Article Text

Abstract
Background Approximately 15%–20% of all non-small cell lung cancer (NSCLC) cases present with stage I disease. Surgical resection traditionally offers the best chance of a cure but some patients will not have this treatment due to older age, comorbidities or personal choice. Stereotactic ablative radiotherapy (SABR) has become an established curative intent treatment option for patients who are not selected for or do not choose surgery. The aim of this study is to compare survival at 90 days, 6 months, 1 year and 2 years for patients who received either lobectomy or SABR.
Methods We used data from the 2015 National Lung Cancer Audit database and linked with Hospital Episode Statistics and the radiotherapy dataset to identify patients with NSCLC stage IA-IB and performance status (PS) 0–2 who underwent surgery or SABR treatment. We assessed the likelihood of death at 90 days, 6 months, 1 year and 2 year after diagnosis and procedure date to observe survival between two patient groups.
Results We identified 2373 patients in our cohort, 476 of whom had SABR. The median difference between date of diagnosis and date of treatment for surgery patients was 17 days while for SABR patients it was 73 days. Increasing age and worsening PS were associated with having SABR rather than surgery. Survival between the two treatment modalities was similar early on but by 1-year people who had surgery did better than those who had SABR (adjusted ORs 2.12, 95% CI 1.35 to 2.31). This difference persisted at 2 years and when the analysis was restricted to patients aged <80 years and with PS 0 or 1 and stage IA only.
Conclusion Our analysis suggests that patients who have lobectomy have a better survival compared with SABR patients; however, we found considerable delays in patients receiving SABR which may contribute to poorer long-term outcomes with this treatment option. Reducing these delays should be a key focus in development and reorganisation of services.
- lung cancer
- thoracic surgery
- non-small cell lung cancer
Statistics from Altmetric.com
Key messages
What is the key question?
Is there a survival difference between patients with stage I non-small cell lung cancer (NSCLC) undergoing lobectomy compared with stereotactic ablative radiotherapy (SABR)?
What is the bottom line?
There is an early survival benefit for patients undergoing SABR, however from 6 months onwards, lobectomy has better overall survival. The patient pathway for receiving SABR is longer than for surgery.
Why read on?
Lobectomy is the treatment of choice for stage I NSCLC with SABR offered to people who decline lobectomy or in whom lobectomy is contraindicated. Trusts and cancer alliances in England should look to optimise their patient pathways for SABR.
Introduction
Non-small cell lung cancer (NSCLC) accounts for almost 85% of all pathologically confirmed lung cancer cases diagnosed in England. Compared with other European and North American countries, people in England have poor overall survival for lung cancer.1 2 This may partly be due to lower rates of delivery of potentially curative treatment, especially surgical resection in stage I lung cancer.3 Recent reports from the National Lung Cancer Audit (NLCA) 2016 have demonstrated that survival figures are improving year on year for England, and that resection rates are also increasing.4 However, even for patients with early stage and good performance status (PS), only 60% ultimately undergo surgical resection.5 Approximately 15%–20% of people with NSCLC have stage I disease at presentation; increasing this proportion is the goal of national early diagnosis programmes and lung cancer screening proposals.
Although surgery is the standard of care in early lung cancer, stereotactic ablative radiotherapy (SABR), a non-invasive external beam radiotherapy has become an established treatment option for early stage patients with peripheral tumours under 5 cm, not suitable for, or declining surgery. SABR uses hypo-fractionated dose schedules and high precision treatment delivery to improve local control of disease compared with fractionated radical radiotherapy.6 7 Studies have also shown less toxicity related to SABR, even in elderly patients, with no significant decline in quality of life.8 9
The recent Lung Cancer Clinical Outcome Project publication reports an overall 90 days survival of 96.3% after surgery for stage I and II, failing to 87.9% after 1 year.4 However, the survival of patients who undergo SABR has not been reported in the same population. The aim of this study was therefore to evaluate survival at different points after treatment for patients who receive SABR treatment compared with lobectomy in stage I patients in England using the 2015 NLCA database.
