Article Text

Abstract
Background Patient sex has clinical and prognostic implications in idiopathic pulmonary fibrosis (IPF). It is not known if sex-related and gender-related discrepancies exist when establishing a diagnosis of IPF. The aim was to determine how patient gender influences the diagnosis of IPF and the physician’s diagnostic confidence.
Methods This study was performed using clinical cases compiled from a single centre, then scored by respiratory physicians for a prior study. Using clinical information, physicians were asked to provide up to five diagnoses, together with their diagnostic confidence. Logistic regression was used to assess the odds of receiving a diagnosis of IPF based on patient gender. Prognostic discrimination between IPF and non-IPF was used to assess diagnostic accuracy with Cox proportional hazards modelling.
Results Sixty cases were scored by 404 physicians. IPF was diagnosed more frequently in men compared with women (37.8% vs 10.6%; p<0.0001), and with greater mean diagnostic confidence (p<0.001). The odds of a male patient receiving an IPF diagnosis was greater than that of female patients, after adjusting for confounders (OR=3.05, 95% CI: 2.81 to 3.31), especially if the scan was not definite for the usual interstitial pneumonia pattern. Mortality was higher in women (HR=2.21, 95% CI: 2.02 to 2.41) than in men with an IPF diagnosis (HR=1.26, 95% CI: 1.20 to 1.33), suggesting that men were more often misclassified as having IPF.
Conclusion Patient gender influences diagnosis of IPF: women may be underdiagnosed and men overdiagnosed with IPF.
- interstitial fibrosis
- idiopathic pulmonary fibrosis
- clinical epidemiology
Statistics from Altmetric.com
Key messages
What is the key question?
How does a patient’s gender influence respiratory physicians when making a diagnosis of idiopathic pulmonary fibrosis?
What is the bottom line?
Respiratory physicians are more likely to give male patients a diagnosis of idiopathic pulmonary fibrosis, after adjusting for age, smoking history, exposures and autoantibodies, suggesting clinicians place a tremendous emphasis on male gender in their pre-test diagnostic probability of this disease.
Why read on?
Although the higher incidence of idiopathic pulmonary fibrosis in male patients has been well established epidemiologically, this is the first study to actually assess how an international sampling of respiratory clinicians integrates patient gender in their diagnostic impression for idiopathic pulmonary fibrosis.
Introduction
Biological sex has important clinical implications in interstitial lung diseases (ILD). Prevalence of different ILD diagnoses varies between sexes: idiopathic pulmonary fibrosis (IPF) and pneumoconioses are common in men, whereas connective tissue diseases (CTD) predominantly affect women.1 2 These differences may in part be due to different genetic and biological predispositions, and in part due to differential exposures. Biological sex has also been shown to have prognostic implications in IPF, CTD-ILD and chronic hypersensitivity pneumonitis, where male sex is a risk factor for increased mortality.3–5
However, it is not known if biases pertaining to biological sex or gender exist when it comes to establishing a diagnosis of ILD on an individual patient basis, assuming equal age, exposures and comorbidities, or if patient gender impacts a physician’s diagnostic confidence for the diagnosis of ILD and IPF specifically. The objectives of this study were to determine how patient gender and other clinical characteristics influence the physicians making a diagnosis of ILD and IPF, as well as the physician’s diagnostic confidence. We hypothesised that female patients would be less likely to receive a diagnosis of IPF and that diagnostic confidence would be lower, but that this difference would disappear after adjusting for age, exposures and other confounders.
