Article Text

Abstract
Background Pneumococcal conjugate vaccines (PCVs) have the potential to prevent pneumococcal disease through direct and indirect protection. This multicentre European study estimated the indirect effects of 5-year childhood PCV10 and/or PCV13 programmes on invasive pneumococcal disease (IPD) in older adults across 13 sites in 10 European countries, to support decision-making on pneumococcal vaccination policies.
Methods For each site we calculated IPD incidence rate ratios (IRR) in people aged ≥65 years by serotype for each PCV10/13 year (2011–2015) compared with 2009 (pre-PCV10/13). We calculated pooled IRR and 95% CI using random-effects meta-analysis and PCV10/13 effect as (1 − IRR)*100.
Results After five PCV10/13 years, the incidence of IPD caused by all types, PCV7 and additional PCV13 serotypes declined 9% (95% CI −4% to 19%), 77% (95% CI 67% to 84%) and 38% (95% CI 19% to 53%), respectively, while the incidence of non-PCV13 serotypes increased 63% (95% CI 39% to 91%). The incidence of serotypes included in PCV13 and not in PCV10 decreased 37% (95% CI 22% to 50%) in six PCV13 sites and increased by 50% (95% CI −8% to 146%) in the four sites using PCV10 (alone or with PCV13). In 2015, PCV13 serotypes represented 20–29% and 32–53% of IPD cases in PCV13 and PCV10 sites, respectively.
Conclusion Overall IPD incidence in older adults decreased moderately after five childhood PCV10/13 years in 13 European sites. Large declines in PCV10/13 serotype IPD, due to the indirect effect of childhood vaccination, were countered by increases in non-PCV13 IPD, but these declines varied according to the childhood vaccine used. Decision-making on pneumococcal vaccination for older adults must consider the indirect effects of childhood PCV programmes. Sustained monitoring of IPD epidemiology is imperative.
- bacterial infection
- clinical epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
This study assesses the indirect effect of 5 years of childhood PCV10 and/or PCV13 programmes on invasive pneumococcal disease (IPD) in older adults across 10 European countries, using the same methodology.
What is the bottom line?
Previous studies in single countries and using different methodologies showed diverging results in terms of overall benefit (IPD incidence) and serotype replacement disease.
Why read on?
Our study reveals that the effect on IPD in older adults differs according to the PCV used in the childhood programme and highlights the continuing rise in non-PCV13 serotypes; these findings are important when deciding on pneumococcal vaccination policy for older adults.
Introduction
Streptococcus pneumoniae is associated with significant morbidity and mortality in older adults. The most severe form, invasive pneumococcal disease (IPD), includes bacteraemic pneumonia, meningitis and septicaemia.1 2 In recent European studies the annual incidence of IPD in persons aged ≥65 years ranged from 10 to 70 per 100 000.1–5 Pneumococcal conjugate vaccines covering 10 (PCV10) and 13 (PCV13) serotypes (table 1) have progressively replaced the 7-valent vaccine (PCV7) in the childhood vaccination schedule of most European countries during 2010 or 2011. PCV vaccination policies are heterogeneous between countries. In 2014, among 17 Western European countries, eight used PCV13 only, four used PCV10 only and five used both vaccines in the childhood vaccination programme.6 PCV13 has also been approved in adults for the prevention of IPD since 2011 and in 2015 the indication was extended to pneumococcal pneumonia.7
Childhood PCV vaccination may have an indirect effect on unvaccinated population groups, especially on older adults (in whom the incidence of IPD is very high), through a reduction in carriage of vaccine serotypes in vaccinated children, with subsequent reduction in circulation and transmission across all age groups. However, this indirect effect is also responsible for an increase in non-PCV serotypes, called serotype replacement. Indeed, after the introduction of PCV7, the decline in PCV7 serotype IPD was partly countered by replacement with non-PCV7 serotypes. A few countries have also recently reported an indirect effect in adults aged ≥65 years 3–4 years after PCV10/13 replaced PCV7 in the childhood vaccination programme.8–12 The decrease in overall IPD incidence after each PCV introduction is generally limited (<25%) because of serotype replacement disease, but its extent is unclear because of large confidence intervals.8–12
Some countries with established childhood PCV10/13 programmes are currently considering whether to introduce PCV13 vaccination in elderly people. A key question, therefore, is what additional value such a programme might offer over the indirect effect of a childhood PCV10/13 programme. In older adults, the polysaccharide 23-valent vaccine (PPV23) aims to protect against 12 PCV13 serotypes and 11 additional non-PCV13 serotypes, but its effectiveness against pneumococcal disease in this age group remains controversial.13 14
Serotype categories causing invasive pneumococcal disease according to the serotype content of vaccines
SpIDnet and I-MOVE+ are complementary European multicentre surveillance projects funded by the European Centre for Disease Prevention and Control (ECDC) and the European Commission since 2012 and 2015, respectively, to monitor the impact and effectiveness of PCV programmes in Europe. In 2015, SpIDnet and I-MOVE+ collected IPD data in adults from 13 sites across 10 countries: the Czech Republic, Denmark, England and Wales, Finland, France, Ireland, the Netherlands, Norway, Scotland, Sweden and the Madrid, Catalonia and Navarre regions of Spain. PCV7 was introduced in the childhood vaccination schedule (2001–2009) across all sites except Finland and replaced in 2010–2011 with either universal PCV13 (six sites), universal PCV10 (two sites) or both PCV10 and PCV13 (five sites, two with universal and three with non-universal PCV10/13), without catch-up vaccination. At the time of this study (2016), none of the sites routinely recommended PCV13 for all older adults. Nine sites recommended PPV23 for this age group; PPV23 uptake varied between 15% and 70% (table 2). Five sites recommended PCV13 for at-risk groups, together with PPV23.
