Article Text

Abstract
Background There is high interest in strategies for improving early detection of chronic obstructive pulmonary disease (COPD). These strategies often rely on opportunistic encounters between patients with undiagnosed COPD and the healthcare system; however, the frequency of these encounters is currently unknown.
Methods We used administrative health data for the province of British Columbia, Canada, from 1996 to 2015. We identified patients with COPD using a validated case definition, and assessed their visits to pharmacists, primary care and specialist physicians in the 5 years prior to the initial diagnosis of COPD. We used generalised linear models to compare the rate of outpatient visits between COPD and non-COPD comparator subjects matched on age, sex and socioeconomic status.
Results We assessed 112 635 COPD and non-COPD pairs (mean 68.6 years, 51.0% male). Patients with COPD interacted with pharmacists most frequently in the 5 years before diagnosis (mean 14.09, IQR 4–17 visits/year), followed by primary care (10.29, IQR 4–13 visits/year) and specialist (8.11, IQR 2–11 visits/year) physicians. In the 2 years prior to diagnosis, 72.1% of patients with COPD had a respiratory-related primary care visit that did not result in a COPD diagnosis. Compared with non-COPD subjects, patients with COPD had higher rates of primary care (rate ratio (RR) 1.40, 95% CI 1.39 to 1.41), specialist (RR 1.35, 95% CI 1.34 to 1.37) and pharmacist (RR 1.62, 95% CI 1.60 to 1.63) encounters.
Conclusions Patients with COPD used higher rates of outpatient services before diagnosis than non-COPD subjects. Case detection technologies implemented in pharmacy or primary care settings have opportunities to diagnose COPD earlier.
- COPD epidemiology
- health economist
Statistics from Altmetric.com
Key messages
What is the key question?
Which types of healthcare encounters should be targeted for case detection to improve early diagnosis of patients with chronic obstructive pulmonary disease (COPD)?
What is the bottom line?
Case detection technologies implemented in pharmacy or primary care settings have many opportunities to diagnose COPD earlier; encounters related to circulatory or respiratory disease offer particularly high value opportunities.
Why read on?
This is the first study to present a comprehensive characterisation of healthcare encounters in outpatient settings before COPD diagnosis, and in comparison to a control cohort.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive disease of the airways that affects approximately 384 million people globally,1 and resulted in the deaths of 3.2 million people in 2015 alone.2 Despite the high prevalence of COPD, an estimated 81% of patients with COPD worldwide have not received a diagnosis at any given time.3 These patients are not receiving treatment and risk factor mitigation for the disease, and are likely to experience worse outcomes over the long term.4 In high-income countries, patients with undiagnosed COPD tend to have less severe disease than diagnosed patients.5 However, previous studies indicate that healthcare services use among these patients is substantial.6 7
Numerous case detection and screening strategies have been proposed to diagnose patients with COPD earlier.8 These strategies typically rely on opportunistic encounters between patients with undiagnosed COPD and the healthcare system.8 The patterns of healthcare services use among patients with undiagnosed COPD are therefore critical factors in determining their success. In a population-based study of nearly 40 000 patients with COPD, a sharp increase in respiratory-related physician consultations in the 5 years preceding a diagnosis of COPD was documented.9 The authors concluded that there was a missed opportunity for an earlier diagnosis of COPD in 85% of patients, and suggested implementing a case-finding approach based on patient risk factors.9 However, this study only examined respiratory-related resource use, and most interactions between patients with undiagnosed COPD and the healthcare system likely occur for non-respiratory reasons.7 This study also did not compare healthcare utilisation in a comparator group. In order to enable efficient case detection strategies, it is necessary to identify the encounters that are best at distinguishing COPD from non-COPD patients.
To address this knowledge gap, we documented the type and frequency of outpatient visits in a population-based sample of patients with COPD before diagnosis. We assessed the rate and probability of primary care, specialist and pharmacist visits in the 5 years preceding a diagnosis of COPD. We compared these results to a matched population of non-COPD subjects to identify the types of visits that were most predictive of a patient having COPD.
Methods
Study design
We conducted a population-based, retrospective cohort study using health administrative data. All inferences, opinions and conclusions drawn in this research are those of the authors and do not reflect the opinions or policies of the data steward(s).
