Article Text

Abstract
Background Non-communicable lung disease and exposure to air pollution are major problems in sub-Saharan Africa. A high burden of chronic respiratory symptoms, spirometric abnormalities and air pollution exposures has been found in Malawian adults; whether the same would be true in children is unknown.
Methods This cross-sectional study of children aged 6–8 years, in rural Malawi, included households from communities participating in the Cooking and Pneumonia Study (CAPS), a trial of cleaner-burning biomass-fuelled cookstoves. We assessed; chronic respiratory symptoms, anthropometry, spirometric abnormalities (using Global Lung Initiative equations) and personal carbon monoxide (CO) exposure. Prevalence estimates were calculated, and multivariable analyses were done.
Results We recruited 804 children (mean age 7.1 years, 51.9% female), including 476 (260 intervention; 216 control) from CAPS households. Chronic respiratory symptoms (mainly cough (8.0%) and wheeze (7.1%)) were reported by 16.6% of children. Average height-for-age and weight-for-age z-scores were −1.04 and −1.10, respectively. Spirometric abnormalities (7.1% low forced vital capacity (FVC); 6.3% obstruction) were seen in 13.0% of children. Maximum CO exposure and carboxyhaemoglobin levels (COHb) exceeded WHO guidelines in 50.1% and 68.5% of children, respectively. Children from CAPS intervention households had lower COHb (median 3.50% vs 4.85%, p=0.006) and higher FVC z-scores (−0.22 vs −0.44, p=0.05) than controls.
Conclusion The substantial burden of chronic respiratory symptoms, abnormal spirometry and air pollution exposures in children in rural Malawi is concerning; effective prevention and control strategies are needed. Our finding of potential benefit in CAPS intervention households calls for further research into clean-air interventions to maximise healthy lung development in children.
- paediatric lung disaese
- asthma epidemiology
- paediatric asthma
- lung physiology
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Is the high burden of chronic respiratory morbidity and household air pollution exposure described in Malawian adults, also seen in children, and would a cleaner-burning biomass-fuelled cookstove intervention have a positive effect on lung function in early life?
What is the bottom line?
We found a substantial burden of chronic respiratory symptoms, spirometric abnormalities and carbon monoxide exposures among young children living in rural Malawi, together with a signal of beneficial effect of a cookstove intervention on carboxyhaemoglobin and forced vital capacity.
Why read on?
Chronic respiratory morbidity in adulthood is influenced by lung health in early life—greater understanding of contributing factors is vital to promote healthy lung development during childhood.
Introduction
Non-communicable lung diseases are major global health priorities across the life course.1 2 Asthma is the the most common chronic disease of childhood and one of the the most common chronic diseases of adulthood, affecting around 358 million people while COPD affects 174 million people, worldwide.3
Although most of the children and adults with these conditions live and die in low-income countries and middle-income countries (LMICs), the majority of the research into these conditions is done in high-income countries. Research is especially scarce in the LMICs of sub-Saharan Africa where limited studies suggest the prevalence of childhood asthma is increasing in urban settings, and that children with symptoms of asthma are likely to be severely symptomatic.4 5 In adult populations, Burden of Obstructive Lung Diseases (BOLD) studies from countries in sub-Saharan Africa, including sites in urban and rural Malawi, have found a high burden of impaired lung function—particularly low forced vital capacity (FVC)6–8—which is concerning given the association between low FVC and mortality in other populations.9
In these same sub-Saharan African populations, there is widespread reliance (by around 700 million people) on inefficiently burned solid fuels for cooking, heating and lighting.10 Studies in rural Malawi report exclusive biomass fuel use (wood, crop waste and charcoal) with households using traditional ‘open-fire’ cooking methods.11 The widespread exposure of children to pollutants such carbon monoxide (CO) and particulate matter, resulting from incomplete fuel combustion, is particularly concerning. Household air pollution has been suggested as a potential contributing factor in the development of non-communicable lung diseases in low-income countries.12 However, the links between household air pollution exposure, new-onset asthma in children and obstructive lung disease in adults, are unclear, with controversy over the interpretation of available data.13–17 Environmental exposures, including inhaled pollutants, during periods of lung growth and development may lead to irreversible long term deficits in adult lung function.18 19
In this context, the Cooking and Pneumonia Study (CAPS) was done to determine whether an intervention comprising two cleaner burning biomass-fuelled cookstoves and a solar charger would reduce the incidence of Integrated Management of Childhood Illness-defined pneumonia in children under the age of 5 years in rural Malawi compared with continuation of traditional cooking methods.11 CAPS recruited households from village clusters in Chikhwawa between December 2013 and February 2016. The primary intention-to-treat analysis found no difference in pneumonia incidence between the two trial arms. Recently reported secondary analyses in adults from a subset of CAPS households found no difference in chronic respiratory symptoms, lung function or personal air pollution exposures between participants from the intervention and control groups.20 That said, median exposure to fine particulate matter (PM2.5) was 71 µg/m3, well above WHO annual and 24 hours guidelines.
