Article Text

Abstract
Introduction Cystic fibrosis (CF) is a multisystem disorder. Treatment is complex and evidence for treatment decisions may be absent. Characterising gaps in the research evidence will highlight treatment uncertainties and help prioritise research questions. We systematically identified the evidence gaps for treatment decisions in CF.
Methods We searched for systematic reviews and guidelines on treatment interventions in CF. Two researchers identified eligible reviews with arbitration from a third. Using a structured framework, we extracted and characterised evidence gaps.
Results There were 73 reviews and 21 guidelines that met our inclusion criteria. From these, we identified 148 evidence gaps across a range of treatment areas. We found 111 evidence gaps through systematic reviews and a further 37 from guidelines. The reason for an evidence gap could only be reliably characterised for systematic reviews. In most cases, there was more than one explanation—most commonly few or no trials (97/111 evidence gaps). Other important factors leading to evidence gaps were small sample size (49/111), inadequate duration of follow-up (38/111) or intervention (37/111) and factors relating to outcomes (35/111). Evidence gaps from both systematic reviews and guidelines fell into the following categories: Respiratory (91); Gastrointestinal (20); PhysiotherapyandExercise (16); Musculoskeletal (6); Endocrine (4); Basic defect of CF (8); Psychosocial (2); Ears, Nose and Throat (1).
Conclusions We have compiled an up-to-date list of treatment uncertainties in CF and the reasons for these uncertainties. These can be used as a resource to aid researchers and funders when planning future trials.
PROSPERO registration number Pre-results; CRD42015030111.
- cystic fibrosis
Statistics from Altmetric.com
Key messages
What is the key question?
What are the evidence gaps in treatment decisions for cystic fibrosis?
What is the bottom line?
We have identified 148 gaps in the evidence for treatment decisions in cystic fibrosis. We list these in full and characterise the reasons for the gaps.
Why read on?
These evidence gaps provide a systematic evidence-based starting point for the next generation of patient-centred, clinical research studies in cystic fibrosis.
Introduction
Life expectancy in cystic fibrosis (CF) is improving, with current best estimate of median survival being greater than 50 years for those born in the year 2000.1 The cost of this improvement in mortality is a high treatment burden, leading to a huge impact on daily activities and significant effect on quality of life.
Doctors, other members of the CF multidisciplinary team, people with CF and their families should be guided by best evidence when making treatment decisions in CF. Systematic reviews are undertaken to identify the evidence for benefit (or harm) from an intervention in order to inform guidelines and guide clinical practice. However, systematic reviews may be unable to reach a strong conclusion due to insufficient clinical trials, few participants or poor trial methodology. One recent study found that only 96 of 283 (34%) systematic reviews in paediatric respiratory medicine were able to make a strong conclusion relevant to clinical practice.2 Conversely, ‘empty’ systematic reviews have been shown to demonstrate evidence gaps, which can focus the attention of the research community and lead to trials which answer these questions.3
CF is a multisystem disorder and is the focus of intense research interest, particularly in the area of drugs which modulate CF transmembrane conductance regulator (CFTR). While it is hoped that the CFTR modulators will provide transformative therapy for many people with CF, it is likely that other ‘conventional’ treatments will still be necessary. Pragmatic clinical research on conventional treatments is therefore still needed. The clinical research budget is finite and the pool of patients eligible for trials is limited (10 000 UK,4 28 000 USA).5 Therefore, the research effort should be focused on providing clear answers to important treatment uncertainties which will in turn guide evidence-based practice. Identifying the important knowledge gaps in the treatment of CF will allow limited resources to be used appropriately.
Here, we have identified these gaps by reviewing the evidence base for treatment decisions in CF through a systematic review of systematic reviews and CF guidelines. We have characterised the reasons for the uncertainties to inform future trial design.
Methods
Our full protocol can be found on PROSPERO (CRD42015030111). Systematic reviews and guidelines which included treatment interventions in people of any age with a formal diagnosis of CF were eligible for inclusion.