Data sources
The province of British Columbia (BC), Canada, had a population of 4.8 million in 2017.10 To administer the public healthcare system in BC, healthcare utilisation records of all legal residents are collected in centralised databases. These administrative databases comprehensively capture information on (1) hospitalisations,11 which include admission date, discharge date and diagnoses coded using the International Classification of Diseases, 9th or 10th revisions (ICD-9, ICD-10) revisions, (2) physician billing claims,12 which include service date, diagnoses and practitioner type, and (3) medication dispensation records,13 which include service date and drug type. In BC, general practitioners and specialists can practise within the community or be employed by hospitals. There are no private healthcare institutions that provide similar services. Demographic and census information are also recorded,14 15 including date of birth, sex and socioeconomic status (SES) based on income quintiles in the geographical neighbourhood of residence.
Study population
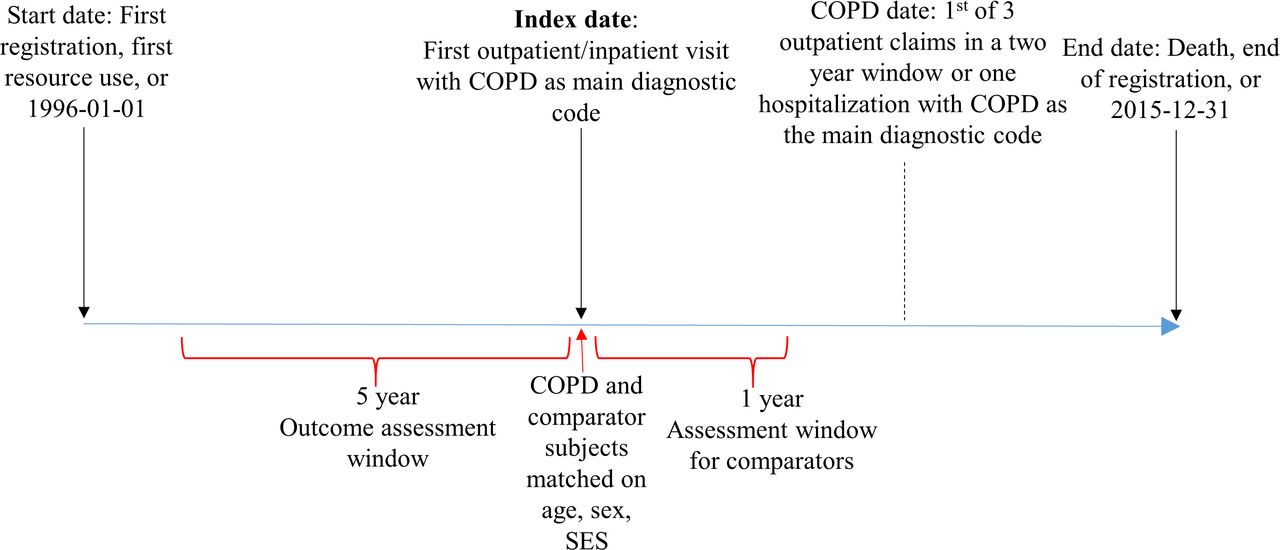
Figure 1 depicts the study design. We created a retrospective longitudinal cohort of patients who fulfilled a validated case definition for COPD between 1 January 1996 and 31 December 2015. Our case definition has a specificity of 95%.16 We defined the index date as the date of first healthcare resource use of any type (outpatient or inpatient) with COPD as the main diagnostic code. Patients who fulfilled the case definition but were <40 years on the index date were excluded, as there is a higher likelihood of overdiagnosis in these patients.

Study design. COPD, chronic obstructive pulmonary disease; SES, socioeconomic status.
The comparator non-COPD cohort was composed of subjects who, as of the same day of follow-up for each patient with COPD, were not diagnosed with COPD. Controls either never developed COPD during the follow-up, or were diagnosed with COPD later in the study period. A comparator subject was matched to each patient with COPD using the following criteria: (1) year of birth within 5 years, (2) sex, (3) sociodemographic status within one income quintile and (4) no COPD diagnosis date, or a diagnosis date that occurred later than their matched patient with COPD. Comparator subjects were assigned the same index date as their matched patient with COPD. Patients with COPD and comparator subjects were required to be in the dataset for at least 5 years prior, and 1 year following the index date. To ensure that comparator subjects were in the province around the index date, COPD/comparator pairs in which the comparator had no healthcare resource use of any type in the year following the index date were excluded. Patients with COPD had an instance of resource use at the index date by definition, thus satisfying this criterion. We assessed healthcare encounters in the 5 years prior to the index date for COPD and comparator subjects. We excluded all pairs in which the patient with COPD had a diagnostic code for spirometry within 1–5 years of index, but the test did not result in a diagnosis of COPD.
