Article Text

Abstract
Purpose Lung cancer risk models optimise screening by identifying subjects at highest risk, but none of them consider emphysema, a risk factor identifiable on baseline screen. Subjects with a negative baseline low-dose CT (LDCT) screen are at lower risk for subsequent diagnosis and may benefit from risk stratification prior to additional screening, thus we investigated the role of radiographic emphysema as an additional predictor of lung cancer diagnosis in participants with negative baseline LDCT screens of the National Lung Screening Trial.
Methods Our cohorts consist of participants with a negative baseline (T0) LDCT screen (n=16 624) and participants who subsequently had a negative 1-year follow-up (T1) screen (n=14 530). Lung cancer risk scores were calculated using the Bach, PLCOm2012 and Liverpool Lung Project models. Risk of incident lung cancer diagnosis at the end of the study and number screened per incident lung cancer were compared between participants with and without radiographic emphysema.
Results Radiographic emphysema was independently associated with nearly double the hazard of lung cancer diagnosis at both the second (T1) and third (T2) annual LDCT in all three risk models (HR range 1.9–2.0, p<0.001 for all comparisons). The number screened per incident lung cancer was considerably lower in participants with radiographic emphysema (62 vs 28 at T1 and 91 vs 40 at T2).
Conclusion Radiographic emphysema is an independent predictor of lung cancer diagnosis and may help guide decisions surrounding further screening for eligible patients.
- lung cancer
- screening
- risk assessment
- national lung screening trial
- emphysema
Statistics from Altmetric.com
Key messages
What is the key question?
Can the presence of radiographic emphysema on baseline lung cancer screen be used to guide further screening in patients with a negative initial low-dose CT (LDCT) screen?
What is the bottom line?
In a retrospective analysis of the National Lung Screen Trial data, emphysema identified on baseline LDCT is an independent predictor of lung cancer diagnosis in subjects with a negative baseline LDCT screen after controlling for risk factors included in several validated risk prediction models.
Why read on?
Risk stratification of patients eligible for additional rounds of lung cancer screening may be augmented by the addition of radiographic emphysema diagnosis.
Introduction
The National Lung Screening Trial (NLST) demonstrated a 20% relative decrease in lung cancer-related mortality among high-risk smokers who underwent low-dose CT (LDCT) screening.1 Based on the NLST enrolment criteria, the United States Preventive Services Task Force (USPSTF) recommends annual LDCT screening for current smokers between the ages of 55 and 80 years with at least 30 pack-years of tobacco use, or former smokers with similar exposure who quit in the last 15 years, without specific consideration for other known lung cancer risk factors.2
The life-extending benefits of annual lung cancer screening must be weighed against potential harms including false positive tests, complications from invasive workup of LDCT findings, radiation exposure and increased healthcare costs. Selection of candidates for screening may be optimised by the use of lung cancer risk prediction models, which allow the identification of people who would benefit most from annual LDCT.3 Incorporating these models into the decision-making process may maximise the benefits by further personalising screening eligibility and decreasing the number of persons needed to screen per case of lung cancer detected.
Current lung cancer diagnosis prediction models use sociodemographic characteristics, smoking history, personal cancer history and the presence of other exposures to estimate lung cancer risk and can be applied at the time of baseline screening.4–7 However, reassessing an individual’s risk for lung cancer at the time of repeat annual screening may be particularly important for people with a negative baseline LDCT, a group at decreased risk of lung cancer.8 Information gained from the baseline screen may provide new valuable information for guiding future screening. We hypothesised that radiographic emphysema, an independent risk factor identifiable on baseline LDCT, might allow for further lung cancer risk stratification among patients who fulfil screening criteria.8–10 Therefore, we determined whether radiographic emphysema independently added information to established risk prediction models in individuals with negative screening tests and quantified the impact on the number screened per incident lung cancer.