Methods
Databases
National Lung Cancer Audit
The recently validated new NLCA database is a longitudinal database that contains data on core cancer and lung specific data items. The audit uses anonymised data collected and processed by the National Cancer Registration and Analysis Services (NCRAS) on all new lung cancer cases submitted by 142 National Health Service (NHS) trusts in England. The NLCA was linked with Hospital Episode Statistics (HES) inpatient data to provide data on any curative/palliative treatment received in secondary care, including lung cancer surgery and Office of National Statistics for accurate records of date of death.
National radiotherapy dataset
The radiotherapy dataset (RTDS) collects consistent and comparable data in order to provide intelligence for service planning, commissioning, clinical practice and research. The RTDS started collecting data from April 2009 and all NHS trusts providing radiotherapy services are required to return data to Public Health England for all activities undertaken on brachytherapy and teletherapy machines. Aside from the type and intent of radiotherapy given, the RTDS also contains details on date of exposure, dose and fraction of each exposure event and trust name of where each therapy took place. The RTDS was linked with the NLCA and anonymised prior to analysis.
The RTDS does not specify what radiotherapy type was administered other than the dose and fraction prescribed, and therefore to identify SABR doses, the data for the all the prescribed dose and prescribed fraction was reviewed by two oncologists independently and then statistically assessed for agreement. A dose of ≥50 Gray (Gy) delivered in 3–8 fractions was considered as a SABR dose in our study. We also carried out Cohen’s Kappa κ statistics and percentage agreement to assess the level of agreement between the two oncologists identifying SABR doses in the RTDS database.
Study population and covariates
We conducted a cohort analysis and used data on all English patients diagnosed with primary lung cancer defined by the International Classification of Disease V.10 (ICD-10) code of C34* in 2015, who had a proven or presumed NSCLC. Patients who were diagnosed through their death certificate were excluded from further analyses. We further restricted our analysis to people with stage IA and IB (tumour, node, metastases (TNM) V.7 defined by the Union for International Cancer Control) and with good PS, that is, PS 0, 1 and 2 as these people are more likely to undergo curative treatment. We identified cases of pathologically confirmed NSCLC based on the recorded Systematised Nomenclature of Medicine (SNOMED) codes, whereas cases without a pathologically confirmed diagnoses, ‘unknown lung cancer’ SNOMED codes or clinically confirmed cases were also classified as NSCLC. This encompasses around 23%–25% of all lung cancer cases annually, and are referred to as ‘presumed’ NSCLC cases as majority of the pathologically confirmed cases are NSCLC. This is in line with the standard NLCA definition of NSCLC.4 Therefore in our cohort, 75% of the people had a confirmed pathological diagnosis of NSCLC, while the rest were presumed to be NSCLC. Using the HES dataset, we were able to obtain data on our cohort’s hospital admissions going back to 2004 which helped us create a comorbidity score. If the person did not have a hospital admission with an ICD-10 code indicating a comorbidity according to the Charlson Index,10 they were coded as having no comorbidity.
In addition to treatment data, we extracted data on variables including age, sex, PS and stage. Age was calculated at diagnosis and grouped into three categories (<65 years, 65–80 years and >80 years). PS, a marker to assess patient’s fitness, was classified according to the WHO definition and stage of the disease was defined using the Union for International Cancer Control definition (TNM V.7), both are recorded in the NLCA. We identified the type of surgery a patient had from NLCA and HES using Office of Population Census and Survey Classification of Intervention V.4 codes. If there was more than one lung surgery recorded, the most extensive one was considered. We only included patients who had either lobectomy or bilobectomy (E54.2, E54.3). All treatments recorded 6 months after diagnosis were excluded on the basis that they may not be related to lung cancer.
Statistical analysis
All data and statistical analysis were performed using STATA V.15. First we conducted a logistic regression analysis to assess association between patient features and likelihood of receiving SABR rather than surgical resection. For our main analyses the endpoints were the likelihood of death at 90 days, 6 months, 1 year, 2 years and overall survival, defined as the time interval between (1) first date of treatment (either SABR or surgery) and date of death from any cause and (2) time difference between date of diagnosis and date of death—to account for the lag time between treatment decision and start of SABR for cases where surgery was initially considered but not received. We used logistic regression analysis to compare survival odds at each specified time points and Cox regression to assess overall survival difference. Log minus log and Schoenfeld tests were performed to check for proportional hazard assumptions and Kaplan-Meier curves estimating survival difference between two groups from time of procedure and time of diagnosis. As a sensitivity analysis to limit the analysis to very fit patients, we also conducted similar analysis on stage IA patients only, excluding patients over the age of 80 years and those with poor PS (PS=2)—patient characteristics that are clinically strongly associated with receiving SABR over lobectomy. We present adjusted ORs that were adjusted for sex, age, PS, stage, comorbidity score, socioeconomic status, lung cancer laterality and pathological confirmation of the diagnosis. All logistic regression analyses were also assessed with 99% CI limits to remove bias by multiple comparisons. Kaplan-Meier (KM) curves for survival by treatment groups and restricted to age <80, stage IA and PS 0–1 were plotted.