Is it not known whether the same pattern of respiratory symptoms, spirometric abnormalities and air pollution exposures would be seen in children as in adults or whether the CAPS intervention would have beneficial effects on any of these outcomes in children? In this paper we report the findings of a cross-sectional study, conducted in the same village communities as CAPS, which set out to: (1) measure the prevalence and determinants (including measured exposure to household air pollution) of non-communicable lung disease in a population representative sample of children in rural Malawi and (2) conduct an analysis comparing lung function between young children in the intervention group and those in the control group in CAPS. Some of the data have been previously presented in abstract form.21
Methods
Study design
We conducted a cross-sectional study of the prevalence and determinants of non-communicable respiratory disease among children living in Chikhwawa District, Malawi.
Setting
Chikhwawa is a rural area, located in the Southern Region of Malawi on the Shire River, 50 km from the nearest city, Blantyre. The population consists largely of subsistence farmers living in village communities and is highly vulnerable to climatic shocks, having experienced flooding, crop failures and famine in recent years. Infectious diseases (malaria, pneumonia and gastroenteritis), HIV/AIDS, malnutrition and limited access to basic healthcare contribute to high childhood mortality rates, although a considerable reduction in the mortality rate for children under 5 years old has been seen in Malawi over the past 25 years.22
Participants
Following widespread community engagement events, children aged between 6 and 8 years, living in households that had taken part in CAPS and BOLD-Chikhwawa were identified by local community advisors and invited to participate if the child’s parent/guardian gave written informed consent (or witnessed thumbprint for those unable to read and write). Exclusion criteria were current treatment for tuberculosis, current acute respiratory infection (defined as cough of <1-week duration, associated with fever and/or increased work of breathing) and other contraindications to spirometry (chest or abdominal pain, haemoptysis). We recruited all children from the study area meeting the eligibility criteria.
Procedures
Fieldworkers visited the children in the community to administer an electronic questionnaire, and assess anthropometry, lung function, and personal exposure to household air pollution. An electronic questionnaire was administered in Chichewa, the local language, detailing respiratory symptoms and potential contributing factors. Core written questions from the International Study of Asthma and Allergy in Children (ISAAC) were included, which had been forward and back-translated.23 Height, weight and mid-upper arm circumference (MUAC) were measured according to standardised protocols. Height and weight were interpreted using the WHO 2007 child growth standards.24 MUAC was used to assess nutritional status.25
Prebronchodilator and postbronchodilator spirometry was performed by BOLD centre-certified technicians, according to American Thoracic Society/European Respiratory Society (ATS/ERS) standards using an Easy On-PC Spirometer (ndd Medical Technologies; Zurich, Switzerland).26 Regular calibration was performed according to the manufacturer’s instructions. The highest forced expiratory volume in one second (FEV1) and FVC measurements for each participant were selected (from a maximum eight attempts), before and after administration of 400 µg inhaled salbutamol, via Volumatic spacer. Reversibility was defined as ≥12% improvement between prebronchodilator and postbronchodilator FEV1.
