Article Text

Abstract
An increasing observation is that some patients with COVID-19 have normal lung compliance but significant hypoxaemia different from typical acute respiratory distress syndrome (ARDS). We hypothesised that changes in pulmonary blood distribution may be partially responsible and used functional respiratory imaging on CT scans to calculate pulmonary blood volume. We found that patients with COVID-19 had significantly reduced blood volume in the smaller calibre blood vessels (here defined as <5 mm2 cross-sectional area) compared with matched ARDS patients and healthy controls. This suggests that using high levels of PEEP may not alone be enough to oxygenate these patients and that additional management strategies may be needed.
- critical care
- ARDS
- imaging/CT
- MRI
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The COVID-19 pandemic has resulted in a proportion of patients progressing to respiratory failure and needing mechanical ventilation.1 This has caused significant challenges worldwide with both hospital ventilatory capacity and ventilation strategies for individual patients. Conventional wisdom for the management of acute respiratory distress syndrome (ARDS) involves use of mechanical ventilation with high levels of positive end-expiratory pressure (PEEP) to recruit lungs by exerting mechanical pressure on alveoli and compressing leaky capillaries located within the interstitial space.2 This use of high PEEP reduces the right-to-left shunt and allows the inspired fraction of oxygenation to become effective at oxygenating the blood.
However, there is an increasing observation that some patients with COVID-19 present with respiratory failure with a significant hypoxaemia but retain preserved lung function with normal compliance, which is different to typical ARDS.3 The mechanisms of this are not understood, but a number of groups have hypothesised that an abnormal vascular response may be responsible. We investigated this further by applying a novel method of image analysis to investigate the blood volume and distribution within the lungs of these patients.
Functional respiratory imaging (FRI) creates 3D reconstructions of the airways and pulmonary vasculature from CT scans to calculate both airway size and blood volume in the pulmonary circulation.4 5 Smoking-related chronic obstructive pulmonary disease has been characterised by distal pruning of small blood vessels, the magnitude of which change predicts the clinical severity of disease.4 Studies have shown that computer modelling of blood volume within the lungs is a strong correlate to histological markers of vascular change.6
Methods
We used FRI coupled with an automated blood vessel segmentation algorithm to perform an eigenvalue analysis of the Hessian matrix to enhance and identify tubular structures, returning the probability of each voxel belonging to tubular structure based on shape analysis. To account for effects of CT slice thickness on results, sensitivity analysis was performed. Volumes of blood were computed from the cross-sectional area of each blood vessel with <5 mm2 defined as small vessels (BV5) and >10 mm2 as large vessels (BV10), as previously defined by others.6 To account for differences in lung volume between individuals, we calculated blood volume within a vessel as a percentage of total blood volume through the lungs of each patient.
We performed FRI on CT scans from 10 intubated patients with COVID-19 (9 taken at initiation of venous–venous extracorporeal membrane circulation (VV-ECMO)) from a tertiary UK lung centre and compared them with data from 7 intubated patients without COVID-19 ARDS and a retrospective set of 107 healthy volunteers. The study was approved by the Royal Papworth R and D committee (ref. S02467). Patients with COVID-19 had scans taken at a PEEP of 10 cmH2O; patients with ARDS had scans taken at PEEP 0 and 20 (figure 1). All group comparisons were made using Kruskal-Wallis test; between-group comparisons were calculated using Mann-Whitney test. Statistical analysis was performed with R V.3.6.1 (R Foundation for Statistical Computing, Vienna, Austria).

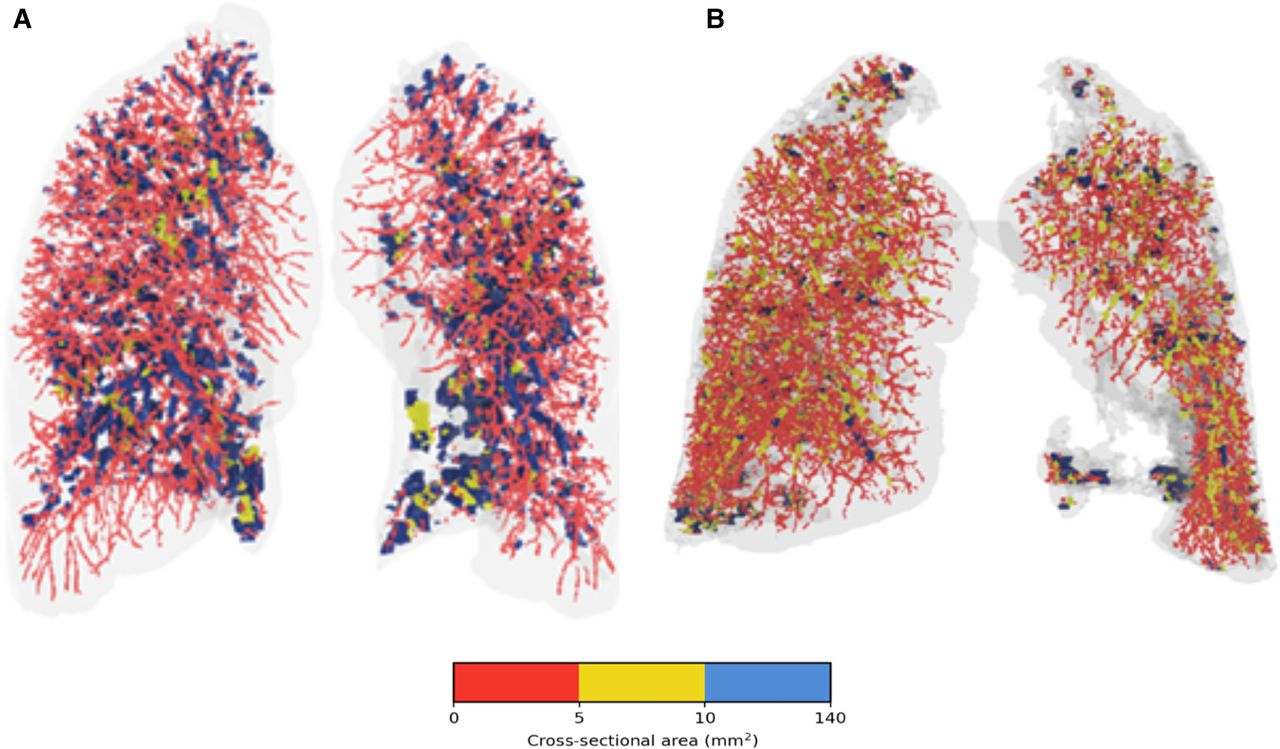
(A) Vascular blood flow through a patient with COVID-19. (B) Vascular blood flow through a patient with ARDS. Colours indicate vessel cross-sectional area. ARDS, acute respiratory distress syndrome.
Results
The groups were matched in terms of age, sex, height and premorbidity. The patients with COVID-19 had a higher body mass index (median 31, range 28.4–35.1) than patients with ARDS (median 26, range 24.8–28.4) (p=0.015). The FRI results showed that the distribution of blood volume was different between groups (figures 2 and 3). Patients with COVID-19 had significantly less total blood within small-calibre pulmonary blood vessels (BV5, defined as those with a cross-sectional area of <5 mm2) compared with ARDS and healthy controls (p=0.005, COVID-19 vs ARDS PEEP0; p=0.005, COVID-19 vs ARDS PEEP20; p<0.001, COVID-19 vs healthy). Conversely, they had a significantly higher proportion of blood volume within large-calibre vessels (BV10, cross-sectional area of >10 mm2) (p=0.007 COVID-19 vs ARDS PEEP0, p=0.009 COVID-19 vs ARDS PEEP20, p<0.001 COVID-19 vs healthy). Blood pressure, arterial pH and right ventricular function in the COVID-19 group were within normal parameters. Total pulmonary blood volume was similar between all groups.

