Article Text

Statistics from Altmetric.com
A 21- year-old Indian man presented with a history of shortness of breath and cough with expectoration for 2 years. The expectoration was copious in amount and was associated with occasional streaky haemoptysis. For 2 years, he had recurrent wheezing with good symptomatic improvement with bronchodilators. Spirometry performed 2 years previously demonstrated moderate obstructive ventilatory defect without bronchodilator reversibility. He had received multiple courses of oral steroids in the past year for treatment of exacerbations. He required hospitalisation thrice in the past year for infective exacerbations, requiring broad-spectrum antibiotics. His perinatal history was unremarkable and he had a history of pneumonia at 3 months of age. There was no history of recurrent infections in early childhood.
The presenting episode commenced with a 2 weeks history of right-side chest pain, fever and increased shortness of breath. On examination, he had clubbing, tachycardia, tachypnea and room air pulse oxygen saturation was 90%. Respiratory system examination revealed bilateral coarse crepitations. A posteroanterior chest radiograph was performed which demonstrated right loculated pleural effusion (figure 1A). Ultrasound guided pleural fluid aspiration was done which showed exudative, neutrophilic fluid with low pH and low glucose. Intercostal tube insertion was performed for drainage of the empyema thoracis. He was started on broad-spectrum antibiotics for 2 weeks and had marked clinical improvement. A CT scan of the thorax was performed, which demonstrated bilateral cystic bronchiectasis (figure 1B,C). Sweat chloride levels were normal.

(A) Chest radiograph demonstrating right loculated pleural effusion with bilateral lower zone opacities. (B) CT thorax demonstrating few air specks suggestive of diverticula in the posterior tracheal wall. (C) Bilateral lower lobe bronchiectasis with right-side hydropneumothorax with intercostal tube in situ.
Question
What is the likely cause of this patient’s bilateral bronchiectasis?
Answer
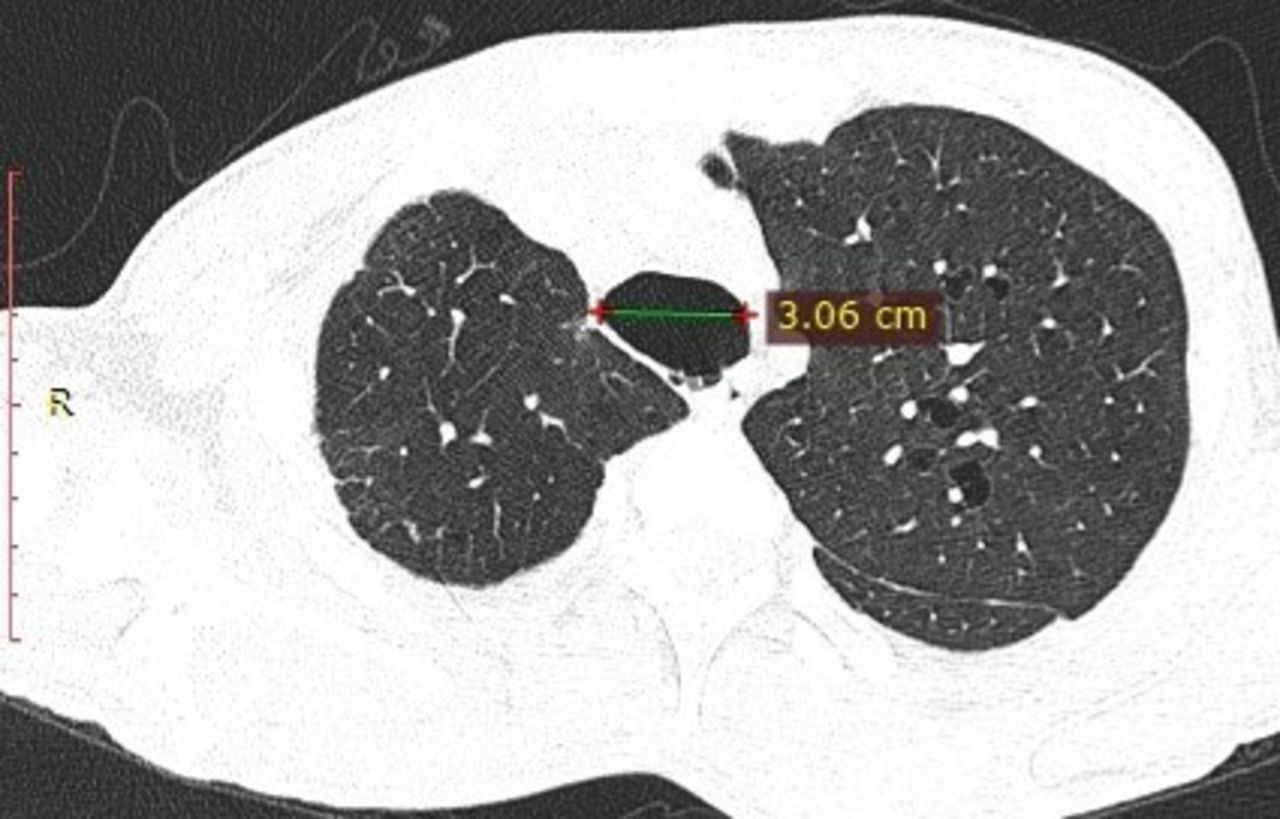
This patient with bilateral bronchiectasis has tracheobronchomegaly, which is appreciable on chest radiograph as well as on CT scan. The transverse diameter of his trachea is more than 30 mm, suggesting a diagnosis of congenital tracheobronchomegaly or Mounier-Kuhn syndrome (MKS) (figure 2). There is formation of multiple tracheal diverticuli in the posterior wall. MKS is an uncommon cause of bronchiectasis, caused by thinning of the muscularis mucosa, as well as thinning of longitudinal muscles and elastic fibres.1 2 This effectively increases the dead space and causes ineffective coughing and impairment of mucociliary clearance, leading to pooling of secretions, bronchiectasis and recurrent lower respiratory tract infections. The disease is sporadic and is reported more commonly in men. No population-based studies are available for the prevalence of MKS, though prevalence of 0.15% was estimated in a study involving 5234 patients who underwent CT thorax for respiratory symptoms.3 Tracheobronchomegaly has been reported in association with Ehlers-Danlos syndrome, Marfan’s syndrome, cutis laxa and ankylosing spondylitis, and these should be excluded before reaching a diagnosis of MKS. Our patient had no clinical features to suggest any of these associated conditions. The hallmark of MKS is central airway dilation, which is commonly overlooked in conventional chest radiographs. CT scan remains the gold standard for the diagnosis. The diagnosis is made by increased transverse and sagittal diameters of the trachea measuring 2 cm above the aortic arch. The diagnostic criteria in adults include diameter measurements as follows: trachea, >30 mm; right main bronchus, >20 mm; and left main bronchus, >18 mm. Saccular diverticula may be seen in the posterior wall of the trachea.2 Treatment options include mucolytics, physiotherapy, postural drainage and vaccination. Airway stenting and tracheobronchoplasty have also been tried with some improvement in symptoms and quality of life.4

{kind=link}
{kind=link}
CT thorax demonstrating trachea with a transverse diameter of more than 3 cm.
Footnotes
Contributors SPB and SM drafted the manuscript. KM and AM helped in patient management, as well as in the revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.