Vaccination programme, population size, proportion of invasive pneumococcal disease (IPD) cases serotyped and number of IPD cases per year among older adults aged ≥65 years by site: SpIDnet/I-MOVE+ multicentre study
We estimated the indirect effect of the childhood PCV10/13 programme on IPD in adults aged ≥65 years (herein referred to as ‘older adults’) across these 13 sites during the first 5 years of PCV10/13 use, in order to support decision-making on the pneumococcal vaccine policy for older adults across Europe.
Methods
IPD surveillance systems and data sources
The 13 study sites conduct population-based IPD surveillance, with laboratory confirmation and serotyping of invasive pneumococcal isolates from cases residing in the catchment area. In 2015, reporting of IPD cases was mandatory in 11 sites and voluntary in two sites. IPD cases were defined according to the 2012 ECDC case definition.15 Aggregated data were collected from each surveillance site by calendar year and serotypes. All cases identified through surveillance were included in the analysis.
The reference laboratories at the respective surveillance sites used capsular reaction with specific antisera (Quellung reaction) or PCR for serotyping. Serotypes 6A and 6C were differentiated by PCR, Quellung or latex agglutination with specific antisera at all sites. The national reference laboratories participated in the external quality schemes organised by the ECDC during 2010–2014. Serotypes causing IPD were classified into categories according to the serotype content of vaccines (see table 1).
Analysis of data
We measured the indirect effect of the childhood PCV10/13 vaccination programme in older adults by comparing the incidence rate in this age group within a population with an established childhood PCV10/13 programme with the incidence rate in the same age group in the pre-PCV10/13 period.16 17 The pre-vaccine period represents the reference population (without a routine PCV10/13 programme) at each site.
For each site we accounted for missing serotype data by assuming the same serotype distribution in cases with and without serotype information, by calendar year. For three sites that reported a change in surveillance sensitivity over the surveillance period, we adjusted the number of reported cases to the sensitivity for each period, as described elsewhere.18–20 We computed annual incidence rates per site and serotype by dividing the numbers of cases adjusted for missing serotyping data and under-reporting by the respective source population.
For each site we thus compared the incidence of IPD in people aged ≥65 years before and after the introduction of childhood PCV10/13. We calculated site-specific incidence rate ratios (IRR) between 2009 and each of the PCV10/13 years (2011–2015) by serotype category. As data availability and the number of years after PCV7 introduction varied across sites in the pre-PCV10/13 period, we selected 2009 as the pre-vaccination period because it was the last pre-PCV10/13 year common to all sites. We performed sensitivity analysis using the average incidence during the PCV7 years as the pre-PCV10/13 period (and 2005–2008 for Finland). We considered 2010 as a transition year because PCV13/10 became available shortly before or during that year.
We computed pooled IRR and 95% CI by serotype category and year using random effects meta-analysis, as we assumed that the true indirect effect could vary across sites.21 We also performed pooled analyses stratified by the childhood vaccine used. We assessed statistical heterogeneity by estimating the between-study variance using tau-squared (τ²), which is less dependent on the number of sites and the precision of site estimates than other heterogeneity measures.22 Heterogeneity between studies was considered to be low if τ² <0.2, fairly reasonable for τ² between 0.2 and 0.5 and fairly high for τ² >0.5 and <1.0.23 The indirect effect of PCV on IPD in older adults was expressed as the percentage change in incidence ((1 − IRR)*100). Statistical analyses were performed using STATA 12.0 (StataCorp, Texas, USA).
Results
In 2015 the 13 sites covered around 32 million adults aged ≥65 years (table 2). PCV uptake in the infant programme exceeded 93% in 9/10 sites with universal vaccination, and ranged between 77% and 81% in the three sites with non-universal vaccination. A total of 56 194 IPD cases were reported among people aged ≥65 years during 2009–2015. Overall, serotyping was performed for 92% of the invasive pneumococcal isolates, excluding France where the incidence and serotype distribution are reported through two different systems without case reconciliation as described elsewhere,19 and the serotyping rate cannot be calculated. The serotyping rate ranged from 91% to 95% annually (for all sites) and from 88% to 100% across the sites (for all years).
Change in IPD incidence
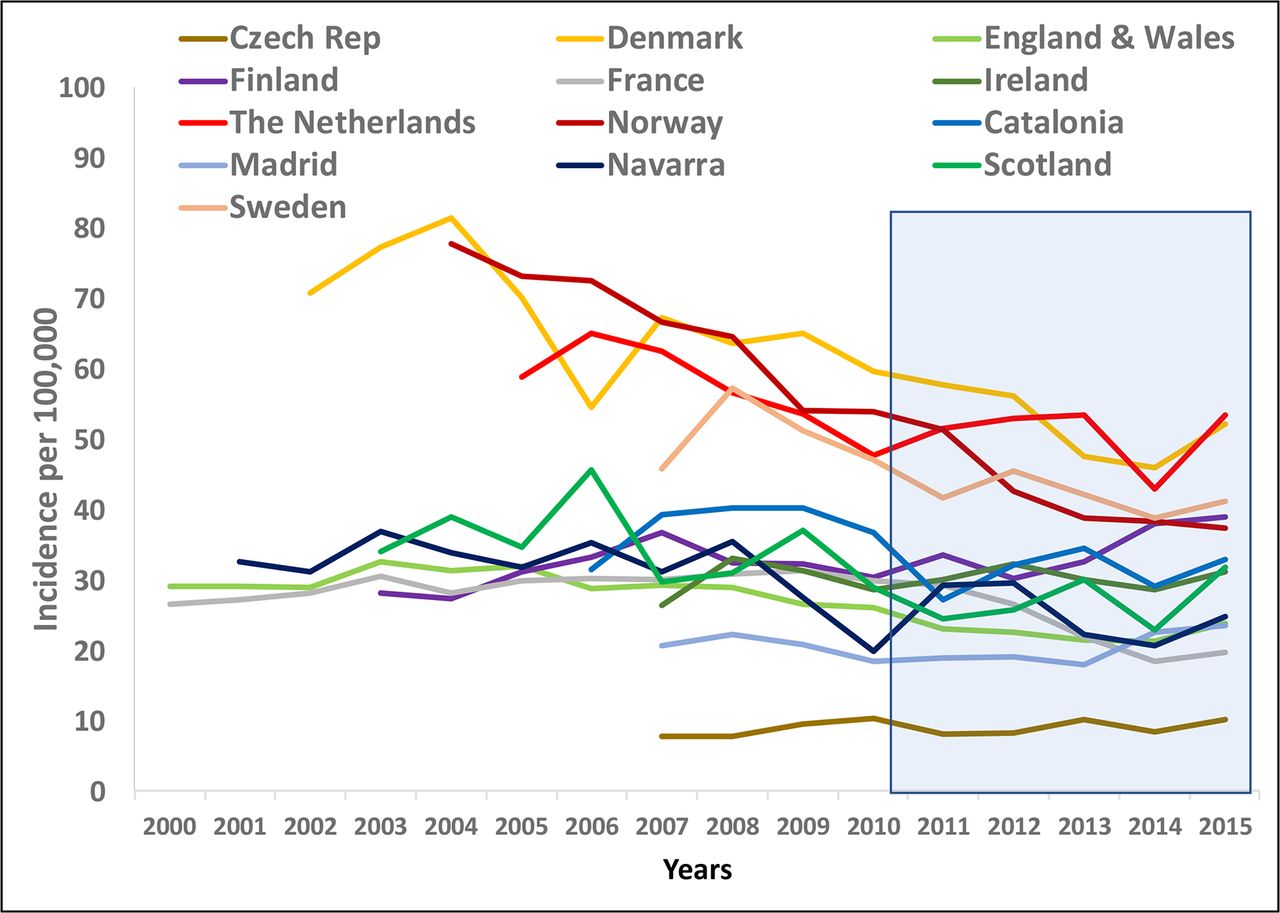
In the pre-PCV10/13 period the overall IPD incidence rates varied by site (figure 1), with higher rates in the Nordic countries and the Netherlands. Based on point estimates, IPD incidence rates decreased from 2009 to 2014 in 11/13 sites and increased from 2014 to 2015 in 12/13 sites (95% CI around IRR including 1 in 7/12 sites), exceeding the 2009 rates in 4/13 sites (95% CI around IRR including 1 in two sites, figure 2A). Pooled analysis estimated an overall decline of 9% (95% CI −4% to 19%) in IPD incidence in 2015 compared with 2009 (pre-PCV10/13 period, figure 3A, table 3).
Incidence rate ratio of invasive pneumococcal disease (IPD) per PCV10/13 year compared with 2009, 13 sites: SpIDnet/I-MOVE+ multicentre study

Overall incidence of invasive pneumococcal disease per site and years in persons aged ≥65 years over the period 2000–2015: SpIDnet/I-MOVE+ multicentre study.

Site incidence rate ratio by serotype category in 2015 compared with 2009: SpIDnet/I-MOVE+ multicentre study. (A) All. (B) PCV7. (C) Included in PCV10 and not in PCV7 (1, 5 and 7F). (D) Included in PCV13 and not in PCV10 (3, 6A and 19A). (E) Non-PCV13. (F) PPV23 non-PCV13. (G) Non-vaccine.

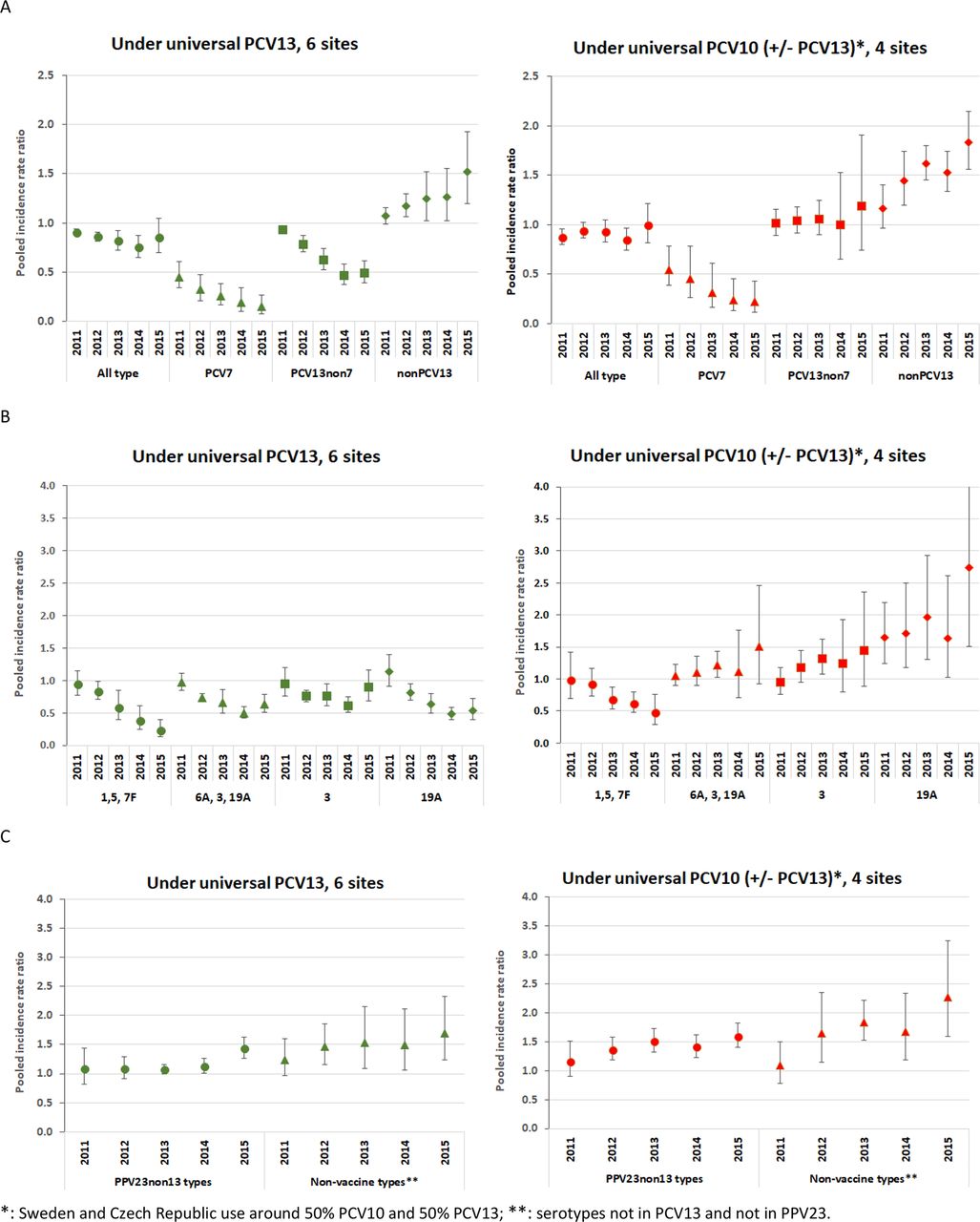
Pooled incidence rate ratio per serotype group over the PCV10/13 years (2011–2015) compared with 2009: SpIDnet/I-MOVE+ multicentre study.
The point estimate incidence of PCV7 serotype IPD declined across all sites except one (figure 2B). The pooled analysis indicated a progressive decline in incidence reaching 77% (95% CI 67% to 84%) in 2015 compared with 2009 (figure 3A, table 3). PCV13non7 serotype IPD incidence declined in 11/13 sites over the same period, with a pooled estimate decline of 38% (95% CI 19% to 53%) in 2015 (figure 3A, table 3). PCV10non7 serotype IPD incidence decreased across all sites (figure 2C), reaching 73% (95% CI 59% to –82%) decline by 2015 in the pooled analysis (figure 3B, table 3). Changes in PCV13non10 serotype IPD incidence varied by site; site-specific IRR ranged between 0.4 and 2.9 in 2015 compared with 2009 (figure 2D). The pooled analysis showed a decline in PCV13non10 serotype IPD incidence up to 2014 followed by an increase in 2015 (figure 3B) based on point estimates, although with overlapping 95% CI around the IRR. The pooled IRR for serotype 3 IPD fluctuated around 1 during the PCV10/13 period (figure 3B, table 3). The incidence of IPD due to serotype 19A declined over time but with wide confidence intervals (figure 3B, table 3). When the average PCV7 period was used as the pre-vaccine period instead of the 2009 year, similar patterns were observed with a decline of 11% (95% CI 0% to 21%) in overall IPD, 83% (95% CI 73% to 89%) in PCV7 serotypes and 33% (95% CI 11% to 50%) in PCV13non7 serotype IPD incidence by 2015.