Healthcare system encounters
For each subject, we determined the number of outpatient visits in each of the five 1 year periods prior to the index date. We assessed visits to (1) pharmacists, (2) primary care physicians, (3) specialist physicians and (4) primary care physicians for respiratory-related reasons. Physician visits types were distinguishable using specialty codes, and all specialties, regardless of their field, were included in the specialist physician assessment. Respiratory-related visits were those with a primary diagnostic code for respiratory diseases other than COPD (ICD-9 460–466, 470–478, 480–487, 490–496, 500–508, 510–514, 516–519, ICD-10 J00-J99) or for respiratory symptoms (ICD-9 786, ICD-10 R05-R07). We did not assess hospitalisations as the focus of this study was on community-based case detection.
We categorised the types of COPD-related inhaler medications dispensed at pharmacist visits using Health Canada’s unique Drug Identification Numbers. We defined the following medication groups: inhaled corticosteroids (ICS), long-acting beta-agonists (LABA), long-acting muscarinic agents (LAMA), short-acting beta-agonists (SABA) and short-acting muscarinic agents (SAMA). Combination therapies were single inhaler ICS/LABA, SABA/SAMA and LAMA/LABA, or LAMA and LABA dispensed as separate inhalers on the same date. We used a master drug list (online supplementary e-table 1) to identify all other respiratory medications. Over-the-counter medications were not recorded in our dataset.
Supplemental material
Analysis
All analyses were conducted in SAS V.9.4 (SAS Institute). We initially created a descriptive summary of the rate of outpatient visits per patient-year, stratified by COPD status. Second, we assessed the medical indications that prompted patients with COPD to visit a primary care physician before diagnosis. Medical indications were grouped by disease type based on the main diagnostic code for each visit. Within disease types, main diagnostic codes could be for either symptoms or disease diagnoses. In a small minority of cases, a visit was attributed to more than one medical indication, and these were counted as separate visits. Third, we calculated the mean number of pharmacist visits per patient year in which a respiratory medication was dispensed. When more than one medication of different classes were dispensed at the same visit, these were counted separately. Last, we assessed the probability that patients with COPD had any opportunity for case detection in the 5 years before diagnosis. We determined the proportion of COPD and comparator subjects with at least one visit of each type in the cumulative years before diagnosis (ie, year 1, then years 1 and 2, etc).
We tested for differences in the rate of outpatient visits between patients with COPD and comparator subjects. We constructed separate generalised linear regression models (negative binomial distribution, log link) for each of the four visit types. The rate ratio (RR) gives the ratio of visit rates between patients with COPD and comparators. We used generalised estimating equations to account for clustering of data between matched pairs of observations. Period number (1–5 range), calendar year at the beginning of the period, age, sex and SES on the index date were included in all models to adjust the exposure estimates for the overall effects of these variables over the study period. To assess trends in the rate of healthcare visits as patients with COPD approached diagnosis, we constructed a second model for each of the dependent variables. The independent variables were identical to the original model, with the addition of an interaction term between period and the group-defining variable (COPD/comparator).
We conducted a sensitivity analysis on the subset of patients with COPD who were prescribed LAMA in the year before or after their index date. Physicians prescribing this drug must provide evidence that the ratio of forced expiratory volume in 1 s (FEV1) to forced vital capacity is <0.7 and FEV1 ≤65% of predicted,17 meaning that nearly all patients in this subgroup had moderate to very severe airflow obstruction according to the Global Initiative for chronic Obstructive Lung Disease (GOLD) guidelines.18 Therefore, the specificity of our case definition for COPD is close to 100% in this subgroup. We performed a second sensitivity analysis, in which all participants with missing data were excluded. In a third sensitivity analysis, we constructed a new cohort with the additional criterion that comparator subjects never developed COPD during the study period.
Results
The sample selection flow chart is shown in figure 2 . A total of 149 213 patients fulfilled the case definition of COPD and were followed for at least 5 years prior to the index date. A total of 112 635 COPD/comparator pairs were included following the selection process. 28.3% of patients with COPD received an initial diagnosis of COPD during hospital admission; the remaining were diagnosed in outpatient settings. 12.3% of patients with COPD were matched to a comparator subject who developed COPD later in follow-up. 51.0% of pairs were male, and the mean age on the index date was 68.6 (SD 12.2) years. A descriptive summary of the sample characteristics is shown in table 1.
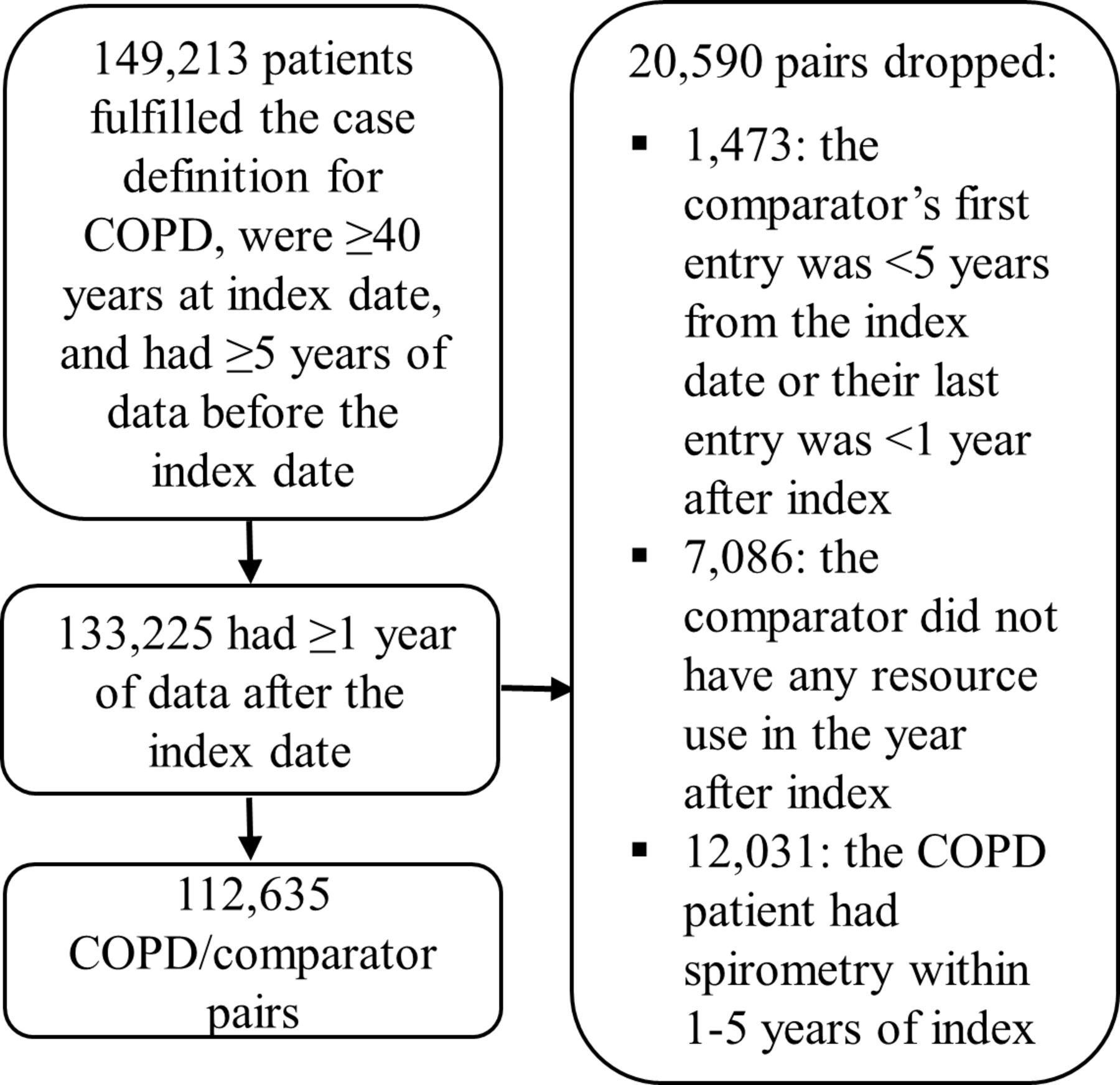
Cohort selection process. COPD, chronic obstructive pulmonary disease.
Characteristics of patients meeting the case definition of COPD and matched comparator subjects
Rate of outpatient encounters
Pharmacist, primary care and specialist physician visits were more common among patients with COPD than comparator subjects throughout the 5-year assessment period (figure 3). In the year prior to being diagnosed, patients with COPD had an average of 17.0 (IQR 5.0–20.0) visits to a pharmacist, 12.6 (IQR 5.0–16.0) primary care visits, 10.5 (IQR 3.0–14.0) specialist visits and 1.8 (IQR 0.0–2.0) visits to a primary care physician for respiratory-related reasons. In contrast, comparator subjects had an average of 10.2 (IQR 3.0–13.0), 8.2 (IQR 3.0–11.0), 6.9 (IQR 2.0–9.0) and 0.5 (IQR 0.0–1.0) pharmacist, primary care, specialist and respiratory-related primary care visits in the year before index, respectively.

Mean number of outpatient visits per patient-year in each of the 5 years before the index date. Patients with COPD and their comparator non-COPD subjects are shown. COPD, chronic obstructive pulmonary disease.
The regression analysis indicated that patients with COPD prior to diagnosis incurred all types of visits at higher rates than comparator subjects (table 2). Relative to comparator subjects, patients with COPD were most likely to visit a primary care physician for respiratory-related reasons (RR 2.17, 95% CI 2.14 to 2.19). COPD and comparator subjects with lower SES had a higher rate of primary care and pharmacist visits. For all outcomes, healthcare visits increased as subjects approached the index date. Models with an additional interaction term between period and the group-defining variable indicated that the rate of primary care visits increased by 8.5% more visits per year (95% CI 8.1% to 8.9%) in COPD than comparator subjects. This figure was 7.3% (95% CI 6.8% to 7.8%) for pharmacist visits, 10.8% (95% CI 10.2% to 11.4%) for specialist visits and 21.9% (95% CI 20.8% to 23.0%) for respiratory-related primary care visits. Coefficients for female, age, SES and calendar year were similar to the main models and are therefore not shown. We observed similar results in the sensitivity analysis of 9079 patients with spirometry-confirmed moderate to very severe COPD near the index date18 (online supplementary e-table 2), for the 110 556 COPD/comparator pairs with no missing data (online supplementary e-table 3), and for the cohort of 106 439 COPD/comparator pairs in which the comparator never developed COPD during follow-up (online supplementary e-table 4).
