Article Text

Abstract
Introduction Breathlessness is common in the population, especially in women and associated with adverse health outcomes. Obesity (body mass index (BMI) >30 kg/m2) is rapidly increasing globally and its impact on breathlessness is unclear.
Methods This population-based study aimed primarily to evaluate the association of current BMI and self-reported change in BMI since age 20 with breathlessness (modified Research Council score ≥1) in the middle-aged population. Secondary aims were to evaluate factors that contribute to breathlessness in obesity, including the interaction with spirometric lung volume and sex.
Results We included 13 437 individuals; mean age 57.5 years; 52.5% women; mean BMI 26.8 (SD 4.3); mean BMI increase since age 20 was 5.0 kg/m2; and 1283 (9.6%) reported breathlessness. Obesity was strongly associated with increased breathlessness, OR 3.54 (95% CI, 3.03 to 4.13) independent of age, sex, smoking, airflow obstruction, exercise level and the presence of comorbidities. The association between BMI and breathlessness was modified by lung volume; the increase in breathlessness prevalence with higher BMI was steeper for individuals with lower forced vital capacity (FVC). The higher breathlessness prevalence in obese women than men (27.4% vs 12.5%; p<0.001) was related to their lower FVC. Irrespective of current BMI and confounders, individuals who had increased in BMI since age 20 had more breathlessness.
Conclusion Breathlessness is independently associated with obesity and with weight gain in adult life, and the association is stronger for individuals with lower lung volumes.
- dyspnoea
- sex
- weight
- lung function
- lung volume
Statistics from Altmetric.com
Key messages
What is the key question?
Do people with higher current body mass index (BMI) or who have increased in BMI since age 20 suffer from more breathlessness in their daily life, and which factors contribute to this increased risk?
What is the bottom line?
Both higher BMI and increase in BMI since age 20 were independently and strongly associated with increased breathlessness, and the adverse effect was stronger for individuals with lower lung volumes.
Why read on?
Obesity and breathlessness are increasing problems globally, and this is a large national population-based study that provides novel knowledge on the relation between obesity and breathlessness including differences between men and women.
Introduction
Breathlessness related to daily activities affects 15%–45% of middle-aged people in the population and is associated with major adverse health outcomes.1–4 Breathlessness during daily life is markedly more common in women than men, both among healthy and in people with chronic obstructive pulmonary disease (COPD). This sex-related difference was recently related to the lower absolute lung volumes in women.1 5 6 There is a need to further identify factors that influence the sensation of breathlessness.
Obesity prevalence has increased steeply in recent decades.7 In 2016, over 650 million adults were obese, defined as having a body mass index (BMI) >30 kg/m2, according to the WHO.7 8 The majority of adults in the USA are now overweight or obese.7 Obesity is associated with negative health effects, including increased comorbidity and healthcare utilisation, mainly related to the metabolic syndrome and cardiovascular disease,9 10 heart failure,11 sleep problems,12 impaired physical and mental health-related quality of life13 and increased mortality.14
Obesity is associated with markedly increased prevalence and severity of activity-related breathlessness in the community.1 3–6 10 15–19 People with obesity have a 3.6-fold increased risk of breathlessness independent of age, sex, ethnicity and level of airflow obstruction.16 In one study, 80% of obese adults reported breathlessness after climbing two flights of stairs compared with 16% of non-obese controls.10 An association between higher BMI and increased activity-related breathlessness, measured using the modified Medical Research Council (mMRC) breathlessness scale,17 20 is reported across countries and regions.1 3–6 18
Knowledge on the link between obesity and breathlessness in the general population is limited. No study has evaluated the relation between prior change in BMI over time and current breathlessness. Regardless of BMI, weight gain is an independent risk factor for other subjective symptoms such as insomnia and daytime sleepiness.12 Whether other markers of central obesity, such as waist circumference, are more strongly related to breathlessness than BMI has not been evaluated. It is also unknown to what extent the association between obesity and breathlessness is mediated by related changes in other key factors such as comorbidities and reduced lung volumes.