Spirometry over-reading was performed by two independent reviewers. Two sets of ATS/ERS standards (aged 4–6 years and aged seven and above) are relevant for the children in this study.26 27 As the age range of our study children overlaps both sets of standards, and to maximise the use of spirometric data collected, we defined acceptable (grade C) quality as two traces within 150 mL or 10% (online supplementary table S1).
Supplemental material
Carboxyhaemoglobin level (COHb) was measured at a single time-point using a Rad-57 pulse CO-oximeter (Masimo Corporation, California, USA). Performance verification was ensured at study outset, according to the manufacturer service manual. To assess personal CO exposure levels, children wore an EasyLog CO USB data logger (Lascar Electronics, Wiltshire, UK), for up to 48 hours, starting immediately after the field visit.
Variables
Clinical outcomes were presence or absence of symptoms, as assessed by the following questions; Chronic cough: defined by a positive response to both ‘Does your child usually have a cough when they don’t have a cold?’ and ‘Are there months in which they cough on most days?’; Current wheeze: ‘Has your child had wheezing or whistling in the chest in the past 12 months?’; Severe asthma: current wheeze, and ≥4 attacks of wheeze, or ≥1 night per week sleep disturbance from wheeze, or wheeze affecting speech, in the past 12 months; Shortness of breath: a composite outcome, positive if children were reported to be breathless during normal daily activities or on minimal exertion; Any respiratory symptom: a composite outcome, positive if a participant was reported to have any of the previously described symptom outcomes.
Continuous FEV1 and FVC values were used in the primary analysis. Standardised z-scores and lower limits of normal (LLN) for FEV1, FVC and FEV1/FVC were derived from the GLI 2012 reference equations for African-Americans, which provide race-specific and sex-specific reference values, taking into account height and age.28
Personal CO exposure monitoring data were not analysed if <24 hours were recorded. To allow comparison of varying lengths of recording, all data were truncated at 24 hours for the final analysis.
Potential effect modifiers included were height (cm), weight (kg), age and sex.
Study size
We calculated a sample of 600 participants (300 male, 300 female) would estimate the prevalence of non-communicable lung disease in each sex stratum with a precision (95% CI) of ±3.3 to ±5.0% (assuming a prevalence of 10%–25%). To allow for unequal sex distributions, refusals and inability to provide spirometry of acceptable quality, we aimed to recruit 1000 children.
Statistical analysis
Descriptive analysis was performed, using Student’s t-test and Pearson’s χ2 to compare continuous and categorical data. For population proportions, Wald-type SEs were calculated, assuming a binomial distribution. Bivariate associations between spirometric and clinical outcomes, and variables including CO, COHb, hospital admission for respiratory illness during infancy, and CAPS allocation were explored. Harmonic regression was used to account for any possible effect of seasonality on the outcome measures. This was implemented by including sinusoidal functions (sine and cosine terms) of time with a period of 1 year. Linear multivariable regression was used to estimate the association between exposures and continuous lung function values (FEV1 and FVC). Multivariable logistic regression models were constructed for dichotomous clinical outcomes. All models included age, sex, height and weight a priori, and variables with a p value <0.2 on bivariate analysis. A backward stepwise regression technique was used to develop multivariable models. An analysis was conducted to compare FEV1, FVC and FEV1/FVC, symptom prevalence and exposure variables between the intervention and control groups of CAPS. CO was log10 transformed for inclusion in linear models to ensure normality of residuals.
Analyses were conducted using R V.3.4.1 statistical software.29
Role of the funding source
The funders had no role in the study design, data collection, analysis, interpretation or writing of the report. The corresponding author had full access to all the study data and had final responsibility for the decision to submit for publication.
Ethical approval was given by the College of Medicine Research Ethics Committee in Malawi (reference P.07/16/1994) and Liverpool School of Tropical Medicine Research Ethics Committee in the UK (reference 16–040).
