Article Text

Statistics from Altmetric.com
A 60-year-old male farmer with headache without fever for 2 months and with no other systemic disease presented to the emergency department with a 2-week history of non-productive cough as well as progressive hearing and vision loss. Chest radiography and CT scan revealed a left solitary tumour with pleural attachment (figure 1) without associated lymphadenopathy. At 3 days after admission, he lost consciousness and was administered emergency endotracheal intubation. On physical examination, a crusted nodule was observed proximal to the lateral end of the left eyebrow (figure 2). CT scan of the head revealed multiple foci of ischaemic change. An India ink stain of the cerebrospinal fluid (CSF) showed multiple encapsulated round yeasts. Biopsies of the nodule (figure 3) and the pulmonary tumour confirmed cryptococcoma. Additional laboratory tests revealed an elevated serum cryptococcal antigen titre (1:32) and normal blood CD4 +T cell count (471/m3). Moreover, viral examinations (for the serum HIV antibody and other viruses) as well as autoimmune panels were all negative. Furthermore, Cryptococcus gattii grew in all fungus cultures of the nodule, lung tumour and CSF. Fluconazole was administered as the main therapy for 3 weeks.

Axial chest CT showing left solitary tumour with pleural attachment.

A crusted nodule proximal to the tail of left eyebrow.

{kind=link}
{kind=link}
{kind=link}
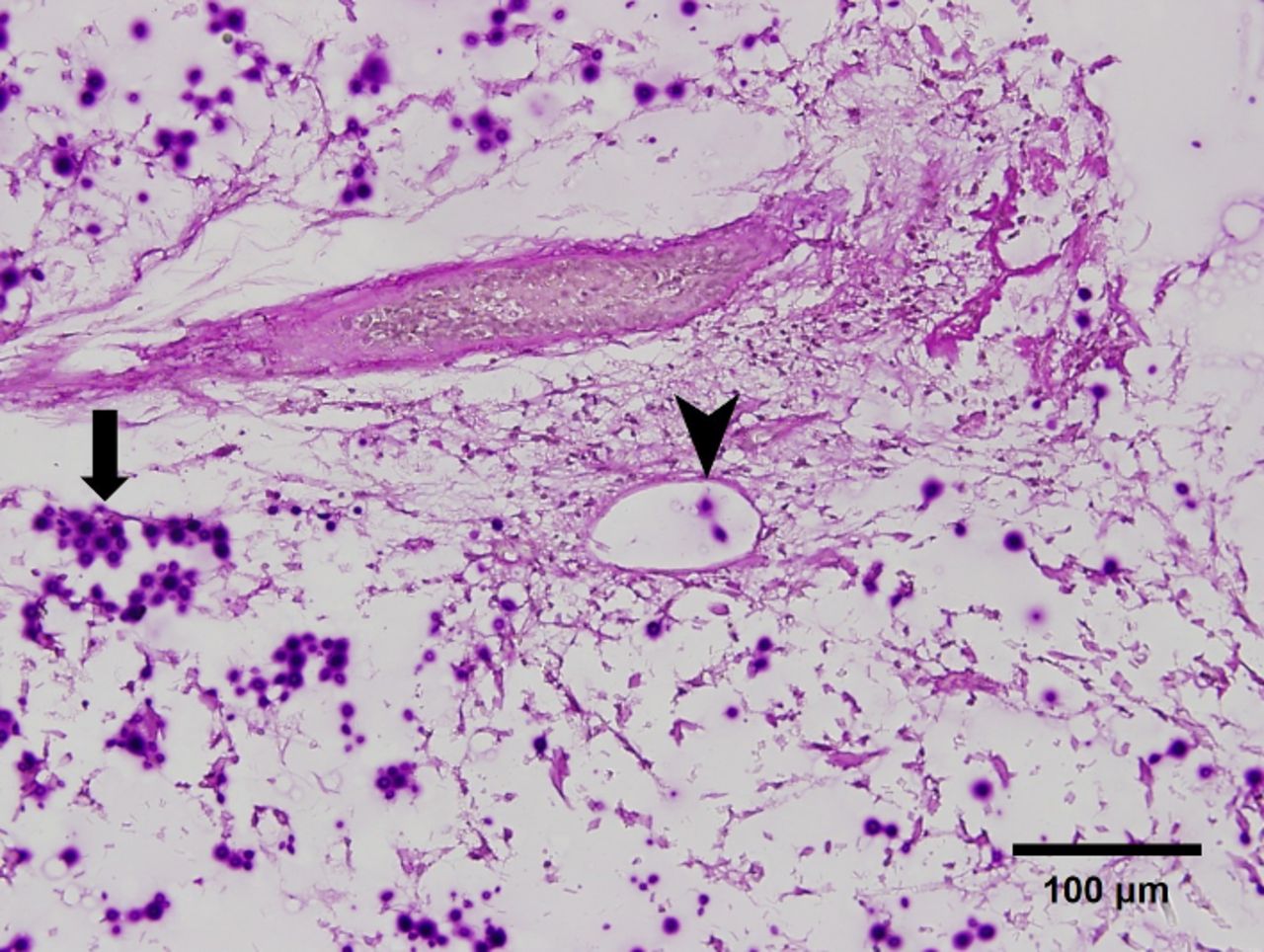
Periodic acid–Schiff stain (original magnification ×200) showing multiple encapsulated round yeasts (arrow) with lymphatic invasion (arrowhead).
Discussion
C. gattii is more prevalent than C. neoformans in immunocompetent hosts.1 The infection might manifest as cryptococcoma mimicking lung cancer.2 Moreover, it could be misdiagnosed as stroke because of severe neurological deficits, such as hearing loss or blindness.3 This infection rarely presents with cutaneous cryptococcal nodules, as observed in the present case, and merits extensive evaluation of disseminated cryptococcal infection involving, in particular, the lung and brain.
Footnotes
Contributors D-JL and C-KP managed the patient. H-HL and D-WH performed the surgery. C-HL prepared the image and D-JL prepared the manuscript. C-KP revised this article.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.