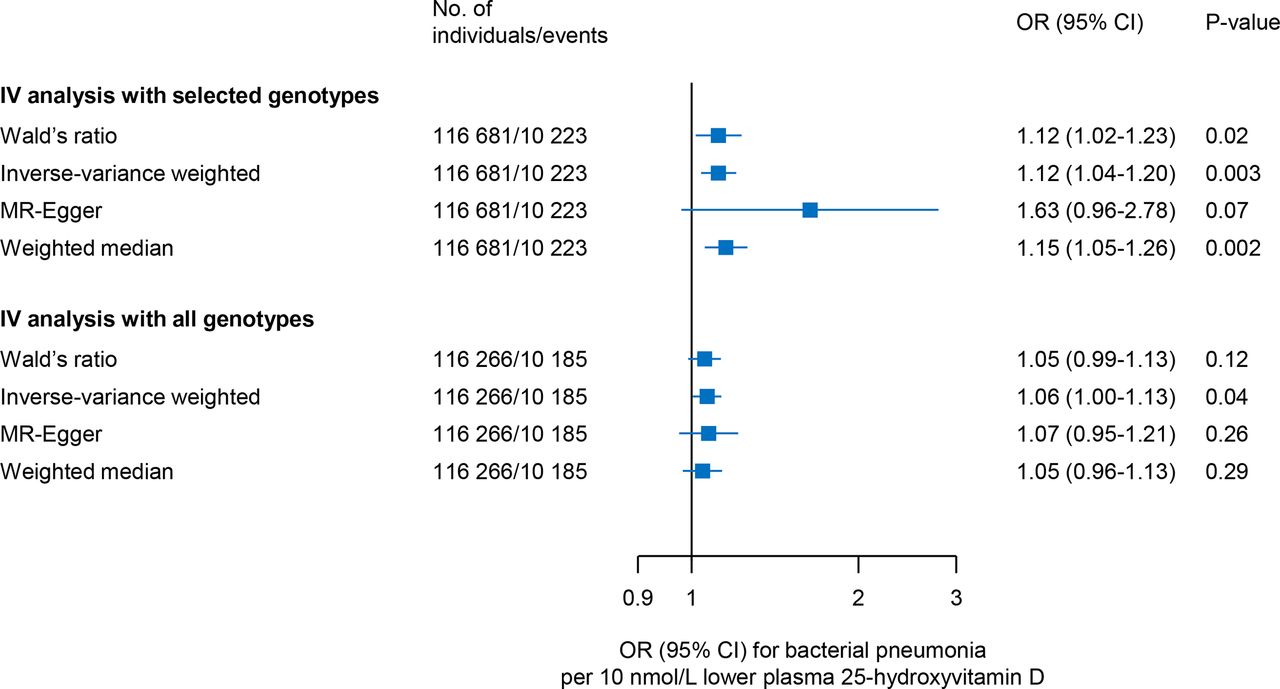
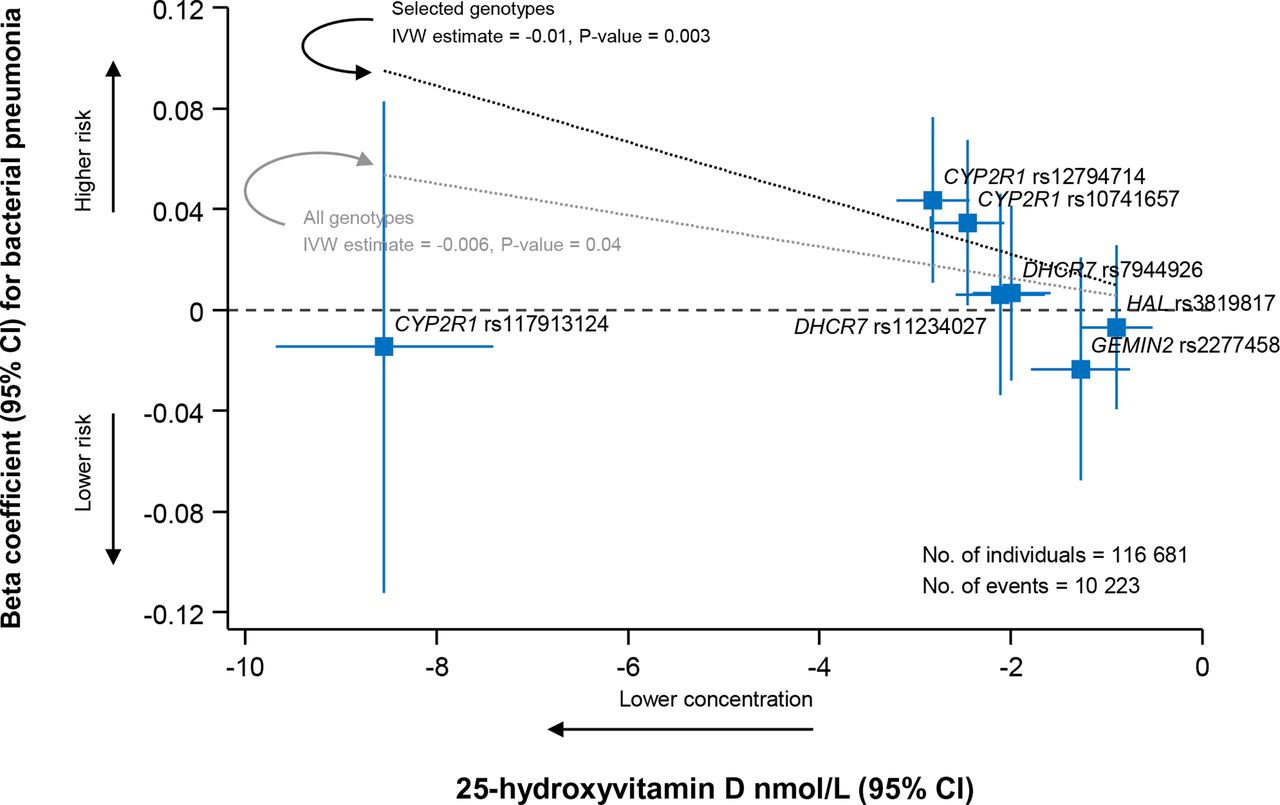
In instrumental variable analysis, lower plasma 25-hydroxyvitamin D concentration was associated with higher risk of bacterial pneumonia (figures 6 and 7). ORs for bacterial pneumonia per 10 nmol/L lower plasma 25-hydroxyvitamin D were respectively 1.12 (95% CI: 1.02 to 1.23) in Wald’s ratio, 1.12 (95% CI: 1.04 to 1.20) in inverse-variance weighted, 1.63 (95% CI: 0.96 to 2.78) in MR-Egger and 1.15 (95% CI: 1.05 to 1.26) in weighted median instrumental variable analysis (figure 7, upper panel). Results were attenuated but similar when also including the rare genetic variant, that is, CYP2R1 rs117913124, and the genetic variants prone to weak instrument bias, that is, GEMIN2 rs2277458 and HAL rs3819817 (figure 7, lower panel). However, these latter analyses may be biassed as outliers affect inverse-variance weighted and MR-Egger estimates, and weak instruments can also bias estimates in general, though usually towards the observational estimate.

Beta coefficient for bacterial pneumonia and change in plasma 25-hydroxyvitamin D concentration D according to 25-hydroxyvitamin D decreasing genotypes in individuals in the general population. Beta coefficients for bacterial pneumonia obtained from logistic regression models adjusted for age, sex, birth year and cohort. Change in plasma 25-hydroxyvitamin D concentration obtained from multiple linear regression models adjusted for age, sex, seasonal variation of 25-hydroxyvitamin D, birth year and cohort. Dashed black (selected genotypes) and grey (all genotypes) lines obtained from inverse-variance weighted (IVW) instrumental variable analysis. Selected genotypes included CYP2R1 rs12794714, CYP2R1 rs10741657, DHCR7 rs7944926 and DHCR7 rs11234027. Based on the Copenhagen City Heart Study and Copenhagen General Population Study.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of bacterial pneumonia according to 25-hydroxyvitamin D concentration using instrumental variable analysis in individuals in the general population. Risk estimates for bacterial pneumonia obtained from logistic regression models adjusted for age, sex, birth year and cohort. Change in plasma 25-hydroxyvitamin D concentration obtained from multiple linear regression models adjusted for age, sex, seasonal variation of 25-hydroxyvitamin D, birth year and cohort. Selected genotypes included CYP2R1 rs12794714, CYP2R1 rs10741657, DHCR7 rs7944926 and DHCR7 rs11234027. Based on the Copenhagen City Heart Study and Copenhagen General Population Study. IV, instrumental variable.