Total amount of blood flow through all blood vessels as measured by cross-sectional area (0–20 mm2). (B) Total amount of blood flow through all blood vessels as measured by cross-sectional area (0–100 mm2). Patients with COVID-19 had scans taken at PEEP 10 cmH2O, ARDS at PEEP 20 cmH2O. ARDS, acute respiratory distress syndrome.

{kind=link}
{kind=link}
{kind=link}
(A) Box-and-whisker plot showing study groups and corresponding fraction of blood volume in vessels with cross-sectional area of <5 mm2. (B) Box-and-whisker plot showing study groups and corresponding fraction of blood volume in vessels with cross-sectional area of >10 mm2. ARDS, acute respiratory distress syndrome; BV5, blood vessel volume for vessels less than 5 mm2; BV10, blood vessel volume for vessels more than 10 mm2; TBV, total blood vessel volume. Mann-Whitney test was used for all between-group comparisons.
Discussion
Our findings suggest that the impaired gas exchange seen in COVID-19 may be partially a result of redistribution of blood away from the small-calibre pulmonary vessels. The mechanisms of this could be increased vascular resistance due to either vasoconstriction of distal pulmonary arteries or presence of microthrombi or both. Patients with COVID-19 have a high incidence of thrombotic complications with 31% from one large Dutch intensive care unit study having complications, including acute pulmonary embolism, deep-vein thrombosis and ischaemic stroke.7 Postmortem studies reveal frequent pulmonary microthrombi despite anticoagulation.8 More recently, a spectrum of vascular inflammation similar to Kawasaki disease has been reported as a late sequelae in some children.9
The main limitations of this study are the small numbers of patients investigated and that patients with COVID-19 had scans taken at initiation of VV-ECMO and may therefore have had a worse spectrum of lung disease compared with the ARDS group. However, given that cardiac indices in the COVID-19 group (as measured at the time of CT scan) was within normal parameters and total pulmonary blood volume (as measured by FRI) was not different between groups, it suggests an intrinsic difference in blood distribution which is not related to either cardiac function or total amount of blood within the pulmonary vessels. Interestingly, we did not find a difference in pulmonary blood distribution between patients with ARDS and healthy volunteers. There is no clear evidence for small vessel abnormalities in standard ARDS where a lung infection causing alveolar damage is the primary driver of hypoxaemia, but it may also be that our ARDS sample size was not large enough to identify these.
Our findings are consistent with a recent postmortem study which found that alveolar microthrombi were present at nine times the burden in COVID-19 compared with a matched ARDS group. The pattern of damage in both lungs was consistent with diffuse alveolar damage and perivascular T-cell infiltration. However, the COVID-19 group showed small blood vessels with structurally deformed capillaries which were elongated and displayed sudden changes in calibre with the presence of intussusceptive pillars.10 This suggests histologically a disorder in the small blood vessels, a finding confirmed by our radiology analysis. Our data also confirm that of others to suggest high PEEP to recruit lungs may not be beneficial in these patients1 but that measures to increase blood flow to the small blood vessels, including sufficient anticoagulation if concerns of pulmonary microthrombi or the use of pulmonary vasodilators, should be considered as part of the overall management strategy for these patients. Further studies with larger sample sizes should be performed to confirm our findings.
Footnotes
Twitter @blackmaccat
Contributors MT and AR devised the study. CP and TM collected data. JDB, MLL and WD performed the functional respiratory imaging analysis. MT, AR and EMS analysed the data and EMS performed the statistical analysis. All authors were involved in writing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JDB, MLL and WD are employees of Fluidda NV who performed the functional respiratory imaging analysis. MT and AR are directors of Qureight who performed the data analytics.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.