Methods
Participating physicians and scoring protocol
This study was performed using clinical cases that were summarised and compiled from a single tertiary care centre, then scored by respiratory physicians for a prior study.6 The study protocol was approved by the National Health Service (NHS) Health Research Authority, and for this retrospective examination of clinically indicated data, the need for patient consent was waived. Briefly, 60 consecutive patients presenting to the ILD unit of the Royal Brompton and Harefield NHS Foundation Trust (London, UK) before the antifibrotic era (between 5 January 2010 and 25 October 2010) were assessed by invited respiratory physicians using a web-based application. Patient’s clinical information included age, gender, lung function, current or prior occupational or environmental exposures (birds, metal dust, wood and asbestos), symptoms of autoimmunity (Raynaud’s, sicca, arthralgias or myalgias), autoantibodies that were available clinically (any titer was considered positive) and serum Aspergillus precipitins. Physicians were asked to review the patients’ clinical information, CT scan images, lung function and bronchoalveolar lavage data and for each case, provide up to five diagnoses, together with their diagnostic confidence for each listed diagnosis (censored at 5% and summing to 100% in each case). The only stipulation to scoring the cases was that each case was evaluated in isolation without interspecialty consultation. For the purpose of this study, all of the cases’ CT scans were read by a thoracic radiologist with 11 years of experience (SLFW) for the usual interstitial pneumonia (UIP) pattern, according to the 2011 and 2018 international guidelines.1 7 The radiologist was not blinded to the patient’s characteristics including sex. Physicians did not have access to this CT report and were not informed if a surgical lung biopsy had been performed.
Before scoring the cases, all physicians had to answer questions about their clinical practice and experience. Physician gender was identified using their names and through an internet search when the name did not immediately inform gender. In addition, a subgroup of expert physicians was identified, comprising respiratory physicians with expertise in the diagnosis and management of ILD, and with a record of publications in this field. The author lists from the published international practice guidelines were used to guide the selection of this group of experts.1 8
Statistical analyses
Statistical analyses were performed using Stata (version 15.1). Summary statistics were used to describe the patient characteristics for the 60 clinical vignettes and the scoring physicians’ characteristics. Differences between male and female patients, and between male and female physicians, were identified using the Student t-test for continuous variables and χ2 test for dichotomous variables. Using the total number of cases scored, the number (%) of the leading diagnoses were compiled for IPF, CTD-ILD and hypersensitivity pneumonitis, stratified by patient gender. Differences in mean diagnostic confidence reported by the physicians were identified using unpaired Student t-test for each diagnostic category. Logistic regression was used to assess the odds of receiving a diagnosis of IPF versus non-IPF ILD based on patient gender. Variables included in the multivariate model were prespecified based on potential confounders in the relationship between gender and ILD diagnoses and included age, smoking history, presence of autoantibodies, serum precipitins and environmental exposures. Analyses were then stratified according to the UIP pattern on CT scan.
Prognostic discrimination between IPF and non-IPF ILD was used as a measure of diagnostic accuracy for a diagnosis of IPF given by scoring physicians, using survival analysis. Cox proportional modelling was used to determine HRs for mortality across diagnoses, adjusted for age and disease severity using lung function, again to validate the accuracy of assigned diagnoses. In principle, more accurate diagnoses of IPF should provide sharper prognostic distinctions between IPF and non-IPF cases. This approach has been used and accepted in prior international studies of diagnostic performance in IPF.6 9 This analysis was adjusted by incorporating clustering at the patient level to account for biases due to survival data originating from only 60 cases. The survival period for each patient was calculated from the date of referral to the host institution to the 1 January 2015 or to the date of death. Mean diagnostic confidence for IPF was compared between male and female patients and across UIP patterns of disease on CT, and regression analyses were conducted to determine the patient-specific and physician-specific variables that influence diagnostic confidence for the leading diagnoses in each case.
Results
Cases and physicians
There were 60 real-life cases compiled from a single institution, of which 34 (57%) were male patients. Their clinical characteristics are described in table 1 according to patient gender. Female patients were significantly younger (p=0.012) and were less likely to have a definite or probable UIP pattern on CT scan. There were no other significant differences between the two groups.