Results
We identified 2373 English patients diagnosed between 1 January 2015 and 31 December 2015 from the linked NLCA dataset that met our inclusion criteria (NSCLC, PS 0–2 and stage IA/IB). The median follow-up length was 2.14 years (IQR 1.85–2.43 years). Baseline patient characteristics are presented in table 1. Fifty-three per cent of our cohort were females (53%) and more than three-fifths of the cohort were aged between 65 and 80 years (62%). 40% had PS 0, 45% had PS 1 and the majority (60%) of the cohort had stage IA NSCLC. Patients treated with lobectomy had better comorbidity score (Charlson Index 0 or 1) than those undergoing SABR. Using the Cohen’s Kappa statistics and percentage agreement, the results from the two oncologists agreed on 99% of the patient radiotherapy doses in the RTDS with a kappa coefficient of 0.993 and we identified 476 patients who received SABR while 1897 had surgery.
Descriptive statistics comparing patient features (n=2373)
We used logistic regression analysis to identify patient features most strongly associated with treatment and these are presented in table 2. There was no association seen with type of treatment received and sex and laterality; however, increasing age was associated with a higher likelihood of having undergone SABR compared with patients aged less than 65 years (age 80 and above OR 12.4, 95% CI 7.45 to 20.9). Patients with stage IB were 52% less likely to have SABR compared with patients with stage IA lung cancer (OR 0.48, 95% CI 0.35 to 0.66). A strong association was also seen with increasing PS and likelihood of having SABR (PS 2 OR 14.5, 95% CI 9.40 to 22.6). This association was still present when patients with missing PS were excluded from the analysis. While in our univariate analysis we saw an association between patients undergoing SABR with a comorbidity index of 4 or more, this was not observed when adjusted for other patient features in table 2.
Likelihood of receiving SABR compared with surgery based on patient features (n=2373)
Pathway from diagnosis to treatment
The median difference between date of diagnosis and date of treatment for surgery patients was 17 days (IQR 1–44) and 73 days (IQR 56–103) for patients who underwent SABR. The median time difference from diagnosis to treatment in biopsied SABR patients was 70 days, 10 days less than SABR patients who were not biopsy confirmed. We also considered the time difference between start of treatment and the final pretreatment multi-disciplinary teams (MDT) discussion date which still showed a difference of almost a month between SABR and surgery (time difference between MDT and surgery =34 days, MDT and SABR =61 days).