We undertook a search for systematic reviews of the following databases in December 2015: Embase, MEDLINE, CINAHL, The Cochrane Library and PubMed. Search strategies were devised iteratively and search terms kept broad to increase sensitivity (online supplementary S1). No date or language limits were applied to the search, although we only included reviews which were available in English. We conducted an additional search of the Cochrane database in February 2017. We excluded reviews covering diagnosis, newborn screening or those concerning diagnostic test accuracy as these did not fall under our definition of treatments. We also excluded those concerning policy, training of physicians or organisation of care (eg, specialist CF clinics versus general clinic care). However, systematic reviews including trials of timings and duration of intervention, combinations of interventions and stopping interventions were considered. Earlier versions of the same review were excluded.
Supplemental material
The ROBIS tool (risk of bias in systematic reviews) was used to assess risk of bias and quality of non-Cochrane reviews.6 Only reviews deemed to be at low risk of bias were included. Several studies have reported that Cochrane reviews are of a very high quality, so we accepted these reviews without assessing risk of bias and quality.7 8 Search results were downloaded to Endnote (V.X7) and checked for duplicates. The online program Covidence9 was used for screening by two reviewers.
Two reviewers (NJR, SS) individually extracted data from all included reviews. ‘Google’ forms adapted from ‘Framework for Determining Research Gaps During Systematic Review’10 (online supplementary S2 and S3) were devised and piloted prior to data extraction. Results were compared and an agreed set of extracted data produced for each review. Evidence gaps were defined as an area of treatment where available information limited the ability of the review authors to form conclusions about effect. We extracted the main reason plus any additional reasons for each uncertainty. Reasons were categorised as follows:
Insufficient or imprecise information
No studies.
Limited number of studies.
Sample sizes too small.
Estimate of effect imprecise from meta-analysis.
Risk of bias
Inappropriate study design.
Major methodological limitations.
Inconsistency or consistency uncertain
Only one study.
Inconsistent results across studies.
Not the right information
Wrong population.
Inadequate duration of intervention.
Inadequate duration of follow-up.
Important outcomes not reported.10
We also recorded population and intervention studied, comparator used, outcomes measured and setting for the study. Any discrepancies were mediated by a third reviewer (AS). Data were collated using Excel. We identified themes and compiled a table of known treatment uncertainties with reason for each. Gaps identified from more than one review of the same topic were merged.
We searched the following for CF treatment guidelines: US National Guideline Clearing House (www.guideline.gov); UK National Institute for Health and Care Excellence (www.nice.org.uk); US CF Foundation (www.cff.org); UK CF Trust (www.cysticfibrosis.org.uk); European CF Society (http://www.ecfs.eu); Cystic Fibrosis Federation of Australia (www.cysticfibrosis.org.au) and ‘Open Grey’ (www.opengrey.eu). Our search of guidelines was for the period 2005–2015. We used the same inclusion and exclusion criteria as with systematic reviews. Guidelines were read in their entirety and areas highlighted by authors as evidence unclear or uncertain were identified and recorded using form online supplementary S4. We were not able to fully characterise the gaps identified through our review of treatment guidelines because the documents did not always include the underlying evidence for each guideline recommendation (including which pieces of evidence were missing and why).
Supplemental material
Results
Description of studies
The searches identified 1042 articles (after duplications were removed), of which 73 met our inclusion criteria (see online supplementary S5 for references). We excluded 691 on title and abstract alone, and 278 from the full-text article with reasons described (Preferred Reporting Items for Systematic Reviews and Meta-Analyses chart figure 1A). Two non-Cochrane reviews met the inclusion criteria, one of which was excluded on ROBIS tool assessment due to high risk of bias (online supplementary S6).
Supplemental material
Supplemental material
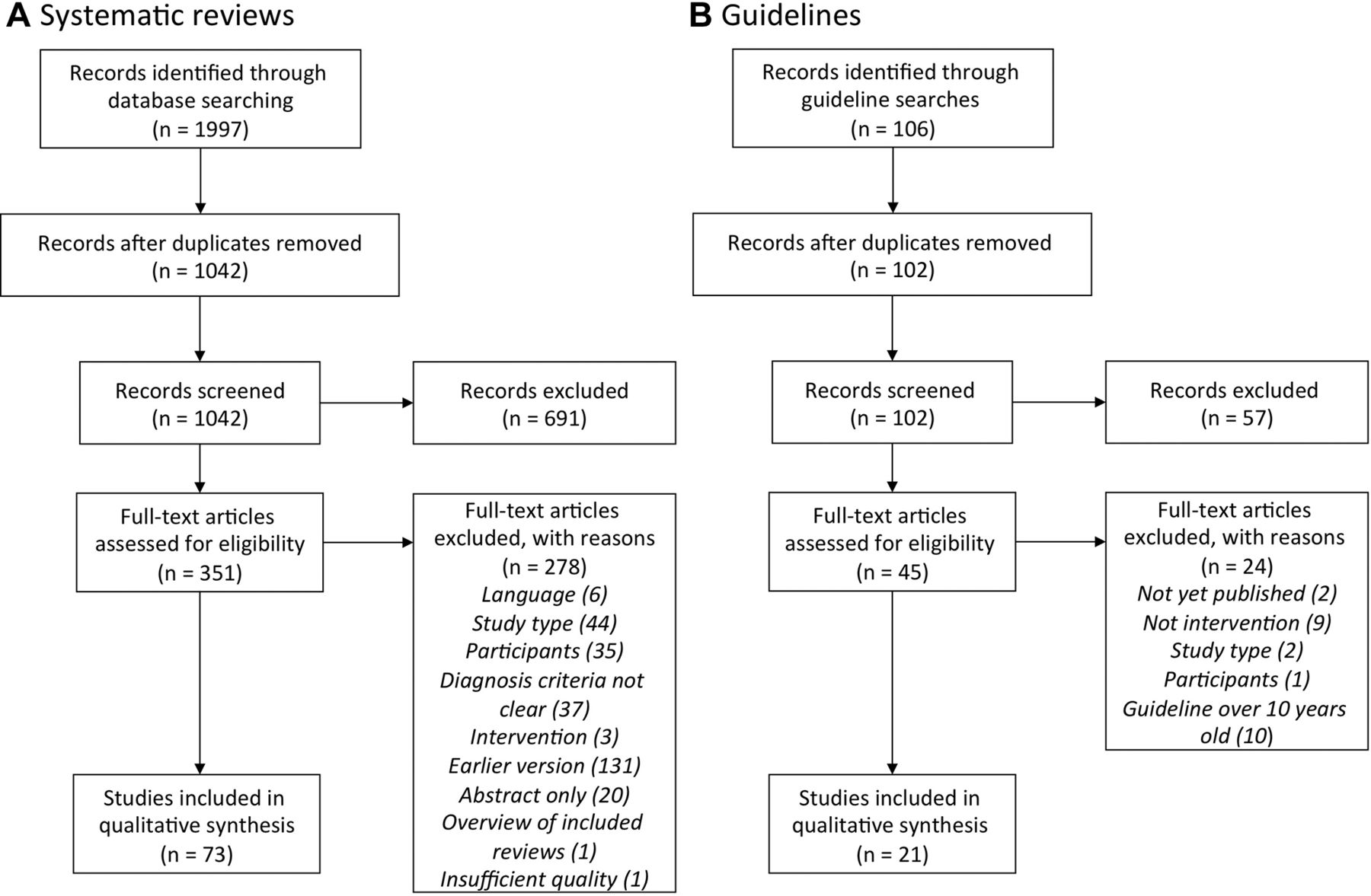
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagrams to show selection of studies for inclusion. (A) Selection of systematic reviews. (B) Guideline selection.
Within the included systematic reviews, there were a total of 466 trials, with 23 591 participants ranging in age from newly diagnosed infant to adult (online supplementary S7). Fourteen systematic reviews found there were no trials for their topic area. Two reviews covered the same topic area (CFTR modulators). Within the systematic reviews, 460 of the included trials were randomised controlled trials (RCTs) of which 263 were of parallel group design, 195 were cross-over and 2 were unknown. The guidelines searches identified 102 guidelines (after duplicates were removed), of which 21 met our inclusion criteria (figure 1B, see online supplementary S8 references).