Methods
Study population
We used data from the NLST, a randomised, multicentre trial that compared LDCT versus chest radiograph for early detection of lung cancer. Participants were randomly assigned to receive either three annual LDCT screens or single-view posterior-anterior chest radiographs and followed up for an average of 6.4 years.1 We identified two analytic cohorts consisting of 1) participants with complete data for calculating lung cancer risk randomised to the LDCT arm who had a negative baseline (T0) screen (n=16 624; the ‘T0-negative’ cohort) and 2) participants who subsequently also had a negative 1-year follow-up (T1) screen (n=14 530; the ‘T0/T1-negative’ cohort). Participants with prevalent cancers or baseline screens positive for nodule(s) >4 mm, enlarging nodule(s), mass(es) or other non-specific abnormalities suspicious for lung cancer were not included in our negative cohorts as they would require additional screening LDCTs regardless of the presence or absence of emphysema.
Our primary outcome was incident lung cancer diagnosis until follow-up after T0 or T1 screen for participants in the T0-negative and T0/T1-negative cohorts, respectively. Lung cancer diagnoses in the NLST were established through the review of standardised data forms administered to all participants. Cases were confirmed using patient medical records, including pathology reports. We also collected the date of death for subjects who died during follow-up for use in cumulative incidence analyses to account for competing risks.
From NLST baseline survey data, we obtained information on participants’ age, gender, race, ethnicity, body mass index (BMI), education, smoking history, personal and family history of cancer, pneumonia, asbestos exposure and self-reported COPD, emphysema and chronic bronchitis. This information was determined from entrance questionnaires given to all participants. All LDCT scans were interpreted by trained radiologists that were certified by the American Board of Radiology or equivalent, had training in diagnostic radiology and were involved in the supervision and interpretation of at least 300 chest CT acquisitions in the past 3 years. Scans were reviewed for nodules, masses or other abnormalities suspicious for lung cancer, as well as other findings of clinical significance such as emphysema.11 Our primary exposure of interest was emphysema determined during the interpretation of baseline screens. There were no specific diagnostic criteria regarding the determination of emphysema in NLST study protocols.12
We classified participants' predicted risk of being diagnosed with lung cancer based on three validated lung cancer prediction models: the Bach model, the PLCOm2012 model and the Liverpool Lung Project (LLP) model (table 1).5–7 All models include age and smoking duration as risk factors for lung cancer. The Bach and PLCOm2012 models incorporate other smoking-related factors such as smoking intensity, the Bach and LLP models include asbestos exposure and PLCOm2012 and LLP also consider a participant’s personal and family history of cancer. The PLCOm2012 model considers self-reported COPD, which was coded to include self-reported COPD, self-reported emphysema and self-reported chronic bronchitis.
Details of lung cancer risk prediction models
Statistical analyses
We calculated the lung cancer risk scores of each participant using the three prediction models described above and stratified them into risk quartiles with quartile 1 representing the lowest and quartile 4 representing the highest predicted lung cancer risk. We fitted Cox proportional hazard model to assess whether radiographic emphysema was an independent predictor of lung cancer after controlling for risk scores and risk quartiles based on the three models. Within each risk quartile, we computed the number screened per incident lung cancer (both screen and non-screen detected cancers), based on actual NLST results, in participants with or without radiographic emphysema. We calculated the time-varying area under the receiver operating curve, or c-statistic, for each model to assess discrimination using the entire follow-up period.13
Subjects with greater smoking exposure (associated with emphysema) were at a higher risk of death from non-lung cancer causes, which served as a competing risk potentially affecting our estimates of lung cancer incidence. To determine the risk of lung cancer in each risk quartile and by radiographic emphysema status while accounting for competing risks, we plotted cumulative incidence curves using competing risk survival methods and evaluated differences in cumulative incidence using Gray’s test.14
All analyses were conducted using SAS V.9.4 and R V.3.4.1.