Sensitivity analyses
None of the 25-hydroxyvitamin D decreasing genotypes were associated with risk of influenza and all pneumonia combined in the UK Biobank, and estimates were attenuated for the Copenhagen City Heart Study and Copenhagen General Population Study compared with bacterial pneumonia alone (online supplemental figure S2); however, the CYP2R1 rs12794714 genotype was associated with increased risk of influenza and all pneumonia in the Copenhagen City Heart Study and Copenhagen General Population Study (latter also as a separate cohort). However, this outcomes definition is different from our main analyses as UK Biobank estimates could not be attained for bacterial pneumonia alone.
Since we suspected that the increased risk of bacterial pneumonia was probably driven through CYP2R1, we combined all available genetic variants around CYP2R1 (rs117913124, rs12794714 and rs10741657) in a genetic risk score. HR per 1,25-hydroxyvitamin D decreasing CYP2R1 risk score for bacterial pneumonias was 1.03 (95% CI: 1.01 to 1.04) in an unweighted genetic risk score and 1.01 (95% CI: 1.00 to 1.02) in a weighted genetic risk score (online supplemental figure S3).
Discussion
By using a Mendelian randomisation approach in two population-based cohorts with >110 000 individuals and up to 38 years of follow-up, we found that low plasma vitamin D is associated observationally and genetically with increased risk of bacterial pneumonias. There was no convincing evidence observationally or genetically that vitamin D is associated with risk of urinary tract infections, skin infections, sepsis or gastroenteritis.
Vitamin D seems to regulate the innate immune system, which is essential in the defence against bacterial pneumonias.2 It has been shown that toll-like receptor (TLR)−2/1 ligand, T-cell-derived interferon-gamma (IFN-γ) and T-cell-expressed CD40 ligand induce upregulation of vitamin D receptor (VDR) and 25-hydroxyvitamin D-1-α-hydroxylase (CYP27B1) (enzyme that converts inactive 25-hydroxyvitamin D to active 1,25-hydroxyvitamin D) through an autocrine pathway in human monocytes and macrophages.39–43 VDR and 1,25-hydroxyvitamin D then induce upregulation of cathelicidin-related antimicrobial peptides, that is, LL-37 and hCAP-18, and human β-defensin 2, autophagy and phagosome maturation, which ultimately leads to intracellular killing of pathogens, as shown for Mycobacterium tuberculosis, Pseudomonas aeruginosa and Bordetella bronchiseptica.39–44
Interestingly, genetic variants around CYP2R1 but not around DHCR7, GEMIN2 or HAL were associated individually with increased risk of bacterial pneumonias. A potential explanation may be that CYP2R1 is more directly involved in the formation of 1,25-hydroxyvitamin D compared with the other genes. Also, while the role of DHCR7 in vitamin D metabolism is well-established (conversion of 7-dehydrocholesterol to cholesterol), the role of GEMIN2 and HAL is unknown. This may also explain the low F-statistic and R2 of genetic variants around GEMIN2 and HAL compared with genetic variants around CYP2R1 and DHCR7. Also, we cannot exclude that variants in these genes may only indirectly affect 25-hydroxyvitamin D through pathways affecting both exposure an outcome separately (pleiotropy). Further, we cannot exclude the possibility that vitamin D may not be involved in the defence against bacterial pneumonias, and that other mechanisms involving CYP2R1 may be at play. Finally, the association of genetic variants around CYP2R1 with risk of bacterial pneumonias could represent a chance finding and therefore needs independent confirmation.