Results
Between February and December 2017, we approached 886 children of whom 804 were confirmed to be eligible and were recruited (79/82 were outside the eligible age range; 3/82 guardians declined to consent). Questionnaire data were collected for all but one participant who withdrew from the study shortly after giving consent. Anthropometry, spirometry, COHb measurement and personal CO monitoring were done on 99.9% (802/803), 99.9% (802/803), 99.4% (798/803) and 99.3% (797/803) of these participants, respectively. Grade A–C prebronchodilator traces were achieved in 65% (522/802) of the children. The duration of CO monitoring was 24 and 48 hours for 91.9% (738/803) and 79.5% (638/803) children, respectively. There were 476 (260 intervention and 216 control) children from households included in CAPS (figure 1).

Participant recruitment flow diagram. CAPS, Cooking and Pneumonia Study; CO, carbon monoxide; COHb, carboxyhaemoglobin level.
The mean age (SD) of participants was 7.13 (0.77) years and 417 (51.9%) participants were female. Most (700 (87.2%)) were attending primary school. The mean (SD) height-for-age and weight-for-age z-scores were −1.04 (0.90) and −1.10 (0.89), respectively. Mean (SD) MUAC was 15.98 (1.26) cm (table 1). No children met the criteria for severe or moderate acute malnutrition, but 11/789 (1.4%) children were ‘at risk for acute malnutrition’.
Demographics and clinical characteristics (n=803)
Chronic respiratory symptoms were reported by 133 (16.6% (SE 1.3)) children, most commonly cough (8.0% (SE 1.0)), and current wheeze (7.1% (SE 0.9)) (table 1). One-fifth (159/803) of children had been admitted to hospital with respiratory symptoms in the past; on one (9.7%), two (6.1%) and three or more (4.0%) occasions. Admission for a respiratory problem during the first year of life was reported for 70 (8.7%) children. Antibiotic use for a chest problem in the last year was common, reported for 112 (13.9%) children, with 69 (8.6%) receiving these on more than one occasion. Half (54.4%) of children with current wheeze had symptoms of severe asthma, representing 3.9% of children overall. Of these, 22 (71.0%) had a previous hospital admission, and 10 (32.2%) missed school due to breathing problems. Very few (0.4%) children had previously been treated for tuberculosis, and 2.0% (6/307) of children who had been tested for HIV were HIV-positive.
Children producing grade A–C spirometry were older than those with unacceptable traces (mean age 7.23 vs 6.96 years, p<0.001); otherwise there were no significant differences in growth parameters and respiratory symptoms between the two groups (online supplementary table S2). Overall, participants had a mean (SD) FEV1 z-score −0.48 (0.93) and mean (SD) FVC z-score of −0.30 (0.96). Children from CAPS intervention households had higher FVC z-scores than those from control households (−0.22 vs −0.44, p=0.05). Prebronchodilator spirometric abnormalities were found in 68/522 (13.0%) of children; 7.1% with low FVC and 6.3% obstruction (table 2). Postbronchodilator spirometry was attempted by 706 children, with 72% (505/706) producing grade A–C traces. Both prebronchodilator and postbronchodilator traces were available for 432 children, 26 of whom had a prebronchodilator FEV1/FVC ratio below the LLN which was reversible in 8 (30.7%).