Baseline case characteristics according to patient gender
A total of 404 physicians from 76 countries completed scoring for all 60 cases, for a total of 24 240 physician-case evaluations. Their characteristics are described in detail in online supplementary table 1. Most physicians had received specialised training in ILD (n=359, 89%), and the majority of physicians were male (n=262, 66%). Male physicians were more likely to have been in practice for longer (p=0.001), but less likely to be practicing in an academic institution (p=0.006). There were no significant differences between male and female physician access to multidisciplinary team meetings for reviewing cases in clinical practice.
Supplemental material
Patient gender and IPF diagnosis
A diagnosis of IPF was made significantly more frequently in male patients compared with female patients (p<0.0001, table 2), and with greater mean diagnostic confidence as reported by physicians (p<0.001). This was true whether IPF was listed as a first-choice or second-choice diagnosis. The first-choice diagnosis of IPF was made in 10.6% of female patients, and in 37.8% of male patients. In contrast, female patients more frequently received a first-choice diagnosis of CTD-ILD (p<0.001) or of hypersensitivity pneumonitis (p<0.001).
Leading diagnoses and mean diagnostic confidence based on patient gender for each individual case scored (n=24 240 case scores)
The odds of a male patient receiving a first-choice diagnosis of IPF were three times that of a female patient, after adjusting for age, smoking history, environmental or occupational exposures, and presence of autoantibodies or serum precipitins (OR=3.05, 95% CI: 2.81 to 3.31, table 3). When stratified by UIP pattern on CT scan, the male gender no longer increased the odds of a diagnosis of IPF in those with a definite UIP pattern once adjusted for confounders (table 4). However, men had significantly greater adjusted odds of receiving a leading diagnosis of IPF compared with women when their CT scan showed probable UIP (OR=1.74, 95% CI: 1.52 to 2.01), was of indeterminate pattern (OR=4.83, 95% CI: 3.54 to 6.59) or compatible with an alternate diagnosis (OR=25.58, 95% CI: 17.80 to 36.77). Results were similar whether the 2011 or the 2018 guidelines for UIP pattern were used.