The primary aim of this study was to evaluate the association of obesity indicators: BMI, change in BMI since age 20 and central obesity, with activity-related breathlessness in the middle-aged general population. Secondary aims were to (1) compare the accuracy of associations between different obesity indicators; (2) evaluate to what extent the associations are due to potential confounders including comorbidities and to (3) untangle the interplay of obesity, comorbidities and reduced spirometric lung volumes in relation to breathlessness in men and women.
Methods
Study design and population
This was a cross-sectional analysis of the population-based Swedish CArdioPulmonary bioImage Study (SCAPIS).21 SCAPIS is a collaborative research project between six Swedish universities (Gothenburg, Linköping, Malmö/Lund, Stockholm, Umeå and Uppsala). The overall goal of SCAPIS is to characterise, in terms of phenotype and environmental and socio‐economic influences, a Swedish cohort of 30 000 men and women aged 50–64 years, to obtain novel information that is relevant in today's environment to identify and treat individuals with cardiopulmonary and metabolic diseases and to optimise the ability to investigate disease mechanisms.21 Participants were randomly selected from the Swedish population register, and the participation rate was around 50%. The present analysis is based on data from the SCAPIS cohort included between November 2013 and December 2016.
Exclusion criteria in the present study were inability to walk due to other reasons than breathlessness and missing data on self-reported breathlessness or any of the evaluated study variables.
Assessments
Self-reported questionnaire data included mMRC, weight at age 20, smoking status, pack-years of smoking (number of cigarettes/20/day×years of smoking), loss of menses due to menopaus, doctor’s diagnoses of hypertension, diabetes mellitus, asthma, COPD, sleep apnoea, ischaemic heart disease (previous myocardial infarction and/or angina pectoris), heart failure, atrial fibrillation/flutter and stroke. Heart disease was defined as the presence of any of ischaemic heart disease, heart failure or atrial fibrillation/flutter.
Frequency of anxiety was assessed by a 5-point score adapted from Rosengren et al , and scores 4–5 were used to define anxiety.22 23 Depression was assessed by asking whether, during the past 12 months, the participant had felt sad, blue or depressed for 2 weeks or more in a row, and if yes, graded by a set of seven yes/no questions—lose interest in things, feel tired or low on energy, gain or lose weight, trouble falling asleep, trouble concentrating, think of death, feeling worthless, of which five or more positive responses were defined as clinical depression.23
The participants’ level of physical exercise during leisure time was analysed by four questions adopted from the Public Health Agency of Sweden.24 Based on the responses, participants were categorised as having a high (regular hard exercise >30 min, >3 times/week), medium (exercise such as walking or cycling for at least 4 hours per week) or low (spending most leisure time at sedentary activities with light physical exercise <2 hours per week) level of physical exercise.
Height, weight, waist and hip circumference were measured at the test centres. Current BMI was calculated as weight (kg)/height(m)2. BMI at age 20 was calculated using the participant recalled weight at age 20 and the current height (recalled height was not obtained). The waist–hip ratio (WHR) was calculated and a high WHR was defined according to the WHO criteria as >0.9 for men and >0.85 for women.25
Dynamic spirometry (forced expiratory volume in one second (FEV1) and forced vital capacity (FVC)) and carbon monoxide (CO) uptake (diffusion lung capacity for CO (DLCO)) were performed with a Vyaire (Mettawa, IL, USA). Spirometry was carried out at least 15 min after inhalation of 400 µg of salbutamol, using a nose clamp and with the subject in the sitting position. CO uptake was determined using the single breath method. All procedures were performed according to American Thoracic Society (ATS)/European Respiratory Society (ERS) standards.26 27 Predicted spirometry values and z-scores were calculated using the Global Lung Function Initiative 2012 reference values.28 29
Statistical analyses
Characteristics were summarised using mean with SD and median with range or IQR for continuous variables with normal and skewed distribution, respectively. Categorical variables were expressed as frequencies and percentages. Characteristics were tabulated for individuals included and excluded from the analysis, separately.