The point estimate incidence of non-PCV13 serotype IPD increased in 12/13 sites over the PCV10/13 period (figure 2E), with a pooled increase of 63% (95% CI 39% to 92%) in 2015 (figure 3A). Pooled IRR was similar for the 11 non-PCV13 serotypes included in PPV23 (PPV23non13) (IRR 1.53, 1.39–1.68) and the non-vaccine serotypes (1.78, 1.41–2.24; figure 3C).
Changes in incidence according to childhood vaccination
We compared pooled IRR for six sites with universal PCV13 with those of four sites with universal PCV10, used exclusively (two sites) or in similar proportion with PCV13 (two sites) (figure 4). From 2009 to 2015, the overall IPD incidence declined by 14% in PCV13 sites (95% CI −4% to 30%) and by 1% (−21% to 18%) in PCV10 sites. IPD due to PCV7 and PCV10non7 serotypes decreased in both groups, by 85% (95% CI 82% to 88%) and 77% (95% CI 60% to 86%) in PCV13 sites and by 78% (95% CI 57% to 89%) and 53% (95% CI 24% to 71%) in the sites using PCV10, respectively. IPD due to PCV13non10 serotypes decreased by 37% (95% CI 22% to 49%) in PCV13 sites and increased by 50% (95% CI −8% to 146%) in the sites using PCV10. Overall, PCV13non7 serotype IPD declined by 51% (95% CI 39% to 61%) in PCV13 sites and increased by 19% (95% CI −26% to 90%) in PCV10 sites, although with overlapping 95% CI. The incidence of IPD due to serotype 19A decreased by 47% (95% CI 38% to 61%) in PCV13 sites and increased by 174% (95% CI 51% to 399%) in PCV10 sites, with the largest increases seen in 2015. The incidence of serotype 3 IPD fluctuated in both groups, but decreased in the first 4 years among PCV13 sites and tended to increase in PCV10 sites. Non-PCV13 type IPD showed similar trends in both groups.
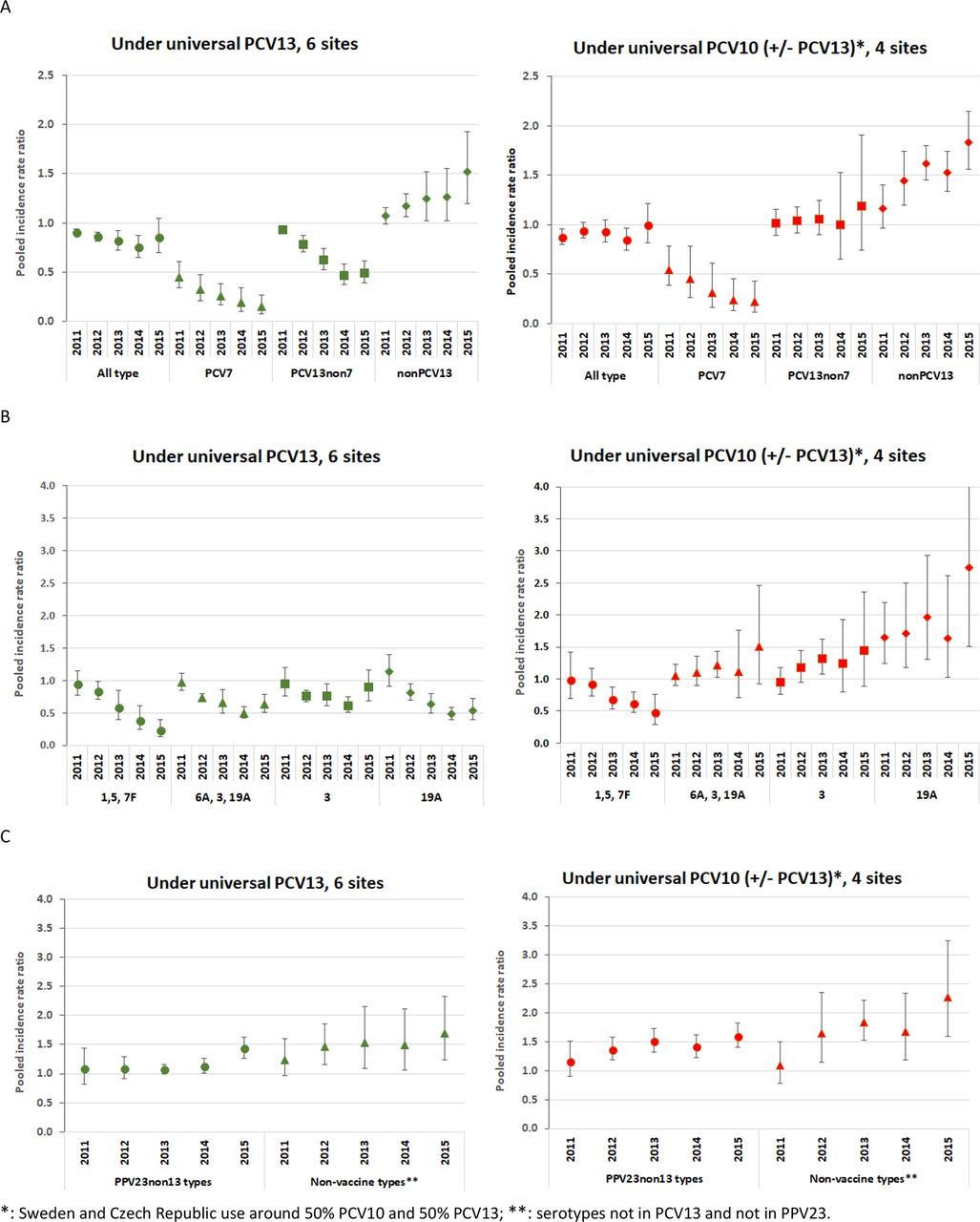
Pooled incidence rate ratio per serotype group over the PCV10/13 years compared with 2009 by vaccine policy: SpIDnet/I-MOVE+ multicentre study.