Parameter estimates* and CIs from the multivariable regression model of the rate of outpatient visits among patients with COPD and comparator non-COPD subjects
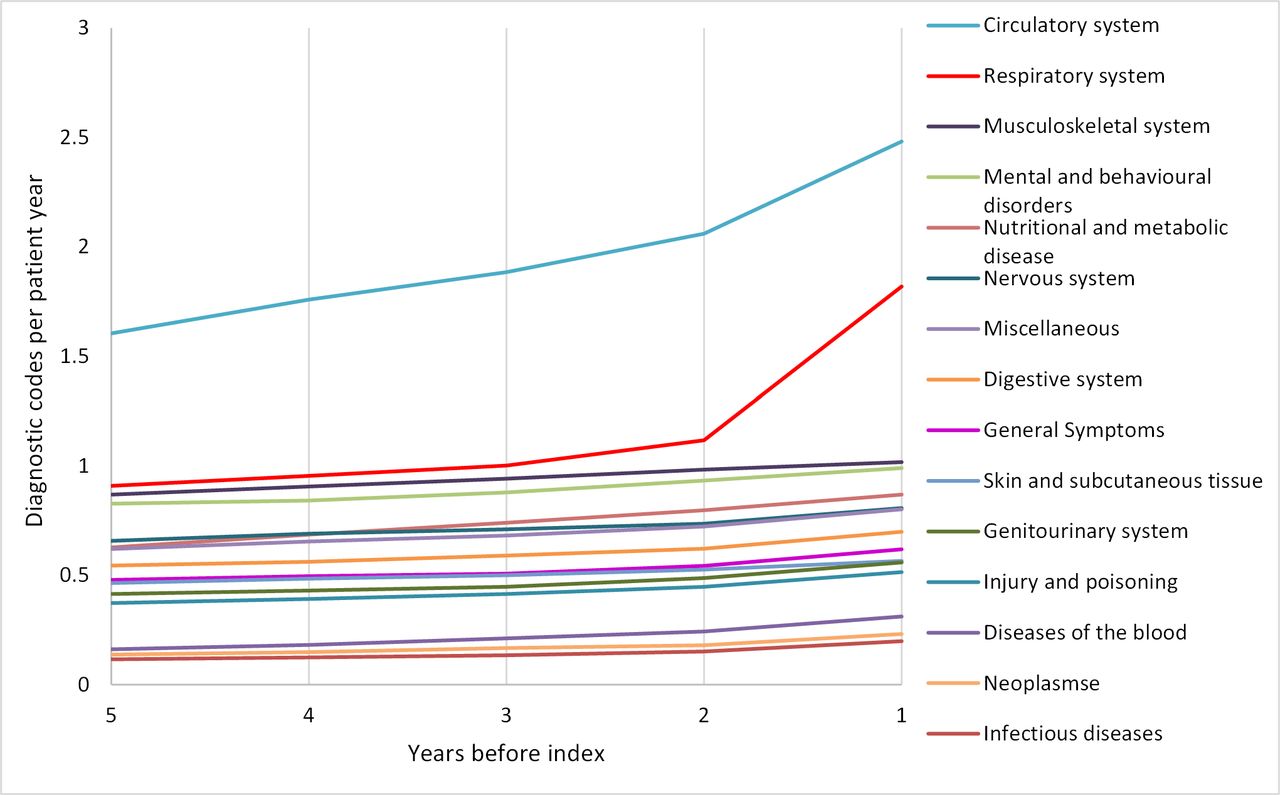
The most common reason for visits to a primary care physician among patients with COPD was circulatory disease (mean of 1.96 diagnostic codes/year, SD 3.77), followed by respiratory disease (1.16 diagnostic codes/year, SD 2.14, figure 4). The frequency of circulatory disease diagnoses increased by 20.4% from 2 years before COPD diagnosis to year 1 before, and by 62.9% for respiratory disease diagnoses over the same time period.

Mean number of ICD diagnostic codesa,b per patient year at the primary care visits of patients with COPD before the index date. aIn 97.7% out of 5 665 378 total visits analysed, there was only one diagnostic code per visit. bDisease categories with less than <0.1 diagnostic codes per year are not shown. COPD, chronic obstructive pulmonary disease; ICD, International Classification of Diseases.
Patients with COPD had a mean of 1.61 (SD 4.48) pharmacist visits per year in which respiratory medications were dispensed (table 3). This increased to 2.46 (SD 5.57) visits in the final year before diagnosis. In contrast, these figures were 0.31 visits/year (SD 1.66) and 0.36 visits (SD 1.86) for comparator subjects, respectively. SABA was the respiratory medication most commonly dispensed to patients with COPD before diagnosis; with a mean of 0.58 (SD 1.96) pharmacist visits with a SABA dispensed per year. Non-respiratory medications were dispensed 53% more frequently to patients with COPD than to comparator subjects.
Mean number of pharmacist visits per 100 patient-years with respiratory and other medications dispensed
Probability of outpatient encounters
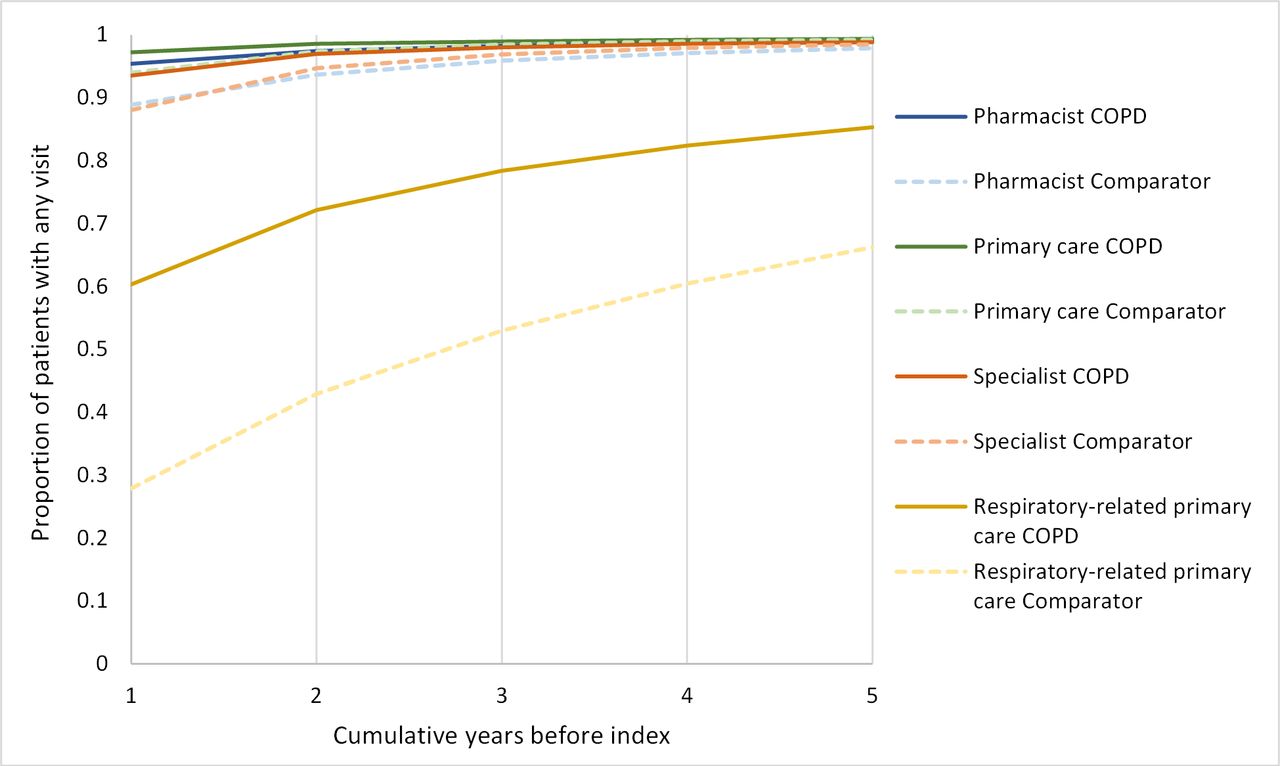
The proportion of patients with COPD that incurred at least one visit in any of the 5 years before the index date was ≥99.0% for pharmacist, primary care and specialist visits, and 85.3% for respiratory-related primary care visits (figure 5). These proportions were similar for comparator subjects, with the exception of fewer respiratory-related primary care visits (66.2%). The highest proportion of patients with COPD visited a primary care physician in the year prior to diagnosis (97.2%), followed by pharmacist (95.4%), specialist (93.6%) and respiratory-related primary care visits (60.3%).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of subjects with at least one outpatient visit in any of the 5 years before index. Patients with COPD and their comparator non-COPD subjects are shown. COPD, chronic obstructive pulmonary disease.
