Article Text

Statistics from Altmetric.com
Case presentation
A 40-year-old man presented with numbness of the lower limbs and pain in the lower back for 11 months. Abdominal CT revealed multiple retroperitoneal masses around the left renal hilus and abdominal aorta. Over the subsequent 4 months, the lesions progressed, resulting in hydronephrosis of the left kidney and bone destruction in the L2 vertebral body (figure 1). Three biopsies (two from the L2 vertebral body and one from the retroperitoneal mass) had been previously taken at another hospital. Pathological examination of all three biopsies had resulted in a diagnosis of IgG4-related disease (IgG4-RD) (figure 2). He had been taking a moderate dose of methylprednisolone (20 mg/day) for 4 months. Chest CT revealed a nodule in the apical segment of the right lung, 7 months after initial presentation. His symptoms did not improve on treatment with steroids. By 9 months after presentation, the patient had developed paralysis, hypoaesthesia, numbness and pain in both lower limbs. Intravenous methylprednisolone (250 mg/day) was administered for 7 days and reduced to 40 mg/day thereafter. He then underwent L1/2 laminectomy and decompression with no improvement in symptoms. The pathological diagnosis was again consistent with IgG4-RD. Ten months after presentation, the patient exhibited incomplete paralysis with level 0-I muscle strength, partial bilateral hypoaesthesia and amyotrophy of the lower limbs, absent tendon reflexes and a negative Babinski sign. He was admitted to our hospital 11 months after onset of symptoms.
Laboratory tests on admission to our institution revealed a high erythrocyte sedimentation rate (>140 mm/hour) and C reactive protein (92.15 mg/L). Serum IgG was 18.03 g/L and IgG42570 mg/L. Screening for tuberculosis, other bacterial and fungal infection by blood and sputum cultures was negative.