Multivariate models of OR for a leading diagnosis of IPF (vs non-IPF)
OR of a diagnosis of idiopathic pulmonary fibrosis based on CT scan pattern in male patients (compared with female patients)
The odds of having a diagnosis of IPF were also significantly greater with older age, lower diffusion capacity and smoking history (p<0.001). In contrast, a diagnosis of IPF was significantly less likely to be given in the presence of any autoantibody, any environmental exposure or serum precipitins (p<0.001). The unadjusted OR for a leading diagnosis of IPF are outlined in the online supplementary table 2.
Prognostic discrimination for IPF
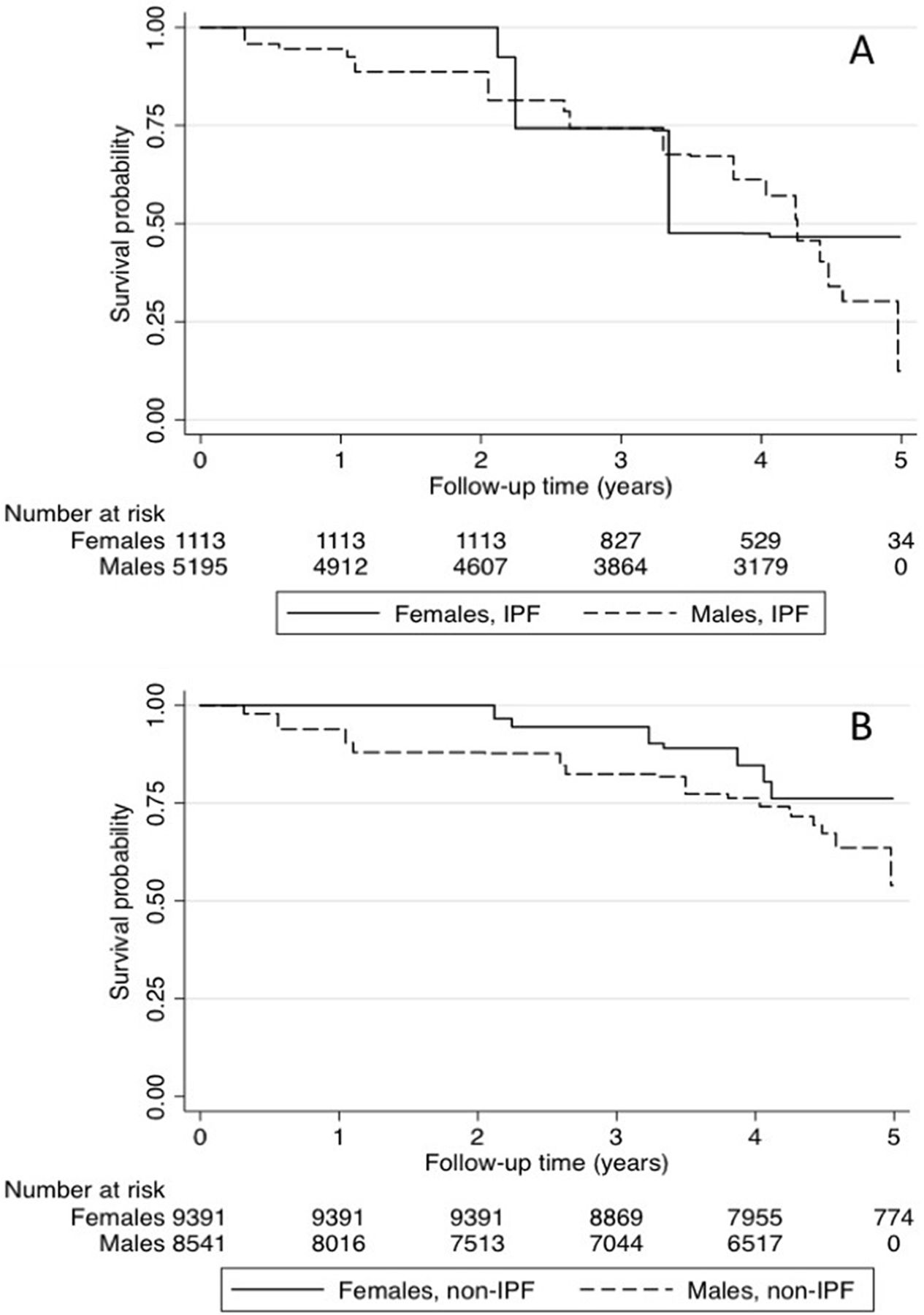
The risk of mortality during the follow-up period was increased overall in cases that were assigned a diagnosis of IPF by physicians compared with non-IPF ILD (table 5, figure 1). The HR for mortality was higher in female patients with a first-choice diagnosis of IPF (HR=2.21, 95% CI: 2.02 to 2.41) than in male patients (HR=1.26, 95% CI: 1.20 to 1.33) after adjusting for age and disease severity (DLCO% predicted). This difference in mortality was especially pronounced when the diagnosis of IPF in females was made by the subgroup of physicians who were considered experts in the field (HR=4.16, 95% CI: 3.10 to 5.90). Adjusting this analysis by incorporating clustering at the patient level did not change the point estimate of the HR for mortality, but did widen the 95% CIs (table 5). Adding smoking history to the model as another confounder did not significantly alter the results, nor did using FVC% predicted or the presence of honeycombing on CT or UIP pattern as measures of disease severity.

{kind=link}
Survival during follow-up with assigned diagnosis of IPF and non-IPF ILD, stratified by gender. Survival during the follow-up period was better in patients who were given a diagnosis of non-IPF ILD compared with those given a diagnosis of IPF. This prognostic discrimination of patients with IPF suggests an accurate diagnosis was made in cases called IPF. Among patients given a diagnosis of IPF (A), female gender conferred a worse prognosis than male patients, suggesting more frequent misdiagnosis in male patients (p<0.001). This opposite was found in non-IPF ILD (p<0.001) (B). ILD, interstitial lungdisease; IPF, idiopathic pulmonaryfibrosis.
Mortality for a diagnosis of IPF adjusted for age and diffusion capacity, stratified by patient gender
Diagnostic confidence
Physicians who gave a diagnosis of IPF did so with significantly greater confidence for patients who were men compared with women (p<0.001, table 2). Diagnostic confidence was greater in those with a definite UIP pattern on CT compared with those with possible or inconsistent with UIP patterns (online supplementary table 3, online supplementary figure). Overall and across all diagnoses, physicians’ diagnostic confidence was significantly impacted by patient gender, smoking history, exposure history, years of experience and practice in an academic centre (table 6). These variables remained statistically significantly associated with diagnostic confidence after multivariate regression analysis. Physician gender did not significantly impact diagnostic confidence across different ILD diagnoses (online supplementary table 4).
Linear regression of diagnostic confidence based on patient-specific and physician-specific characteristics
Discussion
We have shown that male gender leads to a significantly increased odds of being given a diagnosis of IPF by respiratory physicians, despite adjustment for age, smoking history, organic or inorganic exposures, and presence of any positive autoantibody or serum Aspergillus precipitins. Our results suggest that physicians place great emphasis on patient gender in making a clinical diagnosis of IPF, especially in cases where the CT scan is not definitive for a UIP pattern, and that overall, female patients are likely to be underdiagnosed with IPF, whereas male patients are overdiagnosed with IPF. These findings represent an international view of the diagnosis made by >400 respiratory physicians evaluating consecutive cases of suspected ILD.
Although the diagnosis of IPF is widely considered to be more common in males than in females, in our study only about 10% of cases with female patients were given a first-choice diagnosis of IPF, which is substantially lower than expected, and supports the hypothesis that an IPF diagnosis is missed in female patients. In registry and real-life data, males comprise between 67% and 77% of all patients diagnosed with IPF.10–12 In recent treatment trials for IPF, male subjects make up a higher proportion of the study populations, between 78% and 82%.13–15 A recent study based on the Australian IPF registry reported a definite UIP pattern is more common in male patients, whereas there were relatively more females meeting criteria for possible UIP or inconsistent UIP patterns.16 Interestingly, the authors demonstrated similar outcomes between patients with IPF who met guideline criteria for IPF and those who did not, but in whom a working diagnosis of IPF was made. Considering that clinical trials use strict diagnostic criteria for CT UIP, this may contribute to the strong predominance of male subjects in those trials.
Sex and gender are also built into prediction models for the diagnosis of IPF: a recent study looking at predicting histopathological UIP pattern showed that among patients with a possible UIP pattern on CT, the combination of male gender and age over 60 years yielded a specificity of >99% for underlying histopathological UIP.17 However, in this study, sex-based differences were found in CT pattern, with a greater proportion of male patients meeting possible UIP criteria compared with those with CT appearances considered inconsistent with UIP. This difference likely contributed to male gender becoming such a strong predictor of IPF. These findings also suggest that physicians may be missing cases of IPF in female patients when the CT pattern is not definitive for UIP, by being overly influenced by patient gender when making a diagnosis.
In our study, male patients had a nearly 2-fold increased odds of receiving a diagnosis of IPF compared with female patients when the CT scan showed probable UIP, an almost 5-fold increased odds of IPF with a CT that was indeterminate for UIP, and a 25-fold increased when the CT suggested an alternate diagnosis.