Prebronchodilator lung function parameters for participants with grade A–C spirometry, including the CAPS subgroup
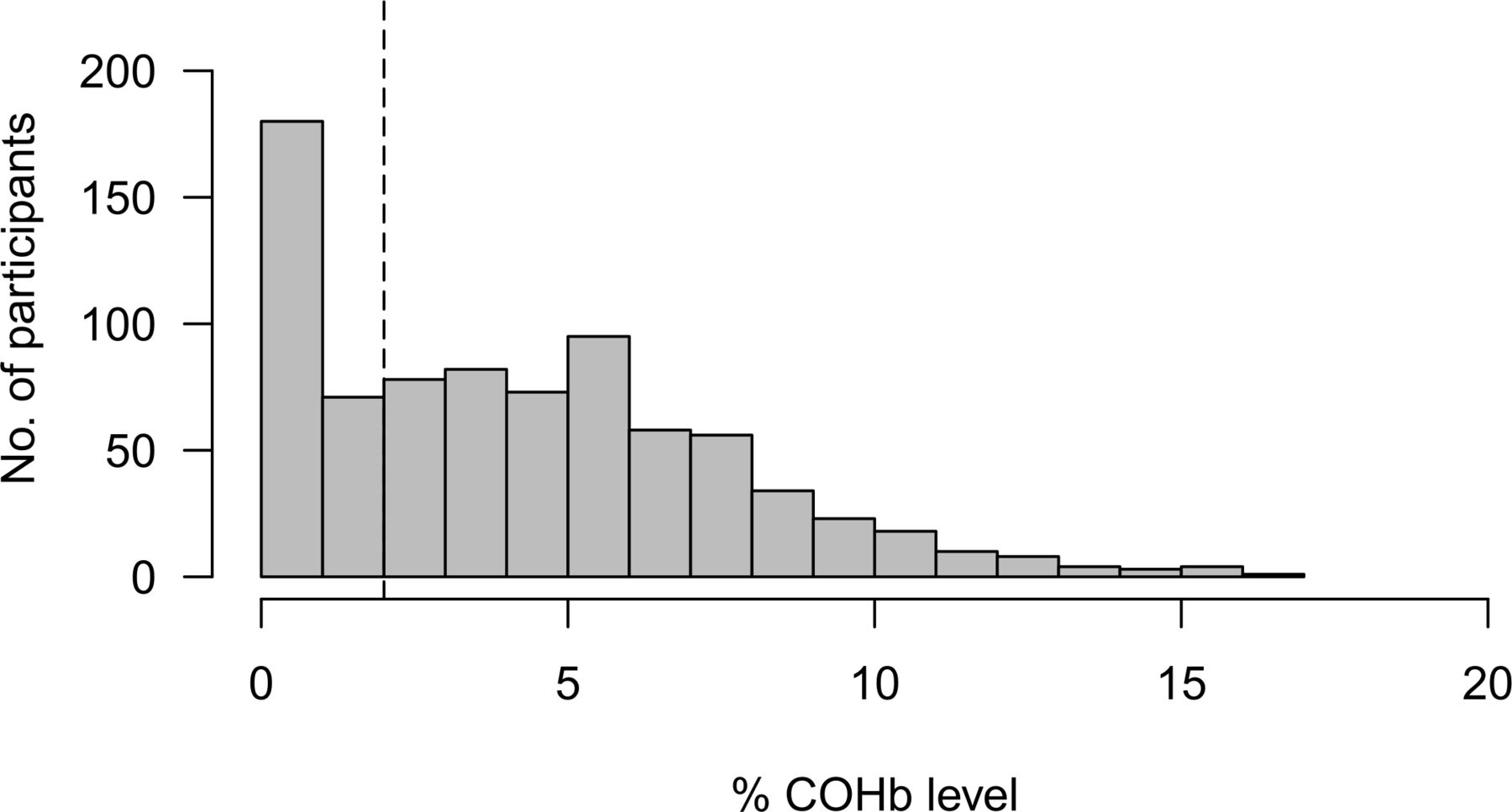
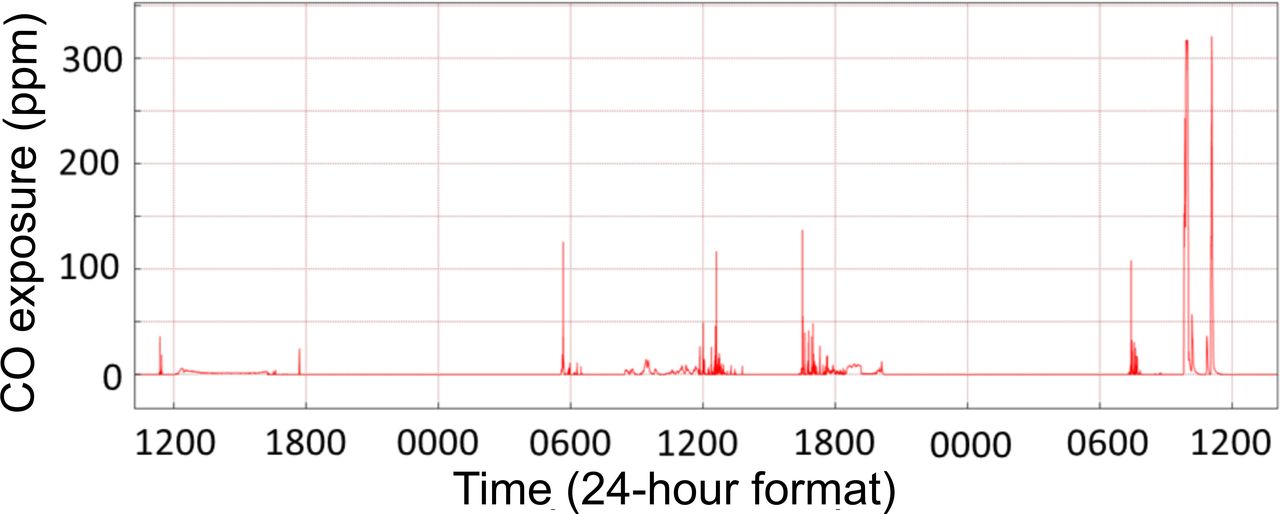
Personal CO monitoring showed considerable variation in exposure throughout the monitored period (figure 2). Mean exposure levels ranged from 0 to 15.1 parts per million (ppm), with a median CO exposure of 0.20 ppm (IQR 0.07–0.54). Peaks exceeding the 15 min indoor WHO guideline (81 ppm; 100 mg/m3) were observed in 370/738 (50.1%) of participants (figure 3).30 Median %COHb was 4.00 (IQR 1.50–6.50). 68.5% of participants had a level greater than 2%, and 6.0% greater than 10% (figure 4). We found no association between respiratory symptoms or spirometric indices and personal CO and COHb measurements in bivariate analyses and therefore these variables were not carried forward into multivariable analysis. In logistic multivariable analysis, chronic cough (OR 2.63 (95% CI 1.13 to 6.12)), current wheeze (OR 5.48 (95% CI 2.45 to 12.26)) and symptoms of severe asthma (OR 6.36 (95% CI 2.34 to 17.28)) were all associated with hospital admission during infancy (table 3). We found no association between respiratory symptoms and spirometric indices in bivariate or multivariable analysis (table 3).
OR (95% CI) for chronic respiratory symptoms estimated by multivariable logistic regression (n=522)

Example of a typical 48 hours CO monitoring trace. CO, carbon monoxide.

Maximum CO levels recorded during monitoring period for 738 participants. Dashed line represents who recommended indoor exposure guideline for a 15 min time period. CO, carbon monoxide.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of COHb level for 798 participants. Dashed line represents the WHO COHb guideline. COHb, carboxyhaemoglobin level.