Outcome was activity-related breathlessness defined as a mMRC breathlessness score ≥1.17 mMRC is reliable, valid and the most commonly used scale for categorising the functional impact and disability from breathlessness in daily life,17 30 including in people with obesity.20 A single cut-off was used for simplicity, as ordinal analysis using all 0–4 mMRC categories yielded similar findings.
Obesity indicators of interest were as follows: (1) measured current BMI categorised as <20, 20 to <25, 25 to <30 and ≥30 kg/m2; (2) absolute change in BMI since age 20; (3) mean change per year in BMI since age 20; (4) measured waist circumference (cm); (5) central obesity defined as a waist circumference >102 cm for men and >88 cm for women.25
The associations between each obesity indicator and breathlessness were analysed using multivariable logistic regression. All models accounted for clustering by centre (n=6). Associations were expressed as ORs with 95% CIs. Robustness of the logistic models was supported by that analysis using ordinal and multinominal logistic regression yielded similar findings. Model fit evaluated using Hosmer Lemeshow’s test was good for the models (p>0.11) but was lower (p=0.04) for central obesity.
Covariates were selected for inclusion in the regression models based on subject matter knowledge.1 3–6 18 19 Evaluated potential confounders were age, sex, waist circumference, WHR, level of airflow limitation (FEV1/FVC z-score), FVC z-score, DLCO, self-reported presence of physician-diagnosed hypertension, diabetes mellitus, heart disease, pack-years of smoking, current smoking (with missing as separate category), anxiety, depression, menopause (in women) and level of physical exercise. Relations between study variables and the minimal required set of variables to adjust were evaluated using a directed acyclical graph (www.dagitty.net) shown in figure S1 in the online supplement. Covariates in the final adjusted models were age, sex, current smoking, FEV1/FVC z-score, asthma, hypertension, heart failure, anxiety, depression and level of physical exercise. Lung function was evaluated as FVC and not DLCO based on a previous analysis that the relation between DLCO and the sex difference in breathlessness was mainly related to women’s lower lung volumes (measured using FVC).6
Supplemental material
The shape of the association between each obesity indicator and breathlessness was evaluated visually using box plots and splines for correct specification of the variables in the models. No data were imputed. The accuracy of the associations between obesity indicators and breathlessness was compared using the area under the curve (AUC) of each model, crude and adjusted for confounders.
The influence of spirometric lung volumes was evaluated by comparing the estimate for the obesity indicators in fully adjusted models with and without FVC in absolute value and z-score (deviation from the predicted normal), respectively. Whether associations between current BMI and breathlessness differed between men and women, by the BMI at age 20 and by FVC, was tested by adding interaction terms separately in the fully adjusted model. Interaction was evaluated using likelihood ratio tests. Associations with the breathlessness probability were plotted as the marginal effects from the models using the command ‘marginsplot’ in Stata. All the analyses were conducted using Stata V.14.2 (StataCorp LP; College Station, TX, USA, 2016). Statistical significance was defined as a two-sided p<0.05.
Results
After excluding those with inability to walk due to other reason than breathlessness (n=144) and missing data on self-reported breathlessness or any of the evaluated study variables (n=2373), 13 437 individuals were included in the analysis.
Compared with the included participants, excluded individuals reported more breathlessness, had slightly higher BMI, more previous and current smoking and slightly more comorbidities (Table S1 in the online supplement). Characteristics of included individuals are shown in table 1; mean age was 57.5 (SD 4.3); 52.5% women; mean current BMI was 26.8 (SD 4.3); mean BMI at age 20 was 21.9 (SD 2.7) and 9.6% reported breathlessness (mMRC ≥1).
Characteristics of participants
Individuals with breathlessness were more likely to be women (67% vs 51%), had similar BMI at age 20 as compared with people without breathlessness but had higher current BMI and more central obesity, higher smoking exposure, more comorbidities, less physical exercise and lower spirometric lung function than individuals without breathlessness (table 1). The current BMI stratified by BMI at age 20 is shown in Table S2 in the online supplement. Generally, the BMI had increased over time. Among individuals with a normal BMI at age 20, 48% had become overweight and 19% obese. Among obese individuals, women had markedly more breathlessness than men (27.4% vs 12.5%; p<0.001).
Current BMI was associated with activity-related breathlessness, in an expected U-shaped relationship (table 2). Associations with breathlessness were also seen for the other obesity indicators.
Associations of obesity factors with breathlessness
The accuracy of the associations with breathlessness (measured using AUC) was similar for the different obesity indicators in the models, which correctly classified the presence of breathlessness in 63.1%–69.4% of individuals (AUC range: 0.631–0.694) (table 2). The predictive power of the models increased when adjusting for confounders, with no substantial differences between the obesity indicators. The associations between obesity (for the different indicators) and breathlessness decreased only slightly and remained highly statistically significant when controlling for differences in FVC (both absolute value and % of predicted) (table 2).
Adjusting for potential confounders (age, sex, current smoking, FEV1/FVC z-score, asthma, hypertension, heart failure, anxiety, depression and level of physical exercise), the associations between the obesity indicators and breathlessness remained largely unchanged (table 2). The same was true also when adding FVC (absolute value or % of predicted) to the model, indicating that only a minor part of the associations between obesity and breathlessness was mediated through a reduction in FVC.
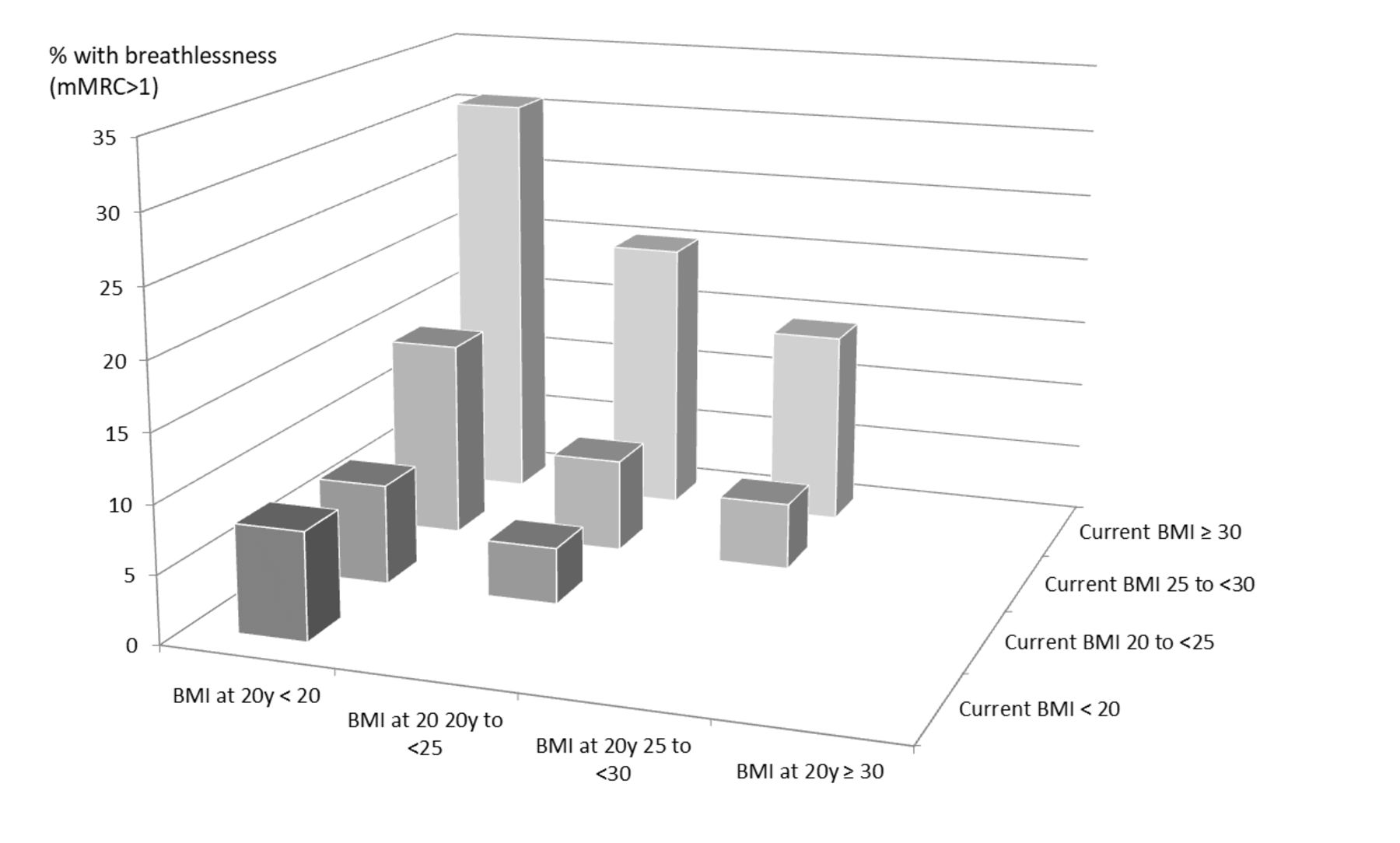
Irrespective of the current BMI, a larger increase in BMI since age 20 was associated with higher breathlessness prevalence (figure 1). Current BMI and change in BMI since age 20 were independently associated with breathlessness when analysed separately (table 2). In addition, both factors were independently associated with breathlessness when adjusting for confounders and each other; for current BMI<20 (OR 1.62, 95% CI: 0.95–2.76); BMI 25 to <30 (OR 1.14; 95% CI: 1.04–1.26) and BMI≥30 (OR 1.67; 95% CI: 1.38–2.02) compared with the reference BMI of 20 to <25; and for change in BMI since age 20, adjusted OR 1.10 (95% CI, 1.09 to 1.11). There was no evidence of an effect modification between current BMI and change in BMI since age 20 (p=0.51 for interaction). Individuals who had decreased more than one unit in BMI since age 20 (n=350; 2.6%) showed a trend of increased breathlessness (OR 2.04; 95% CI, 1.51 to 2.76) compared with people who had remained stable in weight (BMI within 1 unit of the value at age 20), but a decrease in BMI was not associated with breathlessness in the multivariable analysis, adjusted OR 1.14 (95% CI: 0.83–1.56). Individuals who had increased in BMI since age 20 had higher current waist circumference, more central obesity, and were more inactive (Table S3 in the online supplement).
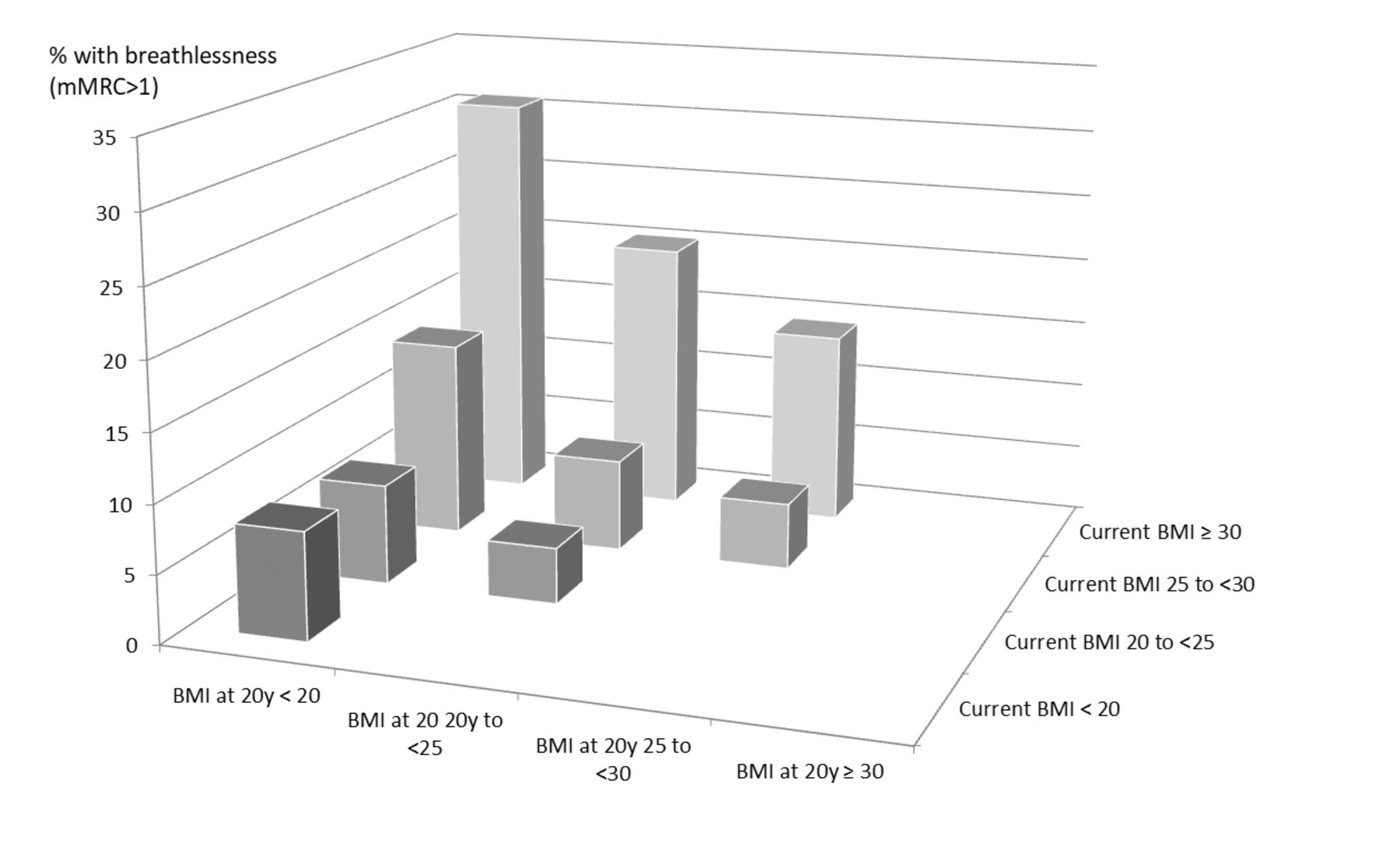
Prevalence of breathlessness stratified by current BMI and BMI at age 20. Breathlessness is defined as a mMRC breathlessness score ≥1. Groups with at least 100 people are shown. BMI, body mass index; mMRC, modified Medical Research Council.
Compared with men, women had a markedly steeper increase in breathlessness prevalence with higher BMI (p<0.0001 for interaction; figure 2). The difference was independent of confounders and adjustment for lung function impairment (FVC % of predicted). Associations between BMI and breathlessness are shown for men and women separately in Table S4 in the online supplement. There was evidence of effect modification between BMI and absolute FVC (p<0.0001 for interaction), with a steeper increase in breathlessness prevalence with higher current BMI in people with smaller spirometric lung volumes compared with in people with large lung volumes (figure 3). When comparing individuals with the same absolute FVC, the probability of breathlessness among obese was similar in men and women (figure 2). Findings were similar when not adjusting for level of physical exercise or FEV1/FVC in the models.

BMI and predicted probability of breathlessness (mMRC ≥1) in middle-aged men (n=6385) and women (n=7052). The models are adjusted for age, current smoking, asthma, hypertension, heart failure, anxiety, depression, level of physical exercise, airflow limitation (FEV1/FVC z-score); with (A) additional adjustment for lung function impairment (FVC z-score). In this model, the association between higher BMI and breathlessness was steeper in women (p<0.0001); (B) after adjustment for absolute spirometric lung volume (absolute FVC instead of z-score), the shape of the association between BMI and breathlessness differed between the sexes (p=0.027), but the probability of breathlessness in obese men and women was similar. BMI, body mass index; FEV, forced expired volume in one second; FVC, forced vital capacity; mMRC, modified Medical Research Council.

{kind=link}
{kind=link}
{kind=link}
The predicted probability of breathlessness (mMRC ≥1) by current BMI and quartiles of absolute FVC. Lower quartiles correspond to lower absolute FVC. The model is adjusted for age, sex, current smoking, level of airflow limitation (FEV1/FVC z-score), asthma, hypertension, heart failure, anxiety, depression and level of physical exercise. In obesity, the increase in breathlessness was higher in people with smaller absolute FVC (p for interaction <0.0001). BMI, body mass index; FEV, forced expired volume in one second; FVC, forced vital capacity; mMRC, modified Medical Research Council.
Discussion
The main findings were that in a middle-aged population, the prevalence of activity-related breathlessness was higher in relation to a range of obesity indicators; current BMI, change in BMI since age 20 and the presence of central obesity based on waist circumference. The accuracy of the associations was similar across the different obesity indicators. Irrespective of current BMI, individuals who had increased in BMI since age 20 had markedly more breathlessness. The associations between obesity and breathlessness remained strong after accounting for potential confounders including comorbidities and spirometric lung volumes (FVC). However, there was an interaction between BMI and FVC; the probability of breathlessness increased more steeply with higher BMI in people with lower absolute FVC. The higher breathlessness prevalence in obese women (compared with obese men) was related to their lower absolute FVC.
This is, to the authors’ knowledge, the first large population-based study evaluating the association between obesity and breathlessness employing physiological data including lung function. A novel finding is that, irrespective of current BMI, individuals who increased in BMI since age 20 reported markedly more breathlessness, which was independent of the confounders. Similar findings have been reported for weight gain and increase in sleep problems.12 While the present analysis was adjusted for available data on level of physical exercise, the association with gain in BMI, independent of current BMI, could reflect increased breathlessness related to life style changes, including decreased physical activity with deconditioning.
Central obesity, both defined using the WHO cut-off or waist circumference as a continuous variable, had similar predictive accuracy for breathlessness, and the association was of similar magnitude and accuracy as for categories of BMI. Unfortunately, data on waist circumference at age 20 were not available, wherefore changes in central obesity over time could not be analysed. Another limitation is that using BMI to define obesity does not account for the distribution of lean and fat mass. Men and women with a rapid gain in BMI at late childhood (in contrast to early childhood) are reported to have a higher fat mass index also when elderly.31 A gain in fat mass might affect breathlessness differently than a similar gain in lean mass. Hence, the association between previous changes in BMI and breathlessness could be related to an increase in fat mass in relation to lean mass, a hypothesis that remains to be evaluated in future research.
The higher prevalence of breathlessness in overweight and obese individuals does not seem to be explained by a higher prevalence of comorbidities in this population. A novel finding is that only a small part of the association between BMI and breathlessness seemed to be mediated through a decrease in FVC. This finding is in line with the previous suggestions that obesity increases breathlessness largely through the extra work load (directly related to the extra weight) and increased respiratory demand during activities of daily life.32–35 Furthermore, laboratory studies suggest that obesity is associated with increased ventilatory drive and exertional breathlessness related to enhanced work load and increased energy cost of breathing due to the weight.15 32–37 The present study extends these findings to breathlessness experienced during daily life in the middle-aged general population.
Interestingly, higher BMI was associated with an exponential increase in breathlessness prevalence, with a markedly steeper increase among people with smaller spirometric lung volumes. In line with this, there was a steeper rise in breathlessness with increasing BMI in women, which was at least partly related to by their lower absolute FVC. This indicates that individuals with smaller lung volumes are more vulnerable to develop breathlessness in relation to factors that increase the demand/capacity ratio of the respiratory system, such as obesity. When accounting for the absolute FVC, the change in breathlessness in relation to BMI became more similar for men and women.
Strengths of the present study include the large, population-based sample with data on relevant confounders and standardised physiologic measurements, including BMI, waist circumference and spirometry. The findings pertain to individuals in the general population, aged 50–64 years. Due to the cross-sectional design, estimates should be interpreted as associations and causality cannot be inferred. BMI at age 20 was calculated using self-recalled weight and current height (as height at age 20 was unavailable), and could therefore be affected by recall bias and did not account for changes in height between age 20 and the assessment at (age: 50–64 years). However, people have been reported to be able to accurately recall body weight after 28 years.38 Data on weight for specific years since age 20 were not available, and the impact of weight fluctuations should be evaluated in further research. The presence of comorbidities was mostly based on self-report and large-scale studies of physiological measurements including of heart function are needed. Measurements of static lung volumes (including the functional residual capacity) or during standardised exercise test were unavailable, and are relatively unfeasible in large population studies. Findings in relation to BMI and breathlessness were consistent with a previous analysis using static lung volumes.6
For the clinician, the present findings put forward the importance of evaluating breathlessness in obesity. Obesity is a preventable and treatable condition and obesity-related breathlessness can be relieved by exercise training39 and weight reduction,34 including bariatric surgery40 41 in selected patients with severe obesity. Individuals with smaller lung volumes constitute a risk group for developing breathlessness in relation to obesity or other factors that increase the demand or decrease the capacity ratio of the respiratory system.
References
Footnotes
MPE and AB are first authors.
Contributors Members of SCAPIS National Steering committee and therefore responsible for funding and the planning and execution of the SCAPIS study: AB, GB, JB, GE, JEE, TJ, AR, MS, JS, SS, KT, CJÖ and EL. Responsible for the conception and design of the analyses included in the specific manuscript and first draft: ME, AB and EL. Data collection: JB, JEE, KG, TH, LTN, HLP, MS, ES and HT. Statistical analysis: ME; All authors were involved in the planning and data interpretation and revision of manuscript drafts for important intellectual content, and approval of the version to be published.
Funding The main funding body of The Swedish CArdioPulmonary bioImage Study (SCAPIS) is the Swedish Heart and Lung Foundation. The study is also funded by the Knut and Alice Wallenberg Foundation, the Swedish Research Council and VINNOVA (Sweden’s Innovation agency) the University of Gothenburg and Sahlgrenska University Hospital, Karolinska Institutet and Karolinska University Hospital, Linköping University and University Hospital, Lund University and Skåne University Hospital, Umeå University and University Hospital, Uppsala University and University Hospital. Individual research support: AR from AFA Insurance [160334]; from the Swedish state under the agreement between Swedish government and the county councils, the ALF-agreement [ALG-GBG-74300 to K.T., G.B., J.B. A.C.O., A.R.], [ALF-VLL-548791 for S.S.] and [ALFLIO-700841 for J.E.E.]. ME was supported by unrestricted grants from The Swedish Society of Medicine, the Swedish Heart-Lung Foundation, and the Swedish Society for Medical Research.
Competing interests SS reports being an advisory board member and receiving speakers honoraria from Actelion, Bayer, MSD, outside the submitted work. Dr Olin reports having a patent WO2009045163 (Collection and measurement of exhaled particles) and being a chairholder and board member of PExA AB, outside the submitted work. JS reports advisory board work for Itrim, outside the submitted work.
Patient consent for publication Not required.
Ethics approval The study was approved by the Regional Ethical Review Board at Umeå University (Nr: 2010- 228–31 M).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Linked Articles
- Airwaves