Overall survival
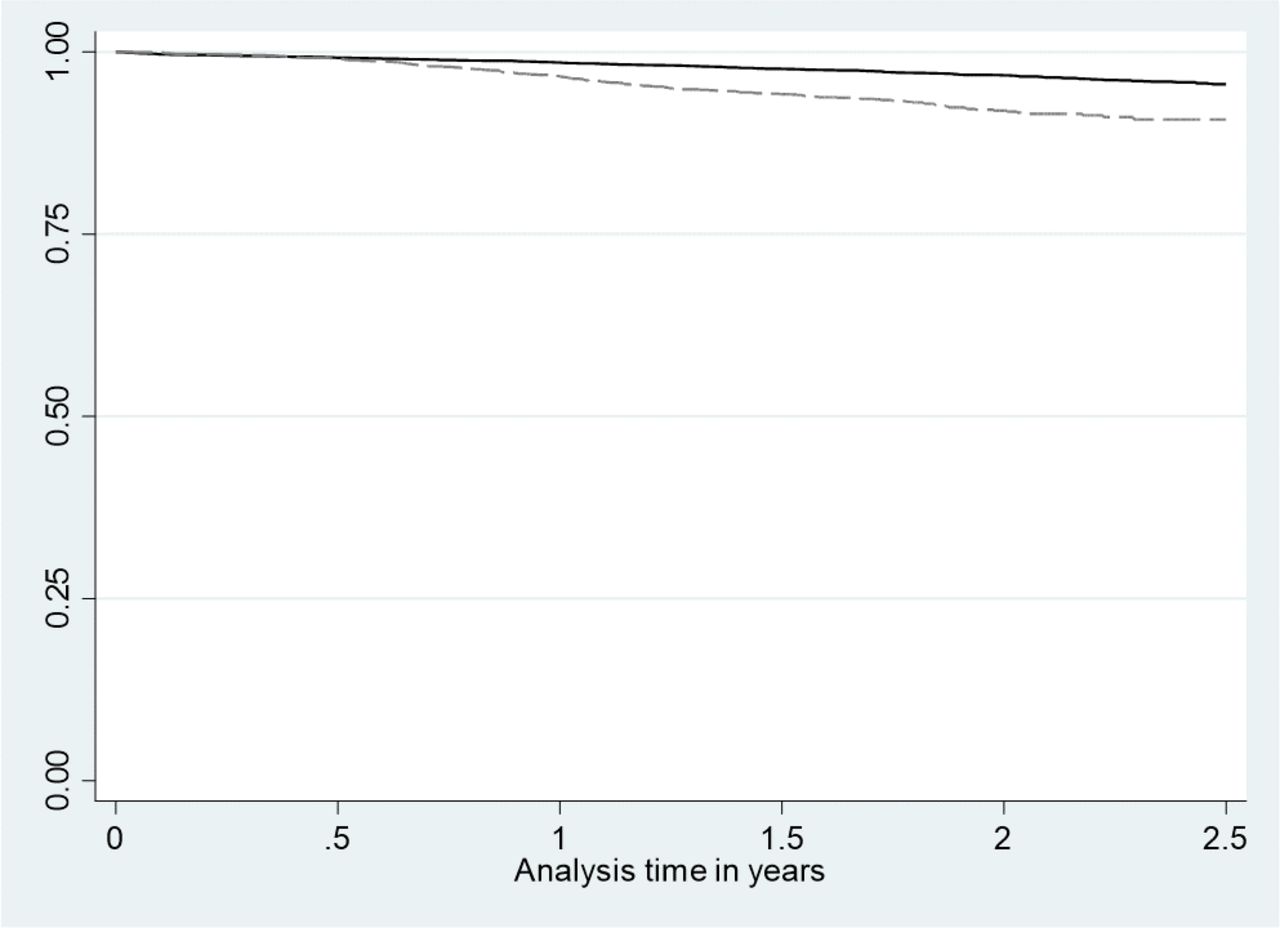
In the first 6 months postprocedure, there were 35 deaths from any cause in the lobectomy group and 21 deaths in SABR group. This doubled in the next 6 months with an additional 52 deaths from any cause in the lobectomy group and 48 deaths in the SABR group. For our Cox regression analyses the proportional hazard assumptions were not met, and for this reason we are not reporting an overall HR but have included the unadjusted and adjusted Kaplan-Meier survival curves (figures 1 and 2). Our Kaplan-Meier plots show good overall survival for people undergoing both SABR and lobectomy. The curves are similar for lobectomy and SABR for the first 6 months, but thereafter lobectomy seems to have a better survival.

Unadjusted Kaplan-Meier estimates from the date of procedure and number of patients at risk of death at 6 months interval.
{kind=link}
{kind=link}
Adjusted Kaplan-Meier estimates from the date of procedure (adjusted for sex, age, performance status, stage, Charlson Index, socioeconomic status, pathology confirmation and lung cancer laterality.
Likelihood of death from date of treatment
The results of logistic regression analysis conducted from the date of either lobectomy or SABR procedure are presented in table 3. Male gender, increasing age, worse PS, advance stage, comorbidity and cancer laterality were not associated with survival.