In the analysis comparing intervention and control groups, we found statistically significant associations between the intervention arm and both FVC (coefficient estimate 0.04 (95% CI 0.00 to 0.07)), and COHb level (coefficient estimate −0.89 (95% CI −1.53 to 0.26) (table 4A). We found no significant differences between CAPS arms for growth parameters (table 4A) or chronic respiratory symptom rates (table 4B).
CAPS secondary trial analyses: mean or median values, with linear model coefficient estimates (95% CI) for continuous outcomes
CAPS secondary trial analyses: proportions and OR (95% CI) for symptom outcomes (n=476)
Discussion
This is one of the first studies to report lung function and personal household air pollution exposure, measured concurrently in young children, and it was conducted in the context of the largest trial of a cleaner-burning cookstove intervention to date. Among children living in rural Malawi, we found that; one in six reported chronic respiratory symptoms; over half with current wheeze had severe symptoms; anthropometric and lung function parameters were generally decreased compared with global reference ranges; the majority of children had COHb levels above WHO recommended guidelines; and half of children exceeded WHO guidelines for CO exposure (100 mg/m3), during 24 hours monitoring.10 Overall, we found no evidence of an association between CO exposure and respiratory symptoms or lung function. However, children from CAPS intervention households had higher FVC z-scores and lower COHb levels than controls.