Supplemental material
Supplemental material
Due to unclear diagnostic criteria, 37 reviews were excluded. The date range for these reviews is 1998–2015 with only six being published before The European Working Group proposing diagnostic criteria in 2006.11 An additional analysis of these 37 excluded reviews showed that only 13 would have met all inclusion criteria and passed ROBIS assessment. Of these, four were covered by already included reviews, but nine could have added more gaps (online supplementary S9). Only two non-Cochrane reviews met our inclusion criteria and only one of these was deemed sufficient quality to be included.12
Supplemental material
The included reviews covered a wide variety of treatment interventions across the field of CF. Figure 2A shows the proportional representation of areas covered in this study. The majority of the systematic reviews (55%) covered respiratory interventions, followed by gastroenterology (15%). Figure 2B shows further breakdown of respiratory intervention reviews by type with 43% of respiratory reviews focusing on antibiotic treatment. From the 73 included reviews, there was sufficient good-quality evidence to identify 30 statements which can robustly support treatment decisions in CF (‘known knowns’) (table 1). When looking at funding sources for trials that fed into these known knowns, 27% were funded by pharma, 31% by charity and 14% by governments (online supplementary S10).
Supplemental material

Themes of systematic reviews and evidence gaps. (A) Categories of the included systematic reviews with the percentage of reviews falling in each category. (B) Number of included reviews in each sub category of the respiratory reviews. (C) Relative percentage of evidence gaps falling within each category. (D) Reasons for the evidence gaps with number attributable to each reason. ABPA, allergic bronchopulmonary aspergillosis; ENT, ear, nose and throat; NIV, non-invasive ventilation.
‘Known knowns’ treatment questions where there is good evidence, from randomised controlled trials, to guide practice
Description of evidence gaps
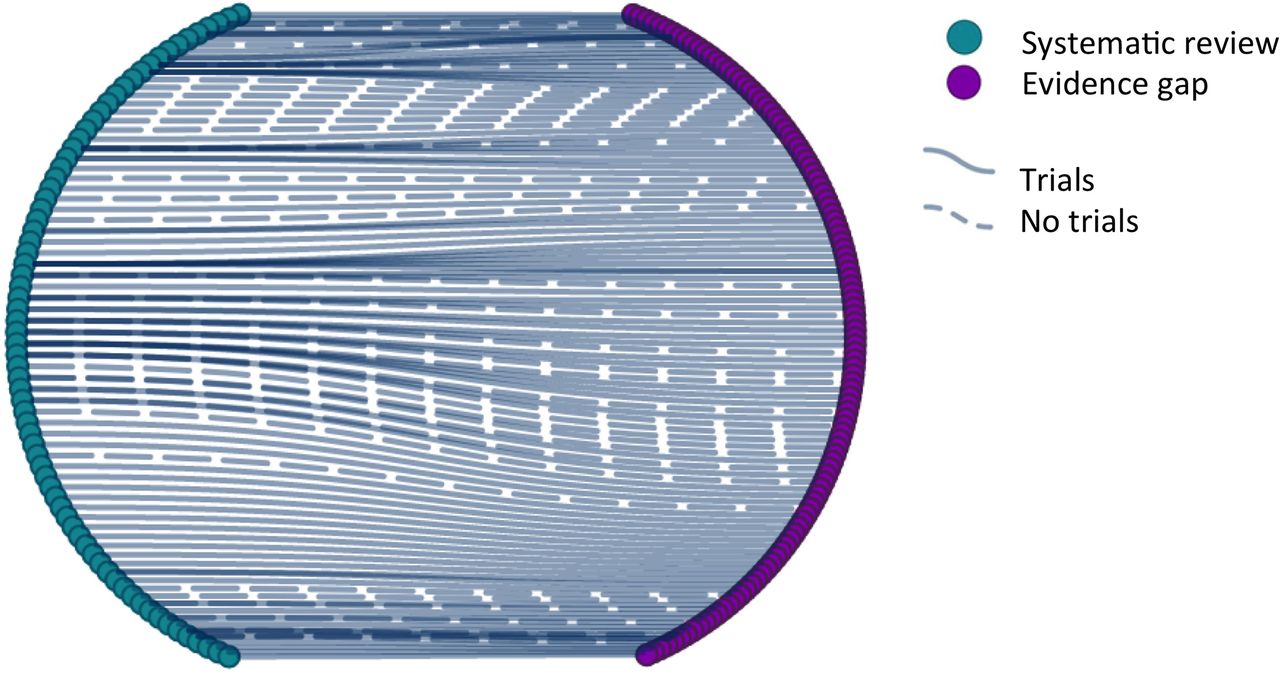
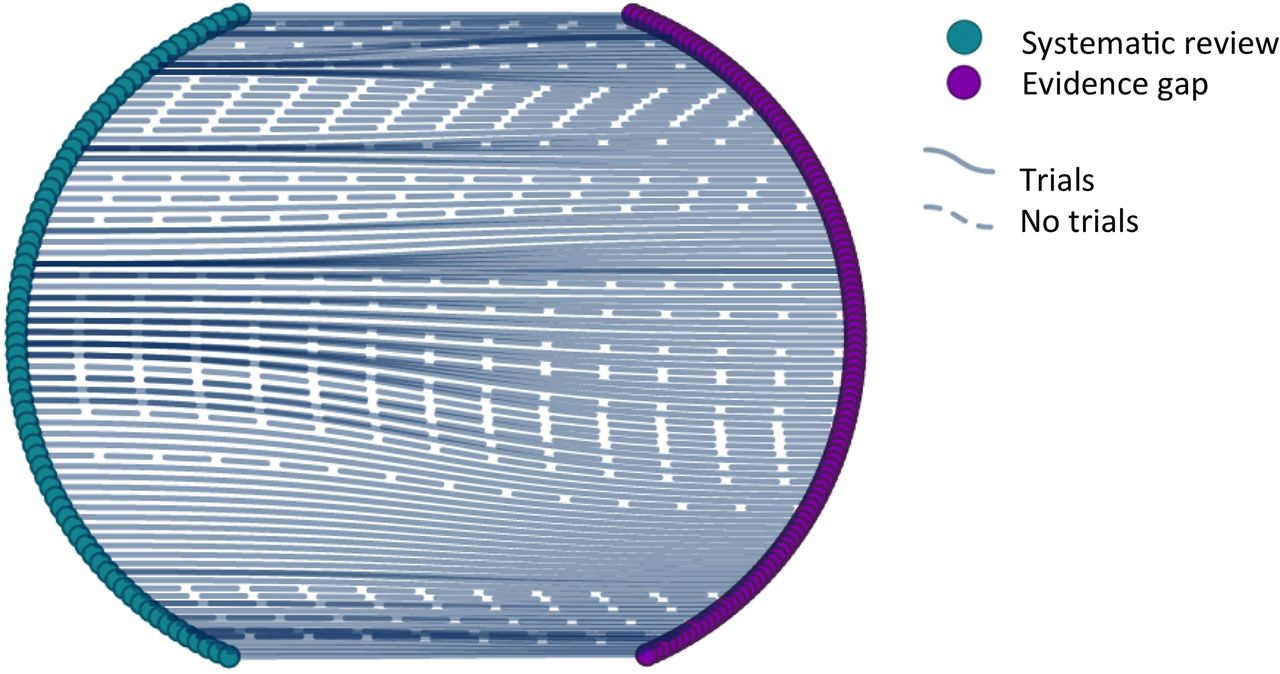
We identified and characterised 111 individual evidence gaps from the 73 included systematic reviews as highlighted by their authors (see supplementary table S11). Duplicate gaps noted from separate reviews on the same topic area were combined. The interactive ‘Prayle plot’2 (figure 3) illustrates the evidence gaps and their source systematic review.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Gaps in the evidence base for treatment decisions in cystic fibrosis. Prayle plot to show the links between systematic review and evidence gaps. Each individual evidence gap is represented by a purple node and each systematic review by a green node. A solid line connecting an evidence gap to a systematic review indicates that there are trials that have occurred to try and answer the question. A broken line indicates that there have been no relevant trials included in the systematic review. An interactive web-based version of the Prayle plot (which loads in all recent major browsers) is available online (https://www.nottingham.ac.uk/~mszap3/gaps_review_figure.html) and allows the reader to explore the underlying data further including reasons for each evidence gap and to break the plot down to view by topic area.
Many of these gaps can be split further to include subquestions, for example patient groups, intervention comparisons and differing drug regimens. Figure 2C shows the proportional distribution of these 111 ‘known unknowns’ across different areas of CF. As one would expect, in areas where there are more systematic reviews, we were able to identify more evidence gaps.
We found 74 gaps from the 21 included guidelines, of which 37 were novel (see online supplementary S12). As guidelines did not always include the underlying evidence for each recommendation, we have been unable to characterise these to the same degree as the gaps identified from systematic reviews.
Supplemental material
Evidence gaps (148), from both systematic reviews and guidelines, fell into the following categories: Respiratory (91); Gastrointestinal (20); Physiotherapy and Exercise (16); Musculoskeletal (6); Endocrine (4); Basic defect of CF (8); Psychosocial (2); Ears, Nose and Throat (1). See online supplementary figures S9 and S10.
Reason for evidence gaps
In the case of gaps identified from systematic reviews, we classified why each one occurred, as described above. The interactive figure 3 and online supplementary table S11 show the reasons for each gap. Most of the gaps existed for more than one reason. The bar chart in figure 2D shows all contributing factors.
More than 87% of the 111 evidence gaps, identified through systematic reviews, existed due to few (n=62) or no studies (n=35). Small sample size was a factor in 49 gaps (44%) and meta-analysis showed imprecise estimate of effect for three gaps (3%). Inappropriate study design contributed towards 12 gaps (11%) and major methodological limitations were implicated in 41 gaps (37%). With four gaps (4%), consistency was unknown, as there was only one study. Inconsistent results across studies was a contributing factor for a further nine gaps (8%). The wrong population was studied in six gaps (5%), inadequate duration of interventions accounted for 37 gaps (33%) and inadequate duration of follow-up contributed to 38 gaps (34%).
Factors relating to outcomes caused 35 gaps (32%). There were a number of concerns with outcomes: trials did not report outcomes the review authors deemed important; discrepancies in the type of outcomes measured in trials; variation in measurement techniques for the same outcomes. In over a third of these gaps (n=12, 34%), review authors identified issues with all three of these outcome categories.
Although most guideline gaps could not be characterised to the level of the review gaps, 11 of these novel gaps were due to no trials and four due to limited studies (38%). Many stated ‘insufficient evidence’ or ‘lack of evidence’, so it is unclear if this is due to no trials or limited number.
Discussion
We have presented a comprehensive list of the ‘known unknowns’ in treatment decisions in CF. We have identified and characterised 111 unique evidence gaps from the 73 systematic reviews that met our strict inclusion criteria. From reviewing guidelines, we found an additional 37 uncertainties. Our results show that the reasons for gaps in the evidence are multifaceted and range from no studies to reasons relating to the methodology of the underlying trials. Understanding the reasons for evidence gaps will allow us to investigate ways to plan future research to specifically address the evidence gaps.