Regression analysis from date of procedure till death at 90 days, 6 months, 1 year and overall
We found no evidence of a difference in survival between the treatment modalities in the first 180 days after treatment. However, by 1 year, the likelihood of death from any cause for SABR patients was higher than those having surgery (adjusted OR 2.12, 95% CI 1.35 to 3.31). This difference persisted at 2 years where the ORs for death from any cause for SABR compared with lobectomy was 2.20 (95% CI 1.56 to 3.09–99% CI 1.40 to 3.45) (see online supplementary appendix 1 for tables with 99% CI). In addition we found that in our sensitivity analyses on stage IA patients only, excluding patients over the age of 80 years with poor PS (PS≥2) (online supplementary table S1), the survival benefit of surgery vs SABR persisted at 1 year and 2 years.
Supplemental material
Likelihood of death from date of diagnosis
We conducted a separate logistic regression analysis from the date of diagnosis of lung cancer until death, presented in table 4. The difference in the likelihood of death was not observed until after 1 year from diagnosis (2 years ORs 1.89, 95% CI 1.33 to 2.69, 99% CI 1.19 to 3.01). Male gender, older age, worsening PS, advance stage lung cancer and being from the most deprived socioeconomical group were associated with a higher likelihood of death at 95% CI but only PS 2 and stage IB were significant at 99% CI at 1 year (see online supplementary appendix table). PS 2, stage IA and IB, most deprived socioeconomic status and male gender were significant at 99% CI at 2 years. When the results were restricted to patients aged <80 year and with PS 0 or 1 and stage IA, SABR patients had an overall poor survival which was only significant at 5% (p value 0.035) (online supplementary table S2). None of the patient features were significantly associated with increased likelihood of death at 1 year at 99% CI (most deprived socioeconomical status significant at 95% CI).
Regression analysis from date of diagnosis till death at 90 days, 6 months, 1 year and overall
Discussion
Main findings
The present study is the first to use English registry data to look at outcomes for stage I NSCLC patients treated with either lobectomy or SABR. Real world data is especially important because randomised trials comparing lobectomy to SABR closed due to poor recruitment.11 Similar to other registry studies, this analysis shows long-term overall survival benefit for patients treated with lobectomy, an association also present when the analysis was restricted by exclusion of older patients with PS 2 and stage IB. Lobectomy remains the treatment of choice for stage I NSCLC in the new National Institute for Health and Care Excellence (NICE) guidelines.12
Patient features including age, PS, comorbidity and stage were very strongly associated with the type of treatment received and contribute to the better survival for patients undergoing lobectomy compared with SABR similar to results from published meta-analysis.13 Our result shows, that the patients undergoing SABR were significantly more likely to be older, have poor PS and have more comorbidities. This study also supports NICE recommendations that SABR should be offered as the curative intent treatment of choice to stage I NSCLC patients who are medically inoperable due to comorbidities or who decline surgery. Another association that remained in our sensitivity analysis was the overall increased likelihood of death in the most deprived socioeconomic group compared with others even after taking into account multiple patient and tumour features. We believe the increased comorbidity associated with a higher smoking prevalence in this groups14 could account for the poor outcome in this group. There is a possibility that we may have underestimated comorbidity. However, studies comparing comorbidity records in primary care data with secondary care data in England have shown that although HES missed a few comorbid conditions, life changing comorbidity, which is more likely to require hospital admission, was better recorded in HES.15 Therefore, with better recording of life threatening and life limiting conditions in HES, it would not have influenced our results much.
Results from studies comparing lobectomy with SABR have failed to reach consensus with some studies favouring early survival and comparable short and overall survival for patients undergoing SABR compared with surgical resection9 16–18 while others have shown higher overall survival for surgery.19 However, a meta-analysis of 12 studies by Deng et al 20 showed that SABR was associated with a significantly lower 3-year overall survival (relative risk of death (surgery/SABR)=0.78). One of the reasons for the lack of consensus may be that different proportions of different operations form the comparison with SABR; these may be lobectomy, sub lobar resections or even pneumonectomy. Another major factor is undoubtedly the difficulty with adequately controlling for frailty in the SABR group. Despite our best attempts to control for this in our study, there may still be some residual confounding due to frailty. Our study shows similar results to study by Puri et al 19 using the American National Cancer Database in which they conclude that patients with surgery have longer overall survival than those who undergo SABR.