Serotype distribution among IPD cases in older adults during 2015
In 2015, PCV7 serotypes represented <20% of all IPD cases in older adults at each site (figure 5), with a range of 2–4% in PCV13 sites, 6–16% in sites using PCV10 and 10–19% in the four sites with limited PCV7 vaccination (none or median uptake ≤60%) before the introduction of PCV10/13 (i.e. Catalunya, Navarra, Czech Republic and Finland). Note that Madrid had universal PCV7 vaccination between 2007 and 2010 (vaccine uptake >90%), replaced by universal PCV13 vaccination up to May 2012. PCV10non7 serotypes were responsible for ≤5% of IPD cases in all sites except one. PCV13non10 serotypes caused 11–23% of IPD cases in PCV13 sites and 20–36% in PCV10 sites. Altogether, PCV13 serotypes represented 20–29% of IPD cases in PCV13 sites and 32–53% in sites using PCV10. The PPV23non13 serotypes were responsible for 37–54% and 22–46% of IPD cases in PCV13 and PCV10 sites, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of serotypes out of all invasive pneumococcal disease in 2015 by serotype group, site and vaccination policies: SpIDnet/I-MOVE+ multicentre study.
Heterogeneity testing
Based on τ², heterogeneity between studies was low or fairly reasonable in all pooled analyses (τ²<0.5), except for serotype 19A across all sites (τ²=0.5 in 2015). Heterogeneity was low (τ²<0.2) in 90% of analyses by vaccine policy and fairly reasonable (τ²=0.2–0.5) in the remaining 10%.
Discussion
Our pooled analysis of 13 sites from 10 European countries identified a large indirect effect of childhood PCV programmes on IPD among older adults, with IPD caused by PCV7 and PCV10 serotypes declining by more than 70% after five PCV10/13 years compared with the pre-PCV10/13 period. The three serotypes included in PCV13 and not in PCV10 declined moderately (20%), but the trends differed by site according to whether the childhood vaccination programme included PCV10 or PCV13 in individual sites. The incidence of IPD due to non-PCV13 serotypes increased by 63%, restricting the overall changes in IPD incidence to a 9% decline, although with wide confidence intervals, after 5 years of the childhood PCV10/13 programme.
The year-on-year increase in the incidence of non-PCV13 serotypes during the five PCV10/13 years, suggesting serotype replacement in disease, is consistent with recent European reports from other sites during at least four PCV10/13 years and counters the marked declines in vaccine serotype IPD incidence, thereby restricting the overall benefits of the childhood programme on IPD in older adults. In Italy and Germany the incidence or number of reported cases in adults aged ≥65 years tended to increase over the PCV13 period.24 25 In contrast, in the USA the incidence of non-PCV13 IPD did not increase in older adults after 3 years of the childhood PCV13 programme.12 Differences in surveillance methodologies, case definitions and clinical practices, as noted since the PCV7 era, along with the shorter surveillance interval in the US study may at least partly explain this difference.26 27
The incidence of PCV7 serotype IPD declined substantially. By 2015 these serotypes represented <5% of IPD cases among the older adults in sites where universal PCV13 replaced PCV7 vaccination. In countries with no or limited PCV7 use prior to PCV13 introduction, however, PCV7 serotypes accounted for 10–19% of IPD cases among the older adults in 2015.