There are limited data regarding chronic respiratory symptoms in children from Africa, and particularly rural settings. One study from rural Senegal reported similar rates with 9% current wheeze and 5% severe asthma among children aged 5–8 years.31 Studies from urban settings in sub-Saharan Africa, including ISAAC sites, reported rates of current wheeze in 5%–16% of young children, with symptoms of severe asthma in half of these.4 32–34 Globally 11.5% of children aged 6–7 years have current wheeze, and 4.9% have symptoms of severe asthma; severe symptoms are seen in one-third of children with current wheeze in Europe.4 The high rates of severe symptoms seen in low-income countries are concerning, and likely reflect multiple challenges within healthcare systems, which are better equipped to manage acute episodes relating to infectious diseases, rather than chronic non-communicable conditions. In keeping with this, recent research from Nigeria and South Africa has reported high rates of under-diagnosed and untreated asthma in schoolchildren.35 36
We found decreased lung function parameters in this study, comparable to values reported for community controls in a recent study exploring long-term outcomes after severe acute malnutrition, at the referral hospital in Blantyre, Malawi.37 These lung function deficits, when compared with international reference ranges, may reflect host and environmental factors such as undernutrition, frequent respiratory infections, low birth weight, exposure to pollutants in utero and early life, which can have adverse effects on lung growth and development.38–42 No children in this study were acutely malnourished (as defined by MUAC measurement), although other anthropometric parameters (weight-for-age and height-for-age z-scores) were reduced compared with international standards, suggesting a level of chronic undernutrition in this community. There are limited data regarding normal lung function in healthy African paediatric populations, and consequently it is difficult to understand the clinical significance of these apparent spirometric deficits.43 Further research is needed to describe optimal lung growth in African populations, and determine the morbidity and mortality associated with lung function abnormalities.44
Consistent with our previous findings in Chikhwawa, we noted exposure to high peaks of CO, reaching up to three times the WHO guidelines around cooking times, although mean and median levels were low; median CO 1.23 ppm (IQR 0.79–1.93) in adults and mean CO 1.27 ppm (SD 2.79) in younger children.20 45 Median CO exposure levels were lower (0.20 ppm (IQR 0.07–0.54) in our older paediatric population perhaps reflecting long periods of time that children spend away from the home environment during the school day. Cookstove trial analyses exploring adult lung function as a secondary outcome have found no evidence of intervention benefit.20 46 47 Paediatric lung function outcomes in cookstove trials are inconclusive, but signal a possible beneficial effect of the interventions. Secondary analysis from the RESPIRE trial found decreased lung growth at around 5 years of age (measured by peak expiratory flow), associated with delayed chimney stove installation, although there was no association between lung function at age five and measured personal CO exposure during the first 18 months of life.48 The GRAPHS birth cohort in rural Ghana recently reported an association between prenatal CO exposure and infant lung function at 30 days of life, with an increased effect of exposure on female infants.49 Cross-sectional studies from Nigeria have described decreased lung volumes (FEV1 and FVC) and increased asthma symptoms in children with self-reported exposure to biomass cooking fuels.36 50
The association between CAPS intervention group and higher FVC is interesting, given the lack of evidence for an association between lung function and CO exposure or COHb level. This positive finding must be interpreted cautiously as it is the result of exploratory secondary analyses, unadjusted for multiplicity and therefore may be due to chance. However, when taken with the second signal of a potential effect, lower COHb observed in the intervention group, the results may be evidence of a genuine impact. We may have observed a benefit among our participants, who were aged 3–6 years during the CAPS trial period, in contrast to findings from adult populations, because the early childhood years represent a key period for lung development. There is rapid alveolar expansion and resulting lung growth during the first 2 years of life, which stabilises around 8 years of age.51 Alveolar number is reflected by FVC in childhood and so it is biologically plausible that we might see improved lung function in children from the intervention arm; the apparent difference of 70 mL in mean FVC between CAPS groups represents approximately 6% of a child’s lung volume. Furthermore, young children have increased susceptibility to air pollutants, exhibiting increased deposition of particles in the lung, due to physiological and anatomical factors.52 CO exposure measures do not appear to be associated with lung function or respiratory symptoms—perhaps CO is an inadequate proxy for other pollutants of interest, such as PM2.5 and nitrogen dioxide. Our previous air pollution monitoring work in Chikhwawa has demonstrated that monitored CO exposure correlates weakly with COHb, PM2.5 exposure, and measured black carbon in airway cells from induced sputum.20 45 53