Results
Study participants
A total of 53 454 participants were enrolled in NLST and 26 722 were randomised to screening with LDCT. We first excluded participants with a baseline LDCT screen positive for nodule(s) >4 mm, enlarging nodule(s), mass(es) or other non-specific abnormalities suspicious for lung cancer as determined by the interpreting radiologist (n=7191) as these participants would have received additional workup regardless of emphysema status. Participants who were non-adherent to the NLST protocol, those with inadequate or low-quality baseline LDCT and participants with duplicate entries were also excluded (n=417), leaving 19 114 participants in our analytic cohort. We then excluded participants with incomplete covariate data (n=2490), leaving final T0-negative and T0/T1-negative cohorts consisting of 16 624 and 14 530 NLST participants, respectively. Among the T0-negative cohort, 5486 (33.0%) participants were determined to have emphysema on baseline scan. Participants with baseline scans positive for emphysema were clinically similar in baseline characteristics to participants with baseline scans negative for emphysema (table 2).
Baseline characteristics of study subjects based on T0 screen results for emphysema
Among the T0-negative and T0/T1-negative cohorts, 367 (2.21%) and 220 (1.15%) cases of lung cancer were diagnosed in the 6.4-year follow-up period, respectively. Most prediction models showed a statistically significant higher incidence of lung cancer with increasing risk quartile in both cohorts. There were non-significant relative increases in hazard of lung cancer diagnosis of participants in risk quartile 2 compared with risk quartile 1 in the PLCOm2012 and LLP models (table 3). Prevalence of radiographic emphysema increased with increased risk quartile in all models with the exception of risk quartile 1 and 2 in the T0-negative cohort stratified by the LLP model, and risk quartile 3 and 4 in the T0/T1-negative cohort stratified by the LLP model (table 3).
Hazard of lung cancer in participants with emphysema adjusting for risk quartile based on established risk models
Regardless of the prediction model, participants with radiographic emphysema had nearly double the hazard of diagnosis with lung cancer when compared with participants without radiographic emphysema after adjustment for risk quartile in both the T0-negative and T0/T1-negative cohorts. When using the Bach model, participants with radiographic emphysema had 1.88 (95% CI 1.53 to 2.31) and 1.93 (95% CI 1.48 to 2.52) times the hazard of lung cancer compared with participants without radiographic emphysema for the T0-negative and T0/T1-negative cohorts, respectively. In the PLCOm2012 model, participants with radiographic emphysema had 1.80 (95% CI 1.46 to 2.22) and 1.80 (95% CI 1.38 to 2.36) times the hazard of lung cancer compared with participants without radiographic emphysema for the T0-negative and T0/T1-negative cohorts, respectively. Based on the LLP model, participants with radiographic emphysema had 1.97 (95% CI 1.60 to 2.42) and 2.02 (95% CI 1.55 to 2.64) times the hazard of lung cancer compared with participants without radiographic emphysema for the T0-negative and T0/T1-negative cohorts, respectively (table 3, all p<0.001). The addition of radiographic emphysema improved the discrimination of the models for the prediction of incident lung cancer, although the difference in c-statistic values was not statistically significant (online supplementary appendix 1).
Supplemental material
In models that controlled for continuous risk score as opposed to risk quartile, similar HRs were obtained. In the Bach model, participants with emphysema had 1.82 (95% CI 1.48 to 2.25) and 1.87 (95% CI 1.43 to 2.45) times the hazard of lung cancer compared with participants without radiographic emphysema for the T0-negative and T0/T1-negative cohorts, respectively. In the PLCO2012 model, participants with emphysema had 1.75 (95% CI 1.42 to 2.16) and 1.78 (95% CI 1.36 to 2.34) times the hazard of lung cancer compared with participants without radiographic emphysema for the T0-negative and T0/T1-negative cohorts, respectively. In the LLP model, participants with emphysema had 1.95 (95% CI 1.58 to 2.40) and 2.01 (95% CI 1.54 to 2.63) times the hazard of lung cancer compared with participants without radiographic emphysema for the T0-negative and T0/T1-negative cohorts, respectively.
The number screened per incident lung cancer was lower in participants with or without radiographic emphysema across almost all risk quartiles for the three risk prediction models (table 4). In the T0-negative cohort, the number screened per incident lung cancer was 28 vs 62 for participants with or without radiographic emphysema. The number screened per incident lung cancer was higher in the T0/T1-negative cohort, 40 vs 91 for participants with or without radiographic emphysema. The number screened per incident lung cancer decreased, in general, with increasing risk quintiles for all prediction models. This decrease was especially pronounced between the lower two risk quartiles and the higher two risk quartiles.