We identified important differences in indirect effects according to the PCV used in the childhood programme. After 5 years the point estimate decline in overall IPD among older adults was greater in the six sites with universal PCV13 vaccination compared with the four sites with universal PCV10, used exclusively or in equal proportions with PCV13, although with wide confidence intervals. This difference was partly due to PCV13non10 serotypes, which decreased by 37% in PCV13 sites compared with a 50% increase (with wide confidence intervals) in sites using PCV10. This was driven primarily by diverging trends in the incidence of serotype 19A IPD and could be expected as PCV10 does not contain serotype 19A. IPD incidence due to this serotype also increased rapidly in countries with established PCV7 programmes prior to PCV13 implementation. Although a decline in serotype 19A IPD incidence has been observed in vaccinated children with PCV10,28 29 potentially through cross-protection from antibodies against serotype 19F, this may not be sufficient to offer indirect (herd) protection for serotype 19A IPD among older unvaccinated individuals.30 Similar differences were observed in Sweden between counties vaccinating with PCV10 and those vaccinating with PCV13.5 For serotype 3, the pooled IRR was <1 in PCV13 sites and >1 in PCV10 in 2012–2015, but confidence intervals were too large to allow any conclusive interpretation. Although the incidence of serotype 3 IPD declined in PCV13 sites in the first 4 years after PCV13 introduction, its increase in 2015 is difficult to explain, thus precluding any conclusion about the ability of the childhood PCV13 programmes to generate herd effects against this serotype. The increase in PCV13non10 serotypes in the four PCV10 sites is problematic because serotypes 3 and 19A already rank among the most prevalent causes of invasive and non-invasive pneumococcal disease among older adults.2 11
Currently, a major question is whether a PCV13 programme for older adults would present an added value compared with the indirect effect of the childhood PCV10/13 programme. The continuing decline in PCV10/13 serotype IPD in older adults through the indirect benefits of the childhood PCV10/13 programme in this study, as in other European studies,10 23 25 31 32 is one factor which explains why most European countries do not advise routine PCV13 for older adults. Our study is, however, the first multi-country study to estimate residual PCV13 disease and differing trends depending on the country’s childhood PCV policy. In PCV13 sites, PCV13 serotypes represented <30% of all IPD among older adults in 2015 and the incidence of PCV13non7 serotype IPD halved after five PCV13 years. In contrast, in the PCV10 sites, PCV13 serotypes were responsible for one-third to one-half of IPD cases among older adults in 2015 and the incidence of PCV13non7 serotype IPD tended to increase over the five PCV10 years. Although future trends cannot be predicted, our results suggest that, in countries using PCV10 in the childhood schedule, a higher proportion of IPD cases would be targeted by a PCV13 programme for older adults. This group, however, comprises more than 30 1-year age cohorts and such a programme would only offer direct protection to vaccinated older adults.
The incidence of PPV23non13 serotypes rose by 50% after 5 years of the childhood PCV10/13 programme and will most likely continue to increase with more years of PCV10/13 use; these 11 serotypes were responsible for 22–54% of IPD among older adults per site in 2015. A recent meta-analysis assessing indirect PCV effects reported a smaller increase in PPV23non13 serotypes in older adults (IRR 1.18 (1.12–1.25)), but the analysis mixed data across different continents, with variable pre-vaccine and post-PCV10/13 periods.23 We did not take into account PPV23 use which is recommended for older adults in some countries. As our study period does not cover the years before PPV23 introduction, this could bias our estimates only if PPV23 uptake varied during the study period, which was not the case. Moreover, we did not identify any different trends among PPV23non13 serotypes by PPV23 use, as the sites with the highest uptake (England and Wales, and Scotland, ~70%) had similar IRR to the pooled estimate (1.46 and 1.60, respectively, compared with 1.50).
In 2015 the overall IPD incidence in older adults increased in 12/13 sites compared with 2014 (although 95% CI overlapped in 7/12 sites), almost entirely due to non-PCV13 serotypes. The exception was Norway, but preliminary data suggest that the IPD incidence increased by 18% between 2015 and 2016 because of an increase in IPD due to non-PCV13 serotypes; preliminary data from some sites indicate a further rise in 2016, again due to non-PCV13 serotypes.5 33 34 Monitoring IPD serotype trends across all age groups in countries with ongoing childhood PCV10/13 programmes is therefore essential.
The reasons for higher pre-vaccine incidence rates in four countries (the Nordic countries and the Netherlands) were not explored in our study. No difference in surveillance sensitivity was identified in these sites, but substantial increases in overall IPD incidence prior to PCV7 introduction (1995–2004) were reported in older adults in these four countries, mostly due to rises in serotypes 1, 4 and 14.35–39 In other sites with longer pre-PCV7 data in our study, such as the UK and France, IPD incidence rates were stable (figure 1). We hypothesise that regional circulation of specific serotypes or pneumococcal clones caused these higher incidences, although differences in social contact patterns and case detection cannot be excluded.
Our results cannot be easily compared with studies from other sites, which were usually restricted to single sites, included shorter post-PCV13 periods (2–3 years) or used an average incidence over the post-vaccine period.12 23 25 40 The added value of our study is the pooling of 13 sites from 10 European countries, coverage of five PCV10/13 years and IRR estimations for each PCV10/13 year. There are, however, some limitations. First, methodologies comparing pre- and post-vaccination incidences are prone to biases, whereby changes in other factors over time such as case detection (eg, blood culturing frequency), reporting and other health interventions may be attributed to the vaccination programme. We partly addressed that risk by adjusting for surveillance sensitivity whenever possible. Although we cannot exclude biases due to changes in IPD case detection and surveillance, these tend to improve in post-vaccine periods and would underestimate the vaccine effects.17 19 41 Second, we expect heterogeneity across sites due to differences in healthcare practices, pre-vaccine epidemiology and vaccination policies. We attempted to address this by using random effects meta-analysis and performing stratified analysis by PCV policy. We assumed that these differences across sites would be constant over time, limiting their influence on relative measures of effect such as the IRR. Reassuringly, the τ² values suggest limited statistical heterogeneity. Third, the selected pre-PCV10/13 reference period may influence effect estimates. We selected 2009 as the last year before PCV10/13 introduction for all sites, but a single year may be more prone to natural fluctuations. Using the average annual incidence after PCV7 introduction, however, we observed similar patterns in IRR, but with slightly differing values, likely reflecting some additional PCV7 effect on PCV7 and non-PCV7 serotypes in sites with longer periods of PCV7 included in the analysis. We therefore believe that using 2009 as reference provides a more accurate estimate of changes due to PCV10/13 only. Finally, given the variability in pneumococcal serotype epidemiology and PCV history across the participating sites, we cannot infer our findings to the rest of Europe.