We found that outcome distinctions between IPF and non-IPF cases were diminished in male patients compared with female patients despite male gender being associated with increased mortality compared with female gender in a previously reported cohort of patients with IPF.4 Interestingly, diagnostic confidence was higher for a diagnosis of IPF in male compared with female patients despite poorer prognostic discrimination across all CT patterns, meaning that physicians scoring these cases readily labelled a male patient with IPF, frequently and confidently, but not necessarily accurately. Our data do not support alternative explanations for this difference in mortality besides misdiagnosis. First, although it is possible that female patients were diagnosed later in the disease, adjusting the analysis for disease severity (as measured by DLCO% or FVC% predicted) would mitigate this potential lead-time bias. There were also no significant differences in lung function at baseline between male and female cases. Second, a prior study has found that emphysema and smoking history leads to a greater decline in lung function.18 In our study, more male patients were ever-smokers than female patients, which should have made their survival worse than female patients had they been accurately diagnosed as IPF. Also, the addition of smoking to the Cox proportional analysis did not significantly change the hazards of mortality.
Gender-based biases in the diagnosis of IPF may have a detrimental impact on treatment initiation. In studies of antifibrotic therapy, male patients comprise the majority of participants.19–22 Including a lower proportion of female patients in drug studies may lead to underappreciating the effects and risks of these medications in women. Female patients have also been shown to discontinue treatment more frequently,23 which could suggest that physicians feel less compelled to keep patients on medication when the diagnosis is less certain. This gender-based treatment gap extends to non-pharmacological therapies such as exercise rehabilitation, where male patients make up a greater proportion of the study population in pulmonary rehabilitation studies.24 25 A similar disparity was found among lung transplant recipients, with male patients receiving more transplants than female patients with IPF, despite male gender being associated with a higher risk of death.26 27
Our study has some unavoidable limitations, common to previous studies of multidisciplinary practice.6 9 Unlike real-world clinical practice, physicians did not engage in face-to-face patient consultation. In complex diseases, direct patient contact may impact clinical impressions in ways that are not easy to replicate. However, our methodology of web-based case reviews enabled access to a large diverse group of physicians which would otherwise have not been possible. This approach is similar to previously published studies of diagnostic performance.6 9 Second, physicians evaluated cases without the benefit of multidisciplinary characterisation which is considered the gold standard for diagnosis, and which could have conceivably impacted diagnosis and management decisions. However not all physicians have access to multidisciplinary meetings and when available, not every case of suspected IPF is discussed. Finally, having only 60 cases scored may have influenced the results, which will have to be validated in further studies. Having a greater number of cases of diverse gender and ethnicities would perhaps add important variability and power to this study, but this limitation is countered by the very high number of international physicians who were able to complete the scoring on all cases.
In conclusion, our results provide evidence that gender impacts clinical impression in patients with suspected IPF, especially when the CT scan is not definite for UIP, which may lead to misdiagnosis and subsequent suboptimal management in female and male patients. Overall, the ILD research and clinical community need to carefully ensure that female patients with IPF are diagnosed and managed appropriately. Moreover, IPF treatment trials should ensure that enrolled cohorts accurately reflect the proportions of male and female patients with IPF in unselected populations.
Acknowledgments
The authors would like to acknowledge the 404 respiratory physicians world-wide who scored the 60 cases and provided their diagnostic impression which were used for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All listed authors have substantially contributed to the conception and design of this study. All authors have contributed to the writing of the manuscript and critical revisions for intellectual content, and have read and approved the final version submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DA reports personal fees and other from Hoffman-La Roche Ltd, personal fees and other from Boehringer Ingelheim, outside the submitted work. JM reports personal fees from Roche, personal fees from Boehringer Ingelheim, outside the submitted work. JK reports personal fees and other from Hoffman-La Roche Ltd, personal fees and other from Boehringer Ingelheim, personal fees from Theravance, grants from CHEST Foundation, grants from UCB Biopharma SPR, grants from University of Calgary, outside the submitted work; AW reports personal fees from Boehringer Ingelheim, personal fees from Intermune/Roche, personal fees from Bayer, outside the submitted work; SW reports personal fees from Boehringer Ingelheim, personal fees from Intermune/Roche, personal fees from Sanofi-Genzyme, personal fees from Bracco, personal fees from Oncoarendi therapeutics, outside the submitted work;
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.