Number screened per incident lung cancer according to the presence or absence of emphysema
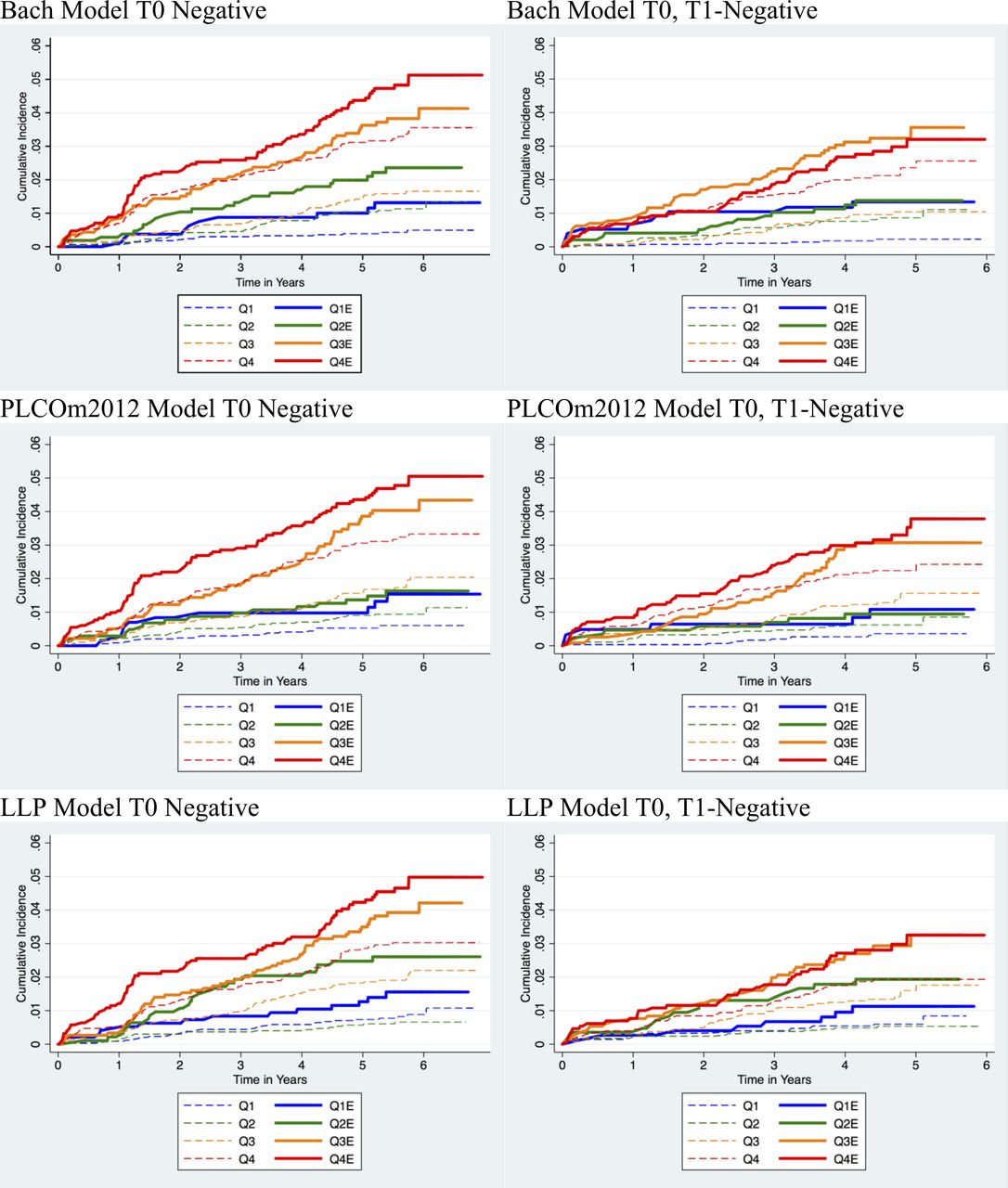
In analyses accounting for the competing effects of all-cause mortality (which may have been higher in subjects with radiographic emphysema), the overall cumulative incidence of lung cancer diagnosis in participants with radiographic emphysema was higher than in participants without radiographic emphysema across risk quartiles (all p<0.0001; figure 1). There was an increased overall cumulative lung cancer incidence with increased risk quartile. Additionally, the cumulative lung cancer incidence was generally lower in participants with both a negative T0 and T1 screen compared with those with a negative T0 screen. The 5-year cumulative incidences of lung cancer based on risk quartile and emphysema status are shown in table 5. The 5-year cumulative incidences of lung cancer generally increased with increasing risk quartile. The 5-year cumulative incidences were higher in participants with emphysema compared with those without emphysema across the same risk quartile, but these differences did not always meet statistical significance.

{kind=link}
Cumulative incidence of lung cancer plots stratified by risk quartile and emphysema. Differing risk quartile cohorts are represented by different colours with quartile 1 (blue) as lowest risk and quartile 4 (red) as highest risk. Bold lines indicate cohorts with emphysema and dashed lines indicate cohorts without emphysema. Q1: risk quartile 1 without emphysema, Q1E: risk quartile 1 with emphysema, Q2: risk quartile 2 without emphysema, Q2E: risk quartile 2 with emphysema, Q3: risk quartile 3 without emphysema, Q3E: risk quartile 3 with emphysema, Q4: risk quartile 4 without emphysema, Q4E: risk quartile 4 with emphysema. All p<0.0001 according to Gray’s test for equality of cumulative incidence functions. LLP, Liverpool Lung Project.
5-Year cumulative incidence percentages (CIP) of lung cancer diagnosis in participants stratified by risk quartile and radiologic emphysema status
Discussion
In this study, we found that radiographic emphysema was an independent predictor of lung cancer risk in NLST participants with negative T0 and T1 screens, even after accounting for validated lung cancer risk scores. Moreover, presence or absence of radiographic emphysema substantially influenced the number screened per incident lung cancer across all risk groups. These findings suggest that adding radiographic emphysema to existing prediction models can increase their discrimination and could help identify individuals more likely to benefit from additional rounds of lung cancer screening. Additionally, individuals with a baseline screen negative for both radiographic emphysema and lung cancer may benefit from a modified screening schedule.
Several well-validated risk prediction models are able to determine lung cancer risk based on patient’s demographics, smoking history, occupational exposure history, personal and family history of malignancies and self-reported history of COPD.4–7 15 Although not currently recommended by major guidelines, including the USPSTF, eligibility criteria based on these models can help optimise screening and may be more efficient than current selection criteria based only on age and smoking history.16 17 In NLST, for example, 88% of preventable lung cancer mortality occurred in participants in the top 60% of risk as determined by the PLCOm2012 model, compared with only 1% of among those in the bottom 20%.4 5 Additionally, a better cost-effectiveness ratio can be achieved by focusing screening on individuals at a higher lung cancer risk.18 19 Several experts have argued that current guidelines lack specificity and that eligibility criteria should be revised to improve the harm-to-benefit profile of lung cancer screening programmes.5 20 Individuals with a negative baseline (or annual repeat) screening test stand to particularly benefit from risk stratification prior to additional screening as they have a lower incidence of lung cancer and lung cancer-related mortality.4
The importance of radiographic emphysema as an independent risk factor for lung cancer has been well studied and confirmed in observational studies and a meta-analysis.4 21 22 Our study builds on these findings by examining radiographic emphysema as an additional lung cancer predictor used in concert with well-established risk stratification models for patients with negative baseline screens, as well as negative baseline and first annual screens. Our findings show that LDCT-detected emphysema, in combination with existing models, can be used to discriminate patients with the highest lung cancer risk that would benefit the most from additional screening. Conversely, low risk patients without radiographic emphysema may benefit from a repeat screening after 2–3 years (or longer) or possibly no further screening. Existing mathematical models of the natural history of lung cancer, as those developed by Cancer Intervention and Surveillance Modeling Network (CISNET), could be used to identify the optimal screening regimens of these individuals.23
Our study had several strengths and limitations. We used data from a large, geographically diverse study which should provide robust data lung cancer prevalence among candidates for lung cancer screening. Our analysis focused on emphysema confirmed on baseline LDCT by a trained radiologist instead of self-reported emphysema which may be inaccurate and subject to reporting bias.24 However, radiologists at different screening sites may have used differing criteria when determining the presence or absence of emphysema. We did not account for emphysema not detected on baseline LDCT but detected on subsequent screens, which may have occurred due to radiologist variability in evaluating and reporting emphysema. It is unlikely a participant with a baseline LDCT truly negative for emphysema would develop evidence of emphysema in their 1-year follow-up screen because emphysema is a chronic process. We focused on risk of lung cancer incidence instead of lung cancer mortality, the reduction of which is the ultimate goal of screening programmes. Although LDCT may lead to some ‘overdiagnosis’, incidental lung cancers detected on annual repeat screening, particularly after a negative baseline test, are more likely to be aggressive.25 Additionally, another secondary analysis of NLST observed that in participants with spirometric COPD, there was no excess in detected cancers between the screening arms with the cancers having comparable histology.26 Thus, our results likely did not overestimate the relationship between LDCT-detected emphysema and lung cancer risk. Our findings are also only applicable to patients with similar baseline characteristics as NLST participants and cannot be generalised to alternative screening and follow-up schedules. Notably, NLST participants were otherwise healthy and asymptomatic, thus those with emphysema associated with decreased functional status may not experience the same benefit from continued screening.
In 2011, there were 8.9 million NLST-eligible and 20.3 million NLST-ineligible smokers between the ages of 55 and 74 years of age and 94 million current and former smokers of all ages in the USA.27 A major unanswered question is which of these individuals would benefit most from lung cancer screening and what would be the optimal screening regimen, including number of years of screening. Online calculators developed for the Bach and PLCOm2012 models have provided opportunities for quick risk estimation in the clinical setting.28–30 The PLCOm2012 model has also been embedded in a widely adopted lung cancer screening decision aid that can be used to satisfy Medicare and Medicaid reimbursement requirement for shared decision making.31 The addition of a radiographic emphysema diagnosis may help to further clarify the benefits of lung cancer screening in the context of continued shared decision making between patients with negative baseline LDCT and their providers.
In summary, emphysema identified on a baseline lung cancer screen was an independent predictor of lung cancer in NLST participants who received continued annual LDCT screens, even after risk score stratification by validated prediction models. Risk stratification of patients eligible for additional rounds of lung cancer screening may be augmented by the addition of radiographic emphysema.
References
Footnotes
Contributors PY takes responsibility for the article as a whole; PY, KMS, JPW, JPde-T, and JJZ conceived the study; JPde-T, JJZ and KMS obtained research funding; PY, KMS and JPW supervised the conduct of the study; PY, GM and MK analysed the data; PY, JPW, CYK, DW, S-AWB and CS interpreted analysis findings; PY drafted the manuscript, and all authors contributed substantially to its revision.
Funding Supported by National Cancer Institute (K07 CA180782 to KMS, K07 CA187071 to MK) and grant PI16/01149 Instituto de Salud Carlos II, Government of Spain. KMS and MK were supported in part by a career award from the National Cancer Institute. This work was supported in part by grant PI16/01149 from the Instituto de Salud Carlos II, Government of Spain. CS was supported by resources from the VA Portland Health Care System, Portland, Oregon, USA.
Disclaimer The funding source had no role in the design, conduct or reporting of this study or in the decision to submit the manuscript for publication. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the US Government.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was exempt by the Institutional Review Board of the Icahn School of Medicine at Mount Sinai.
Provenance and peer review Not commissioned; externally peer reviewed.