Conclusion
We report the indirect effect of 5 years of the childhood PCV10/13 programme on the incidence of IPD in older adults across 13 sites in 10 European countries. The large decline in IPD due to vaccine serotypes was partly countered by increases in non-PCV13 serotypes, resulting in a limited net effect on overall IPD. Our findings suggest that the potential benefit of a PCV13 programme in older adults progressively reduces over time because of the progressive decline in PCV13 serotype IPD and the gradual rise in non-PCV13 serotype IPD across that age group. The substantial and increasing proportion of IPD due to the additional PPV23 serotypes suggests that the advantage of PPV23 over PCV13 in terms of serotypes covered may increase over time in older adults. Our data also suggest that IPD trends in older adults differ according to the childhood PCV used, especially relating to serotype 19A. Policy makers need to take into account the indirect impact of childhood programmes when considering vaccination programmes for older adults in their decision-making process. Our results also indicate that vaccines targeting older adults should include other (or at least more) serotypes, or provide a wider mechanism of protection against pneumococcal disease than against specific capsular serotypes.
The evolution of this indirect effect is difficult to predict. In particular, the consistent observation of an increase in IPD in 2015 across the European sites, the differing trends in serotype 19A and the rise in non-PCV13 serotypes raise concerns. This highlights the need to further monitor IPD serotype trends in future years as more infant cohorts receive PCV10/13.
References
Footnotes
Contributors GMH performed the statistical analyses of the pooled data and wrote the manuscript. CS was responsible for study coordination, collected data from the SpIDnet sites, contributed to the statistical analyses and writing of the manuscript. SNL and RW contributed to the writing of the manuscript. LPC provided technical support for the study design. PK, PV-B, SNL, NKF, JPN, HR-K, AL, EV, JM, MC, MK, H-CS, AvdE, BAW, DFV, EMD, JK, AS, PC, CM-A, MO, PL, MG, JC, EM and BH-N coordinated the collection, validation and preparation of data at site level. All authors read, commented on and approved all versions of the manuscript. Authors are included in alphabetical order of the country of the participating sites, except for first and last authors.
Funding This study was co-funded by participating countries, the ECDC (SpIDnet project) and the European Commission (Horizon 2020, I-MOVE+).
Competing interests The following authors report funding for research projects, travels or consultancy outside the submitted work: H-CS (project sponsored by Pfizer); ZH (travel grant from Pfizer), SNL (research including GSK, Pfizer, Sanofi Pasteur on behalf of St George’s University of London and Public Health England (PHE)); NKF (employed by PHE Respiratory and Vaccine Preventable Bacteria Reference Unit and PHE Immunisation that provided serotype surveillance reports to Affinivax, Pfizer and GSK); HR-K and JJ (employed by the National Institute for Health and Welfare that received research funding from GSK for the conduct of a trial of PCV10); AvdE (Pfizer grant for an investigator initiated project, consultancy fees from GSK, participation in the Pfizer Scientific Advisory board); CM-A (fees from GSK and grants from Pfizer); EV (Pfizer grants and personal fees); MC (Pfizer grants and personal fees); HH (research funding from Pfizer and Astellas).
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Czech Republic: Helena Sebestova, Marek Maly. Denmark: Kurt Fuursted, Tine Dalby, Victoria F de Casadevante, Zitta Harboe, Charlotte Sværke Jørgensen. England and Wales: Sarah Collins, Nick Andrews, Abdelmajid Djennad, Richard Pebody. Finland: Jukka Jokinen. France: Emmanuel Belchior, Daniel Levy-Bruhl, Scarlett Georges, Marie-Cécile Ploy, Jacques Gaillat. Ireland: Robert Cunney, Hilary Humphreys, Suzanne Cotter. The Netherlands: Elisabeth Sanders, Wim van der Hoek, Guy Berbers, Hester de Melker. Norway: Marianne Bergsaker. Scotland: Claire Cameron, Barbara Denham. Catalonia, Spain: Conchita Izquierdo, Sonia Broner, Roman Pallarés. Madrid, Spain: Luis Garcia, Juan Carlos Sanz. Navarra, Spain: Carmen Ezpeleta, Alberto Gil-Setas. Sweden: Tiia Lepp, Ann Lindstrand, Jessica Darenberg. ECDC: Edoardo Colzani SpIDnet /I-MOVE+ coordination team: Marta Valenciano, Alain Moren.
Linked Articles
- Editorial