Discussion
We conducted a longitudinal study of healthcare encounters before COPD diagnosis in a sample of the general population. Nearly all patients had at least one encounter in an outpatient setting in the 5 years before they were diagnosed with COPD. They interacted most frequently with pharmacists, followed by primary care physicians, and then with specialist physicians. The rate of visits of every type increased as patients with COPD approached diagnosis, and healthcare encounters were particularly high in the year before diagnosis. Outpatient visits occurred at a substantially higher rate in patients with COPD than in matched non-COPD comparator subjects. Our findings indicate that case detection technologies implemented in primary care settings have frequent opportunities to diagnose COPD earlier.
COPD is a progressive disease that is characterised by airway, and in certain patients, systemic inflammation.19 Due to this inflammation and also to shared risk factors, patients with COPD have higher rates of comorbidities than subjects without the disease.20 Cardiovascular comorbidities are especially common among patients with COPD.21 The most common reason for visiting a primary care physician before being diagnosed with COPD was circulatory disease, followed by respiratory diseases other than COPD or respiratory symptoms. Gershon et al 7 also found that circulatory diseases were the most common reason for outpatient visits in undiagnosed patients with COPD. In our analysis, the frequency of circulatory and respiratory disease diagnoses spiked in the year before COPD diagnosis. The increase in healthcare encounters leading up to diagnosis might reflect these systemic manifestations of the disease. It is also possible that COPD was the underlying cause of some of these circulatory-related visits, as symptoms such as dyspnoea and fatigue are shared between diseases.22 It is likely that these increased encounters were what eventually led to the COPD diagnosis. Increased awareness of the risk of COPD among patients with cardiovascular disease in particular might lead to earlier detection. However, the presence of frequent healthcare encounters is not in itself sufficient to warrant suspicion of COPD, as the pattern of increased healthcare services use leading up to diagnosis is common to other disease areas.23 24 Case detection methods such as risk assessment questionnaires25 26 or screening spirometry27 should be implemented at these types of routine visits in order to identify patients at high risk of having COPD.
Our results indicate that there are substantial opportunities to diagnose COPD earlier. 85% of patients with COPD visited a primary care physician for a respiratory-related reason in the 5 years before they were diagnosed with COPD. This proportion is almost identical to that found by Jones et al 9 in the UK. Moreover, due to our exclusion criteria, none of the patients with COPD in the main analysis received spirometry despite visiting a primary care physician for either respiratory symptoms or other respiratory diseases. Many of these patients were also receiving treatment for respiratory symptoms despite not having been diagnosed with COPD. Influential guidelines, such as GOLD, recommend considering a diagnosis of COPD in patients with respiratory symptoms or risk factors for COPD.18 Risk factors can include other respiratory diseases such as asthma, environmental or early childhood exposures, for example, to childhood respiratory infections, which can result in lung damage long before the clinical manifestation of COPD.28 This suggests that programmes systematically attempting to diagnose COPD earlier through the use of case detection methods have the potential to substantially increase testing for COPD. Given that almost all patients with COPD had at least one respiratory consultation in the 5 years before diagnosis, and many were already receiving respiratory medications, respiratory-related primary care visits might provide particularly high value opportunities for case detection. This type of visit was much more common among patients with COPD than in comparator subjects, which would increase the prior predictive value of any diagnostic test.
Our study has several strengths. We characterised healthcare services use in a large sample of the general population. We used routinely collected data rather than self-reporting by physicians or patients, which is particularly important given that information or recall bias might affect the accuracy of self-reports. A limitation of this study is the lack of data on individual patient characteristics such as spirometry and disease severity, which limited us to studying healthcare services use before COPD diagnosis, rather than in patients with undiagnosed COPD. However, we observed similar results in the subset of patients who had spirometry-confirmed moderate to severe COPD near the time of diagnosis. Our use of a highly specific case definition may have resulted in a sample of patients with more severe COPD and higher healthcare service use than in the general population of patients with undiagnosed COPD. Another limitation is that we only followed patients for 5 years before diagnosis. We imposed this criterion to ensure identical follow-up between matched COPD and comparator subjects while still maintaining a large sample size. The probability of a patient having undiagnosed COPD also decreases as time to diagnosis increases. Finally, our results are most relevant to high-income countries, as more limited access to care could result in lower or no healthcare services use among patients with undiagnosed COPD in low-income and middle-income countries.
Conclusions
We documented frequent interactions between patients with COPD and the healthcare system prior to their date of COPD diagnosis. This suggests that there are many opportunities to implement case detection strategies in outpatient settings, and that it is possible to improve early detection substantially while relying only on opportunistic healthcare encounters. Patients with COPD interacted most frequently with pharmacists before diagnosis, but the greatest difference between COPD and non-COPD subjects was in the rate of primary care visits for respiratory-related reasons. Either of these types of visits might present high value opportunities for case detection. Increased testing for COPD during the routine visits of at-risk patients has the potential to substantially improve early detection. The cost-effectiveness of case detection strategies implemented during outpatient visits should be investigated in a randomised comparator trial or simulation experiment.
Footnotes
Collaborators for the Canadian Respiratory Research Network
Contributors MS, SB and KMJ formulated the study idea. AK prepared the data. KMJ performed all data analyses and wrote the first draft of the manuscript. All authors contributed to interpretation of findings, critically commented on the manuscript and approved the final version. KMJ is the guarantor of the manuscript.
Funding This study was funded by a Canadian Lung Association Breathing as One Studentship Award and the Canadian Institutes of Health Research (application number 142238).
Disclaimer The funders had no role in study design, data collection and analysis, or preparation of the manuscript.
Competing interests DDS has received honoraria for speaking engagements from Boehringer Ingelheim (BI), AstraZeneca (AZ) and Novartis; has served on COPD advisory committees for AZ; Sanofi-Aventis and CSA; and has received research funding from AZ, BI and Merck, outside the submitted work.
Patient consent for publication Not required.
Ethics approval Ethics approval was obtained from Population Data British Columbia (BC) (H13-00684).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data used for this study were provided by British Columbia’s Ministry of Health. These are anonymised health care resource use data of legal residents of the province. The data are protected by the Freedom of Information and Protection of Privacy Act (FIPPA) and as such cannot be shared to any entity outside of the province. FIPPA not only prohibits the storage of personal information outside of Canada, but it also prohibits access, which includes viewing. Please refer to www.popdata.bc.ca/dataaccess/process/analysis/sre for further information. Data requests can be sent to dataaccess@popdata.bc.ca and general enquiries about the data should be addressed to info@popdata.bc.ca.
Linked Articles
- Airwaves