This study was conducted in the context of the largest cookstove intervention trial to date—a major strength enabling us to assess the effect of a cookstove intervention on childhood spirometry and air pollution exposure outcomes. Other strengths include high participation rates for spirometry and CO exposure monitoring, and good quality spirometry in a representative sample of children, despite the highly challenging research environment of a rural area in a low-income country. We achieved our sample size, even though field work was disrupted by vampirism hysteria in the community. We acknowledge limitations to our study including that personal monitoring of CO for 48 hours provides only a snapshot of exposure to a single pollutant. There are substantial limitations to the methods currently available for monitoring personal exposure to other pollutants in this young age group; the Lascar CO-monitoring device represents one of the best options available, at present. Monitoring during a 48 hours exposure period may not describe individual variation in daily and seasonal routines but reflected a compromise in terms of feasibility and acceptability in this large study population. Questionnaire data may have been subject to recall bias, with limited information on contributing factors such as birth weight, gestation at birth, HIV-status and exposure to passive smoking.
In conclusion, the substantial burden of chronic respiratory symptoms, abnormal spirometry and air pollution exposures in children in rural Malawi is concerning and calls for strategies to maximise healthy lung development and to effectively manage chronic respiratory conditions. To achieve this, research will be needed to develop ways to increase awareness of non-communicable lung diseases, such as asthma, at a community level to inform healthcare seeking behaviours and ensure access to appropriately trained healthcare providers and effective long-term treatment such as inhaled medication. Our finding of a potential beneficial effect of a cleaner burning biomass-fuelled cookstove on lung function (FVC) calls for further research into clean-air initiatives, tackling multiple sources of air pollution in a community-wide approach to promote lung health in children.
Acknowledgments
We thank the study participants, village leaders and community representatives, the study team in Chikhwawa, MLW and LSTM, the CAPS trial steering committee and data monitoring committee, the Malawi Ministry of Health, and the African Clean Energy (ACE) company for their valued contributions to making this work a success.
References
Footnotes
Contributors Design: KM, JG, SR. Acquisition of data: SR, RN, AN, FM, KM. Analysis of data: SR, RN, CJ, JG, KM. Interpretation of data: SR, RN, CJ, JRB, JG, KM. Writing the manuscript, approval of the version to be published and agreement to be accountable for all aspects of the work: All authors.
Funding This work was funded by a Research Grant from the Medical Research Foundation (Ref: MRF-021-0001-RG-MORTI), a New Investigator Research Grant from the Medical Research Council (Ref: MR/L002515/1), a Joint Global Health Trials Grant from the Medical Research Council, UK Department for International Development and Wellcome Trust (Ref: MR/K006533/1) and the Medical Research Council Doctoral Training Programme at the Liverpool School of Tropical Medicine and University of Lancaster (Ref: MR/N013514/1). Additional support was provided by the NIHR Global Health Research Unit on Lung Health and TB in Africa at LSTM—'IMPALA'. In relation to IMPALA (grant number 16/136/35) specifically: IMPALA was commissioned by the National Institute of Health Research using Official Development Assistance (ODA) funding. The views expressed in this publication are those of the author(s) and not necessarily those of the National Institute for Health Research or the Department of Health.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was given by the College of Medicine Research Ethics Committee in Malawi (reference P.07/16/1994) and Liverpool School of Tropical Medicine Research Ethics Committee in the UK (reference 16-040).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.