An unexpected finding in this study was a large time difference from diagnosis to treatment between patients who have surgery and SABR and there may be a number of reasons for this, reflecting everyday practice in England. One of the factors may be lag time for offering SABR to patients initially thought to be medically operable but subsequently found to be borderline or too high risk on further assessment. Second, the NLCA definition of ‘date of diagnosis’ prioritises date of pathology but for patients who do not have pathology (48% of SABR patients), the date of diagnosis would be the first date of CT or CT-PET imaging, which typically occurs earlier in the pathway. Medically inoperable, frailer SABR patients may have had several CTs demonstrating growth of an unbiopsied pulmonary nodule before proceeding to PET-CT scan and then delivering SABR.21 This timeline should improve as English hospitals work towards implementing the National Optimal Lung Cancer Pathway and while SABR may still be deliverable, the new TNM8 staging reflects that even small increases in the size of stage I lung cancers influences long-term outcome.22 23 Conversely, the low pathological confirmation rates in SABR patients (52%) compared with surgical patients (99%) may positively influence survival for patients, as some may not have lung cancer, although other studies have not shown this to be the case.24 Finally, variation in health service resources may also be a factor as SABR was only available in 17 English radiotherapy centres in 2015 and not all lung MDTs had access to a SABR oncologist, requiring tertiary referral for consideration of this treatment. Increasing access to lung SABR across the country by commissioning lung SABR delivery in more radiotherapy centres may help address this and in addition, may allow more older, frailer stage I patients who currently receive no treatment at all, easier access to SABR.
Limitations to our study include the lack of adjustment for lung function, tumour location, size and comorbidities which have not led to a hospital admission but may have influenced treatment selection. The NCRAS and NLCA databases either do not collect data on these items or have poor data completeness. We were also unable to identify and include sublobar resections in the surgical group or differentiate the surgery category of ‘lobectomy’ into types including open lobectomy, video assisted thoracoscopic surgery (VATS) or robotic, which may have underestimated mortality if reports of mortality rate of surgery being better with VATS are confirmed.25
Another important limitation is the lack of nationally collected data on disease specific survival and recurrence. Although our data shows that patients undergoing SABR are more likely to die in the months after treatment, we cannot know what proportion of deaths in each group occur from lung cancer or from unrelated conditions, although the fact there was no increased risk of death at early time points would suggest the risk of treatment-related death is low in both groups. In view of the fact that SABR patients are generally older and of poorer PS, their risk of non-cancer related death is likely to be substantial as reported in a contemporary SABR cohort within the CHISEL trial where there were more deaths from non-cancer related causes than from lung cancer itself in the months following treatment.7
Clinical relevance
This study has identified an overall survival difference in stage I NSCLC patients undergoing lobectomy versus SABR in routinely collected real world data and supports the recent NICE guidance of recommending lobectomy as treatment of choice with SABR or sublobar resection offered for people who decline lobectomy or in whom it is contraindicated. It also identified delays in the patient pathway for SABR compared with lobectomy which should be addressed nationally.
References
Footnotes
Contributors The conception of the study was done by AK and RH. AK acquired the data from the National Cancer Registration and Analysis Services (NCRAS) and all analysis was done by AK. RH, SH, NN, DW, DB and PB were involved in the data interpretation. Majority of the paper (including the initial draft) was written by AK and RH, SH, DB, NN, DW and PB were involved in revising the paper critically. The final manuscript was approved by all the authors prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AK has conducted the statistical analysis for the National Lung Cancer Audit annual reports for the past 4 years, which were funded by Royal College of Physicians. None of the authors have received any personal earnings from any funding body for this work. RH has a grant provided by the British Lung Foundation chair of respiratory epidemiology.
Patient consent for publication Not required.
Ethics approval The data were obtained from NCRAS. The responsibility for reporting to CAG/HRA on the processing of cancer registration data without patient consent under the PIAG 03(a)/2001 approval transferred to Public Health England, which became known as NCRAS. The NLCA has Ethics and Confidentiality Committee (ECC) approval to use patient information from the National Health Services (NHS). The data were anonymised in the linked dataset by NCRAS personal prior to be given to the researcher.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data used in this study is available on formal request from National Cancer Registration and Analysis Service (NCRAS). Data requests can be made to the "PHE Office for Data release" https://www.gov.uk/government/publications/accessing-public-health-england-data