Because a chest CT revealed progressive nodule enlargement, we performed video-assisted thoracoscopic surgery to investigate the pathology of the lesion. Surprisingly, the pathological diagnosis was pulmonary inflammatory myofibroblastic tumour (IMT), anaplastic lymphoma kinase being positive by immunohistochemistry (figure 2). His symptoms began to resolve immediately after surgery. Six months later, lower muscle strength had improved to level V and the dosage of methylprednisolone had been reduced to 8 mg/day (figure 1E–H).
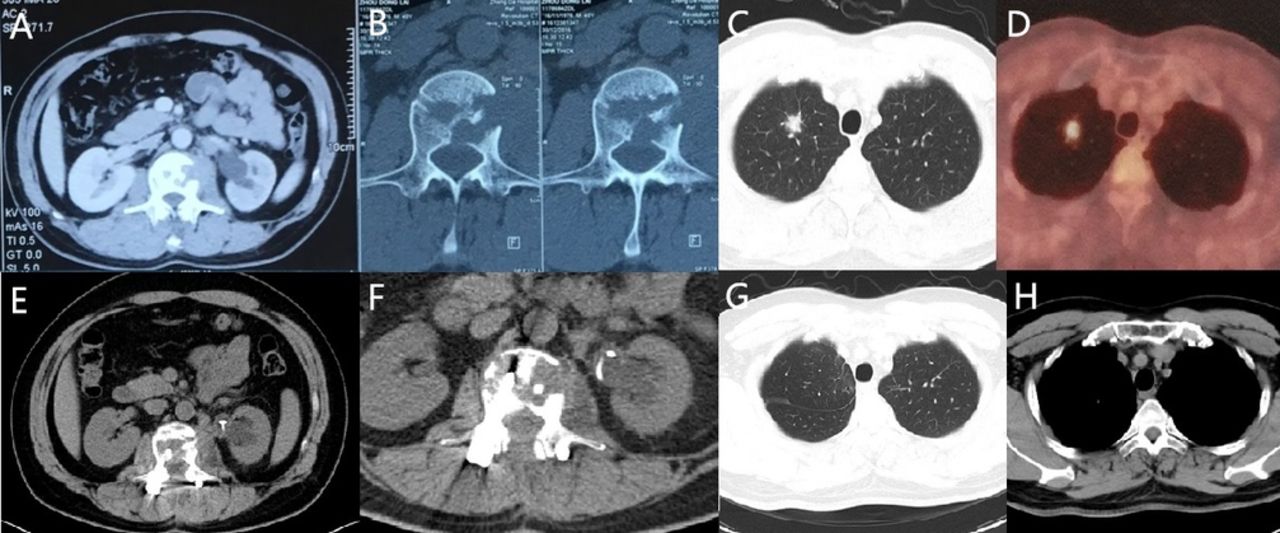
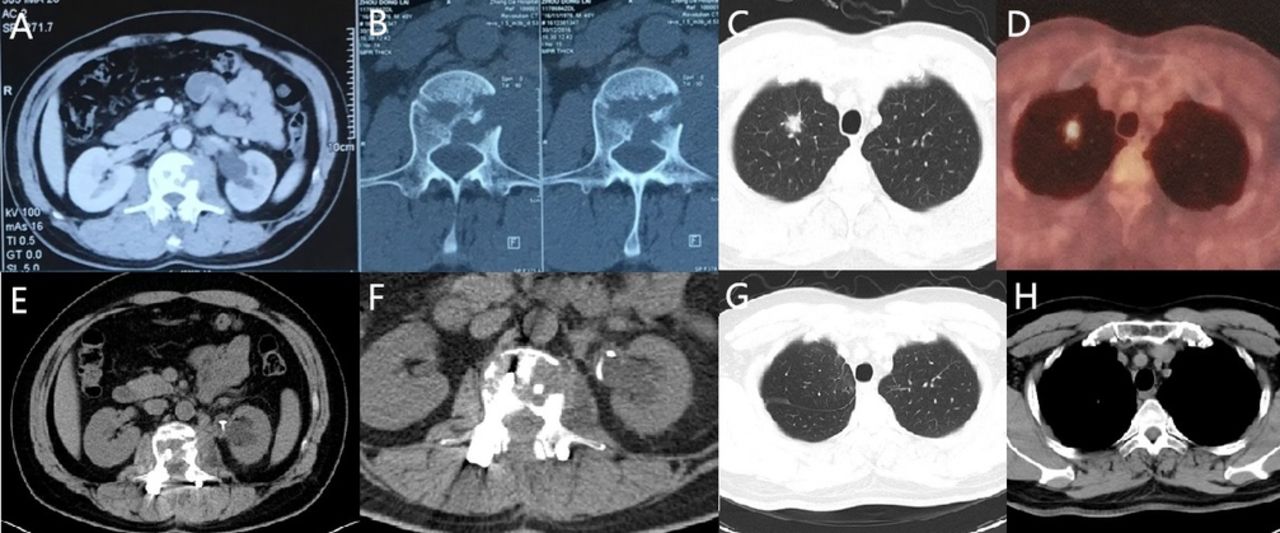
CT imaging and fluodeoxyglucose-positron emission tomography/CT scan retroperitoneal mass around the left renal hilus and aorta abdominalis (A), bone destruction in the L2 vertebral body (B) and enlarged nodule in the apical segment of the right lung (diameter, 1.4 cm) with a maximum standard uptake value of 8.34 by fluodeoxyglucose-positron emission tomography/CT scan (C, D) before surgery. And CT scan of retroperitoneal mass (E), bone destruction (F) and lung (G, H) after L1/2 laminectomy and decompression surgery and pneumonectomy. A, B, C, D are images before thoracoscopic surgery; E, F, G, H are images 6 months after thoracoscopic surgery.

{kind=link}
{kind=link}
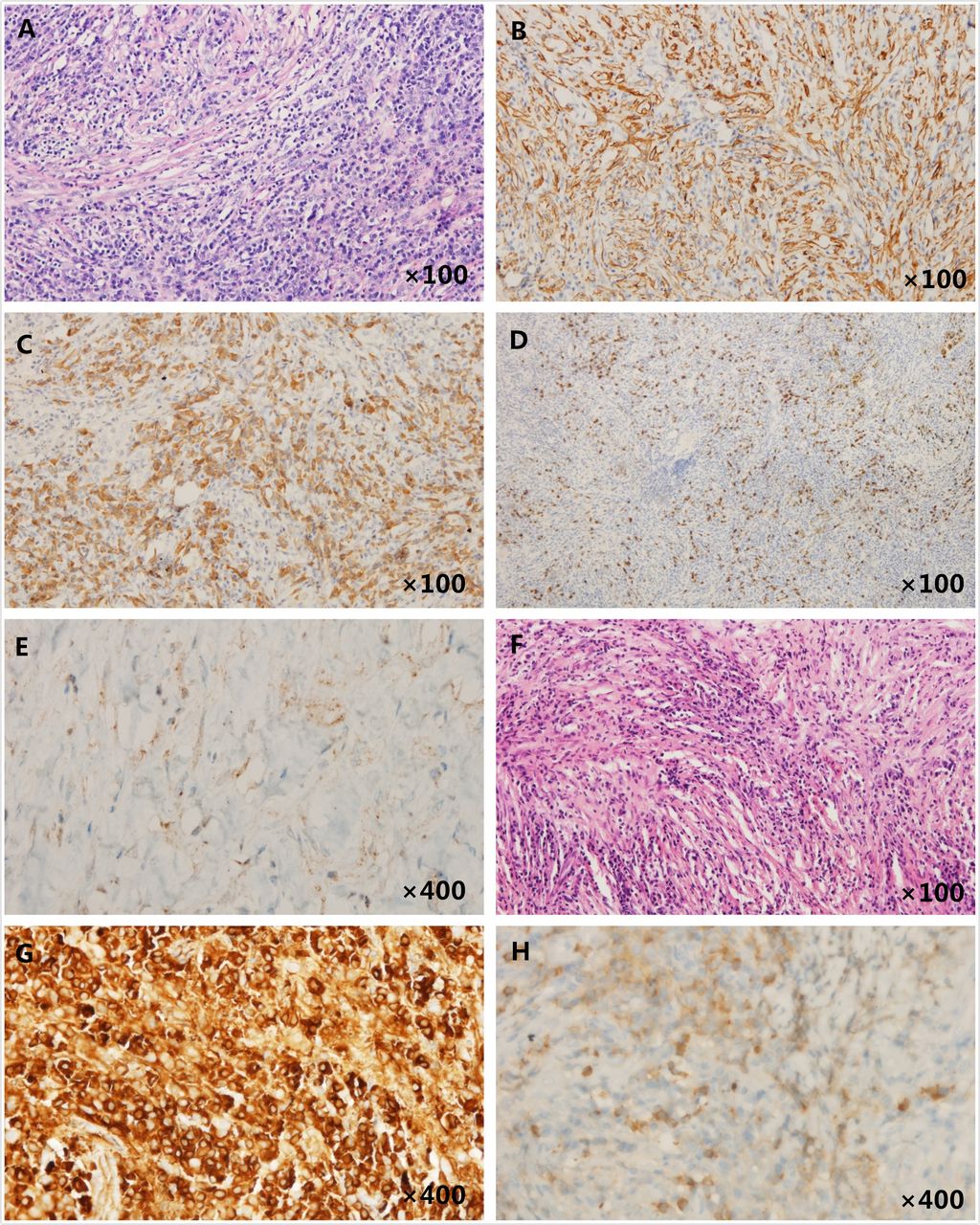
Lung lesion biopsy and L2 vertebral body lesion H&E and immunohistochemistry (IHC) staining lung lesion specimen with plasma and lymphocytes infiltrated in numerous myofibroblasts, H&E staining of lung lesion specimen (A). A positive IHC staining of the inflammation cells presented in the cytoplasm in lung lesion specimen for smooth muscle actin (SMA) (B), IgG (C), IgG4 (D) and anaplastic lymphoma kinase (ALK) (E) expression. L2 vertebral body lesion with H&E staining (F), positive IHC staining of IgG (G), with poor staining quality and IgG4 (H).