We were unable to replicate our findings in the UK Biobank. A potential explanation may be that a different outcome was used, that is, influenza and all pneumonia combined instead of bacterial pneumonia alone. Although we found evidence of an association with influenza and all pneumonia for the 25-hydroxyvitamin D decreasing CYP2R1 rs12794714 genotype, we believe that this association was probably driven by bacterial pneumonia. Another potential explanation may be that events were identified differently in the UK Biobank and the validity of these endpoints in UK biobank is unknown. Information on events in the present study was obtained from the national Danish Patient Registry, which records all public and private hospital contacts in Denmark, where diagnoses are made by medical doctors according to national law. In addition, events were only defined as acute emergency department visits and hospital admissions based on the primary diagnosis to increase the validity,45 and to secure that we only captured the most serious cases admitted to hospital in the Copenhagen cohorts.
Previous observational studies have found an association of low plasma 25-hydroxyvitamin D concentrations with higher risk of respiratory tract infections.3–9 Although results from randomised controlled trials testing the effect of vitamin D supplementation against respiratory tract infections have been conflicting,10–23 the largest systematic review and meta-analysis to date has pointed at a beneficial effect.24 In the present study, we show that low vitamin D is associated with increased risk of bacterial pneumonias in observational analyses and in part in genetic analyses. The fact that there was no evidence observationally or genetically that vitamin D is associated with risk of other organ specific infections suggests that the association could be specific for respiratory infections such as bacterial pneumonias. Future randomised controlled trials should therefore be designed to study the effect of vitamin D supplementation against bacterial pneumonias.
Strengths of the present study include two large-scale independent cohorts from the general population with randomly selected individuals with a long follow-up time, no losses to follow-up and a substantial number of bacterial pneumonias. Furthermore, we used physician encoded diagnoses with high validity.46
Potential limitations in Mendelian randomisation analyses include population stratification bias, genetic pleiotropy and linkage disequilibrium. However, as we had an ethnically homogeneous white Danish population, the complicating effects of population stratification were likely avoided, and as genotype distributions did not appear to differ according to the Hardy-Weinberg equilibrium, genotyping and population sampling errors were also likely avoided.
Another potential limitation is that we did not have information on family relationships, which could bias our results. However, since we have sampled randomly, we believe that this bias will be of minor importance.
As mentioned above, we cannot exclude that our positive genetic observation could not represent a chance finding. However, it is reassuring that all different instrumental variable analyses that were used to estimate the causal effect, each with its belonging strengths and weaknesses,34 gave similar results, suggesting that the results are robust.
In conclusion, low vitamin D is associated observationally and genetically with increased risk of bacterial pneumonias.
Data availability statement
Data are available upon reasonable request. Additional data regarding technical details, statistical code and derivative data are available from the corresponding author. Data access for further analyses is possible through direct collaborative agreement or through locally managed access arranged through the study’s principal investigator.
Ethics statements
Ethics approval
Both studies were approved by Danish ethical committees and conducted according to the Declaration of Helsinki (approval numbers: KF-V-100-2039/91 and H-KF-01-144/01). All individuals provided written informed consent.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators NA.
Contributors YÇ and SA had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analyses. YÇ, BGN and SA contributed to the study concept and design. YÇ, BGN and SA collected, analysed or interpreted the data. YÇ wrote the draft manuscript and did the statistical analyses. YÇ, BGN and SA revised the manuscript for important intellectual content. BGN obtained funding. BGN provided administrative, technical or material support. BGN and SA supervised the study.
Funding The Lundbeck Foundation. The funding source had no role in the design and conduct of the study; collection, management, analysis or interpretation of the data; preparation, review or approval of the manuscript; or decision to submit the manuscript for publication.
Competing interests YÇ reports personal fees from Boehringer Ingelheim, AstraZeneca, Sanofi Genzyme outside the submitted work. BGN and SA have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.