Insufficient or imprecise information caused by no underlying trials, limited number of trials or small sample sizes was a major reason for our evidence gaps. For some gaps identified as having ‘no trials’, there are trials now in progress. An example of this is the Stop2 trial (NCT02781610), looking into duration of antibiotic treatment for exacerbations (G9, online supplementary S11). Arguably, the problem of ‘insufficient or imprecise information’ (category A above) can be addressed with a single, adequately powered trial or with a meta-analysis of several smaller trials. Gap G1 (online supplementary S11) ‘Does elective IV antibiotic therapy improve clinical status and survival in people with CF in comparison to symptomatic treatment’ could be addressed with one large trial. Unfortunately, the single large study to address this question failed to recruit its planned sample size.13 The pool of people with CF to participate in trials is relatively small and the daily regimen of treatments is onerous, making trial recruitment and retention difficult. Where the concern is around rare organisms such as non-tuberculous mycobacterium (NTM), the pool of eligible participants is even smaller. The one review that we included on NTM had no trials included.14 The same was true for Stenotrophomonas maltophilia 15 and Burkholderia cepacia. 16 17 A further reason for small numbers of participants is where one of the treatment arms is unattractive to the participant, for example home versus hospital care. The review of this topic is limited by a small number of eligible trials and small sample sizes.18
One way to overcome the problem of recruiting adequate numbers is to use a cross-over design. It can be argued that as CF is a chronic progressive disease, a cross-over design may be inappropriate.19 However, with a limited pool of patients with CF to take part in research, compromises will have to be made in order to answer the important questions. Three quarters of the trials included in our review were of a cross-over design. With increasing numbers of people with CF gaining access to CFTR modulators, it will be important to ensure that trials are designed that allow participation of patients on these medications, so that trial participants are representative of those seen routinely in clinic.20
Not all the gaps we have identified are likely to be closed through conventional clinical trials. An example is G42 ‘Can long-term inhaled corticosteroids slow decline in lung function and improve survival in people with CF?’ This gap has been partly addressed through a novel study design. The CFWISE study21 found that stopping inhaled corticosteroids does not result in earlier onset of exacerbations. A trial randomising participants to start inhaled steroids (or a comparator) is therefore unlikely. CFWISE looked at a short-term outcome measure (exacerbations). The majority of information gathered in this review came from RCTs. These are not always practical to perform, so it may be that other approaches may be more appropriate. Study designs other than RCTs (such as cohorts derived from CF registries) could provide valuable evidence of the long-term safety and effectiveness of treatment.22
Risk of bias can lead to gaps in the evidence, for example when the study design of underlying trials is inappropriate or there are major methodological limitations to the available studies. A large proportion of the studies included in a review of positive expiratory pressure physiotherapy for CF airway clearance were reported only in abstract form which meant that the risk of bias across the domains was unclear. The same review found that many of the included trials were of a cross-over design with the inherent problems of carry-over effect. So, although there were 26 included trials, the authors were still unable to provide good-quality evidence for clinicians and people with CF.23
We excluded reviews which did not state the diagnostic criteria for CF to ensure that we could be confident that findings related only to people with a confirmed CF diagnosis. An additional 13 systematic reviews could have been included in our study had the authors stated more clearly how the diagnosis of CF was made. Clear, detailed protocols, with up-to-date diagnostic criteria for both trials and systematic reviews, will prevent such data being wasted.
Outcome measures included in underlying trials accounted for 30% of missing evidence. Individual trials may measure the same outcome in different ways, making meta-analyses impossible. Outcomes widely used in trials of antimicrobials (such as resistance) show no relationship to clinical response in people with CF.24 Trials may be designed with short-term or surrogate outcomes for reasons of feasibility. Had included trials measured the same outcomes in the same way, some of the evidence gaps may have been filled. Thirty-nine of the uncertainties existed because outcomes deemed to be important to the review authors were not measured in any of the included trials. In the current era of CFTR modulator use becoming increasingly available, and with these hopefully less rapid decline in lung function, we may need to step away from FEV1 and look towards other outcome measures and in other body systems.25–28 This highlights the need for core outcomes to be identified for clinical trials in CF. A project to develop a core outcome set for CF is underway through the COMET initiative (https://www.comet-initiative.org).
There have been few previous attempts to identify evidence gaps in CF. A pilot systematic review of five CF foundation guidelines found similar reasons for treatment uncertainties, to those we have described in our review.29 This earlier review reported that no studies, or a limited number of studies, was the explanation for almost 80% of evidence gaps.
We identified evidence gaps through systematic reviews and guidelines. It follows that if no systematic review of an intervention has been done and there is no treatment guideline, we will not have identified an evidence gap in that area. The number of gaps identified in different treatment areas is not therefore indicative of the burden of treatment or the importance of disease area. Domains with few systematic reviews such as mental health interventions, end-of-life care or lung transplantation may also contain important ‘unknown unknowns’. Furthermore, where an ‘umbrella’ question has not been answered, we have not listed more detailed and specific questions as further gaps. An example of this in the area of NTM, G21 (online supplementary S11): ‘Does antibiotic treatment of NTM improve clinical outcomes in people with CF’.14 We have not identified further questions, such as particular antibiotic regimens.
We limited our searches to English publications. Only six articles were excluded on language grounds, but it is possible there are further gaps that could have been identified if these had been translated and included.
Well-designed, adequately powered studies measuring outcomes that are important to patients are needed. From 466 trials involving 23 591 people, we could demonstrate only 30 ‘known knowns’ to inform clinical practice (table 1). Many clinical trials in CF remain unpublished.30 Were this not the case, then more trials would contribute to the evidence base. It is estimated that 85% of all health-related research is wasted—through non-publication, lack of completeness of reports, unnecessary duplication or poor study design.31 Our list of evidence gaps provides a resource for CF researchers to use, to help minimise the risk of future research waste in CF.
Prior to any future studies, we recommend that investigators perform an interim review of the topic area to find trials which have been completed since the systematic review described here. Furthermore, clinical trial registries (such as ClinicalTrials.gov) should be searched for trials which are in progress. This will be particularly important in fast-moving areas such as CFTR modulators that have the potential to profoundly modify disease course.32
Presently, the direction of clinical research is guided by researchers and funders, including the pharmaceutical industry. We have identified gaps in the evidence which can be used as a resource for both researchers and funding bodies, to focus research on areas of persisting uncertainty in CF care. Trials capacity in CF has been increased through clinical trial networks in the USA33 and Europe.34 However, the number of evidence gaps still exceeds the capacity of the research community, the available funding and the number of eligible participants with CF. Therefore, prioritisation is needed. We have recently undertaken a priority-setting exercise with clinicians, patients and families through the James Lind Alliance.35 This has in turn led to a funding call by the UK National Institute for Health Research.36 These evidence gaps informed this process. We encourage researchers to co-produce research studies with the CF community in order to ensure the research questions are relevant and the study design is acceptable. This will in turn encourage patient participation and minimise research waste.37
Conclusions
We have produced an up-to-date list of treatment uncertainties in CF, and we have elaborated the reasons for these evidence gaps and made some suggestions about how these obstacles might be overcome. This information can be used by researchers and funders to ensure that future research focuses on areas where there is little or no evidence to inform treatment decisions. We believe that our results will help to influence the research agenda in CF and reduce research waste. This methodology will be suitable for other areas of respiratory disease.
Supplemental material
Supplemental material
References
Footnotes
Contributors NJR, SS, ARS and KAR contributed to the study design. Data extraction and analysis were carried out by NJR and SS with advice from ARS. APP provided the source code and produced the interactive Prayle plot. All authors were involved in the preparation of the manuscript.
Funding This work was supported by a CF Trust Venture and Innovation Award (VIA025). NJR is an NIHR academic Clinical Fellow. SS is a Cochrane Systematic Reviewer. APP is an NIHR Academic Clinical Lecturer.
Competing interests Outside the submitted work: NJR reports non-financial support from Teva. ARS reports personal fees from Vertex, PTC, Roche, TEVA and Gilead. In addition, ARS has a patent Application No. 14737297.3 (in Europe) Biomarkers for Pseudomonas aeruginosa for The University of Nottingham pending and has taken part in clinical trials sponsored by Vertex, Raptor, Insmed, Pharmaxis and Boehringer Ingelheim.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Authors plan to make data available within 1 year of publishing this article via an online repository or on reasonable application.
Linked Articles
- Airwaves