Discussion
IgG4-RD, an immune-mediated fibroinflammatory disease, is characterised by high serum IgG4 titres, massive IgG4-positive lymphocyte infiltration and fibrosis. Recent studies suggest that tumours can mimic IgG4-RD,1 which is consistent with the patient’s original misdiagnosis of primary IgG4-RD on the basis of the biopsies. Notably, removal of the patient’s pulmonary IMT resulted in dramatic symptomatic improvement. IMT is composed of differentiated myofibroblastic spindle cells with excessive inflammatory cell infiltration, differentiating it from IgG4-RD. Detection of anaplastic lymphoma kinase expression is helpful in the differential diagnosis of IMT and IgG4-related inflammatory pseudotumours.2 Some IMTs are functional tumours, associated with paraneoplastic syndromes.3 To the best of our knowledge, this is the first report of IgG4-RD associated with pulmonary IMT. More attention should be paid to identifying diseases that can mimic IgG4-RD, particularly when the presentation is atypical, because of the significant differences in response to treatment.
Acknowledgments
The authors would like to thank our colleagues who were involved in the care of this patient but were not eligible for listing as authors. They also thank Trish Reynolds, MBBS, FRACP, from Liwen Bianji, Edanz Group China, for editing the English text of a draft of this manuscript.
Footnotes
Patient consent for publication Obtained.
Contributors ShuZ and ShaZ conceived of the project. All authors contributed to discussion about, and treatment of, the patient and approved the final version of the manuscript. ShaZ is the corresponding author of this manuscript and takes full responsibility for its contents.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves