Article Text

Abstract
Background Chronic lung disease is a leading contributor to the global disease burden; however, beyond tobacco smoke, we do not fully understand what risk factors contribute to lung function decline in low-income and middle-income countries.
Methods We collected sociodemographic and clinical data in a randomly selected, age-stratified, sex-stratified and site-stratified population-based sample of 3048 adults aged ≥35 years from four resource-poor settings in Peru. We assessed baseline and annual pre-bronchodilator and post-bronchodilator lung function over 3 years. We used linear mixed-effects models to assess biological, socioeconomic and environmental risk factors associated with accelerated lung function decline.
Results Mean±SD enrolment age was 55.4±12.5 years, 49.2% were male and mean follow-up time was 2.36 (SD 0.61) years. Mean annual pre-bronchodilator FEV1 decline was 30.3 mL/year (95% CI 28.6 to 32.0) and pre-bronchodilator FVC decline was 32.2 mL/year (30.0 to 34.4). Using multivariable linear mixed-effects regression, we found that urban living, high-altitude dwelling and having hypertension accounted for 25.9% (95% CI 15.7% to 36.1%), 21.3% (11.1% to 31.5%) and 15.7% (3.7% to 26.9%) of the overall mean annual decline in pre-bronchodilator FEV1/height2, respectively. Corresponding estimates for pre-bronchodilator FVC/height2 were 42.1% (95% CI% 29.8% to 54.4%), 36.0% (23.7% to 48.2%) and 15.8% (2.6% to 28.9%) of the overall mean annual decline, respectively.
Conclusion Urbanisation, living at high altitude and hypertension were associated with accelerated lung function decline in a population with low daily smoking prevalence.
- not applicable
- copd epidemiology
- tobacco and the lung
Statistics from Altmetric.com
Key messages
What is the key question?
Beyond cigarette smoke exposure, what are the major risk factors for worsened lung function decline in low-income and middle-income settings?
What is the bottom line?
Hypertension, urban dwelling and high altitude are all independently related to greater than average annual decline in lung function.
Why read on?
Our results propose new relationships between lung function and various risk factors for disease including urbanisation, living at high altitude and cardiovascular health.
Introduction
Chronic lung disease is a leading cause of death worldwide, and accelerated decline in lung function is associated with increased hospitalisations,1 cardiovascular morbidity2 3 and all-cause mortality.1 4 5 Accelerated lung function decline is indicated by faster than average annual decrease in FEV1or FVC. In low-income and middle-income countries (LMIC), where chronic cardiovascular and respiratory diseases are the leading causes of death,6 there has been limited exploration into the understanding of accelerated lung function decline.
One of the most widely recognised risk factors for accelerated lung function decline is cigarette smoking.7 8 However, there remain variable data regarding the influence of other environmental exposures including ambient and traffic-related air pollution,9 10 and household air pollution from biomass fuel smoke exposure.11 12 It is unclear whether other risk factors including urbanisation, underlying lung disease13 and poorer cardiovascular health contribute to accelerated lung function decline in LMICs.2 12 14 Understanding the burden of environmental risk factors and comorbid medical conditions in LMIC settings can direct health systems and policy interventions geared towards disease prevention and identification of at-risk subgroups.
Previous cross-sectional analyses by our group identified risk factors associated with respiratory disease burden in our four diverse settings in Peru.15 We found that household air pollution was associated with a higher prevalence of COPD and hypertension,16 17 that urbanisation was associated with a higher prevalence of asthma18 and that both household air pollution and urbanisation were associated with a higher prevalence of chronic bronchitis.19 In this longitudinal evaluation of the CRONICAS cohort study, we aimed to determine environmental and comorbid risk factors for accelerated lung function decline. Specifically, we evaluated the effect of urbanisation, altitude, household air pollution, asthma, chronic bronchitis, history of post-treatment pulmonary tuberculosis (TB), hypertension, body mass index (BMI), systemic inflammation as measured by high-sensitivity C-reactive protein (hs-CRP) and diabetes and the relationship of each of these risk factors with longitudinal lung function.
Methods
Study setting
We conducted a longitudinal, population-based study aimed to better understand the progression towards chronic pulmonary and cardiovascular diseases across four disparate regions in Peru. The study has been described in detail elsewhere and involved collection of sociodemographic and clinical data from adults aged ≥35 years in four diverse populations in Peru.15 The four settings under study varied based on degrees of urbanisation, living at high altitude and prevalence of daily biomass fuel use (table 1). The diverse demographics of our study sites allowed us to evaluate unique environmental risk factors, specifically urbanisation, altitude and biomass fuel smoke, and comorbid conditions including hypertension, obesity, diabetes, chronic bronchitis and COPD.
Study site classification by urbanisation, indoor and outdoor pollution, and altitude
Design
We enrolled an age- (35–44, 45–54, 55–64 and ≥65 years), sex- and site-stratified sample of eligible subjects. Recruitment began in September 2010 and was conducted until approximately 1000 participants with complete information per site were enrolled. Only one participant per household was enrolled. In Puno, we stratified recruitment to include 500 participants each from the urban and rural settings. Patients were followed for a total of 3 years after their enrolment date. Inclusion criteria were being ≥35 years of age, being a full-time resident in the specified setting and capacity to understand procedures and consent to the study. Exclusion criteria were being pregnant, having a physical disability that prevented measurement of blood pressure or anthropometry, or having active pulmonary TB.
Data collection
Each participant was evaluated three times over three years. At enrolment, participants responded to a questionnaire on sociodemographics, smoking history, respiratory symptoms, medical history and family history of disease. A detailed questionnaire also evaluated frequency and duration of cooking with biomass fuels. Spirometry was conducted annually for a total of three tests per participant using the Easy-On-PC spirometer (ndd, Zurich, Switzerland). Pre-bronchodilator examinations were conducted on all three visits, whereas post-bronchodilator examinations using 200 μg of inhaled salbutamol via a spacer were conducted in the first and third visits only. Trained technicians measured spirometry in participants following joint American Thoracic Society and European Respiratory Society guidelines.20 We adapted a standardised grading system for quality control, review and interpretation.21 Participants with low-quality spirometry were asked to repeat the test on another day for a total of three attempts. Blood samples were collected in the first and third visits.
Definitions
To assess lung function decline, we looked at subject-specific change in pre-bronchodilator FEV1/height2, FVC/height2 and FEV1/FVC over time.22 All results are presented as mL/m2 or per cent difference from mean baseline values. FEV1/height2 was calculated by dividing FEVs (in millilitres) by height (in metres) squared. We also presented results as lung volumes adjusted by height and Z-scores for sensitivity analysis. All of the following risk factors for lung function decline were assessed using baseline clinical data from visit one. We defined chronic bronchitis as having self-reported phlegm production for at least three months each year in two successive years. We created a wealth index according to assets, household facilities, household income and occupation.23 We defined biomass fuel use as using biomass fuels for cooking at least once daily. We defined daily smoking as having at least one cigarette a day; hypertension as having systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, self-report of a physician diagnosis or current use of antihypertensive medications; diabetes as a fasting glucose ≥126 mg/dL, self-report of physician diagnosis or current use of antihyperglycaemic medications; and TB as self-reported medical history of treated pulmonary TB (ie, post-treatment pulmonary TB). Urban or rural dwelling was defined according to site. Lima and urban Puno were classified as urban, whereas Tumbes and rural Puno were classified as rural based on city density and traffic (table 1). Rural and urban Puno were considered high-altitude sites, whereas Lima and Tumbes were considered sea-level communities.
Biostatistical methods
We sought to characterise average lung function decline in our study populations and identify potential factors that were associated with an accelerated decline. As such, we used multivariable linear mixed-effects models with random intercepts and random slopes by individual to assess the potential factors associated with longitudinal lung function values. The use of random effects in longitudinal data analysis accounts for the heterogeneity in subject-specific lung function values at baseline (intercept) and change over time (slope). All models were adjusted for the following a priori selected baseline factors: age, sex, height, environmental exposures (self-reported smoking, self-reported daily biomass fuel use, urbanisation, living at high altitude, wealth index), comorbid conditions (hypertension, diabetes, chronic bronchitis, asthma, history of post-treatment pulmonary TB), BMI and hs-CRP. In place of adjusting for site, we decomposed site into multiple components including degree of urbanisation and altitude. For continuous variables such as BMI and hs-CRP, we scaled the effect size to the IQR, that is, the difference between the 75th and 25th percentiles of these variables. We then conducted sex-specific subset analyses of above models. Attributable annual decline in lung function (as a percentage) for each risk factor were calculated as the estimated change in lung function for that specific factor divided by the average annual decline in lung function in the population, multiplied by 100 (eg, an expected decline of 6 mL for a risk factor modelled in our regression with regard to the observed average 30 mL annual decline in pre-bronchodilator FEV1 corresponds to a 20% decline above expected). We used local polynomial regression to estimate the smoothed mean and 95% CI for values in figure 1.24 Analyses were conducted in R (www.r-project.org) and linear mixed effects models used the package lme4.

Histogram of annual declines in mL/year for pre-bronchodilator FEV1 (left panel) and FVC (right panel) for all study participants, expressed as a proportion of the total number of participants. All values were calculated using the 2793 (90.0%) participants with at least one follow-up visit.
Results
Participant characteristics
A total of 3048 people completed at least one spirometry testing in any of the three visits and 2956 (97%) participants of these had complete data on all other variables included in the longitudinal models. Of the 2956 participants with complete data, 2180 (72.2%) had spirometry measurements in all three visits, 537 (17.6%) had spirometry measurements on two visits and 309 (10.1%) had a spirometry measurement at just one visit. Non-participation in subsequent data collection was due to death, participant declining further testing or questioning or incomplete data collection. There were no differences in sex (p=0.56), having COPD (p=0.86) or age (p=0.12) between participants who were included in analysis compared with those who were not; however, participants included higher BMI (p=0.05) than those who were not.
Among the 3048 participants with spirometry, average age at enrolment was 55.4±12.5 years and 49.2% were male. The four sites were heterogeneous with respect to BMI, wealth index, cigarette and biomass fuel exposures, clinical history and data, and lung function (table 2). Tumbes and Lima (sea-level settings) had higher average BMI and hs-CRP, and higher prevalence of hypertension. Lima, the urban sea-level population with high outdoor air pollution, had the highest prevalence of post-treatment pulmonary TB , asthma and chronic bronchitis. Urban and rural Puno (high-altitude settings) also had high prevalence of chronic bronchitis, but rural Puno, when biomass fuel is predominantly used, there is a marked increased prevalence of COPD compared with all other study sites. Prevalence of daily cigarette smoking was highest in Lima, but overall it was relatively low across all settings (table 2).
Demographic, clinical and lung function characteristics stratified by site
Overview of lung function decline
Average annual decline in pre-bronchodilator FEV1 and FEV1/height2 was 30.3 mL (95% CI 28.6 to 32.0 mL) and 10.8 mL/m2 (10.3 to 11.4 mL/m2) per year, respectively (table 2 and figure 1). Lima and rural Puno had similar FEV1 annual decline whereas urban Puno had the fastest and Tumbes had the lowest annual decline (table 2). Mean annual decline in pre-bronchodilator FVC and FVC/height2 was 32.2 mL (30.0 to 34.4 mL) and 11.4 mL/m2 (10.3 to 11.4 mL/m2) per year, respectively. Compared with participants who were at sea level, those who lived at high altitude had a faster decline in lung function (table 2). There was substantial heterogeneity in annual decline of both pre-bronchodilator FEV1 and FVC across participants (figure 1). Moreover, adults with higher pre-bronchodilator FEVs at baseline also had a faster annual decline in their lung function (figure 2).
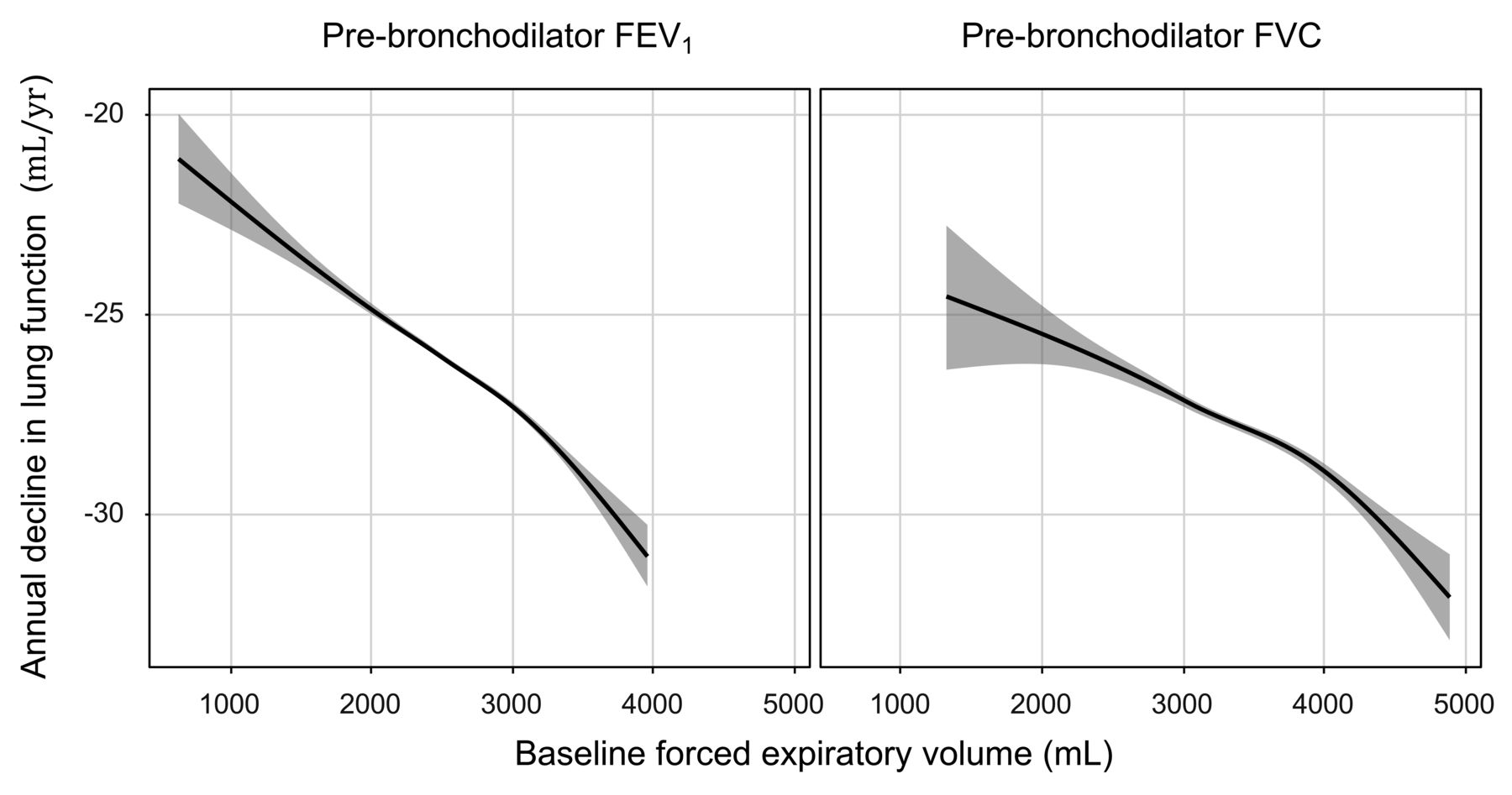
Annual decline in pre-bronchodilator FEV1 (left panel) and FVC (right panel) as a function of the corresponding baseline FEV. Smooth lines (in blue) and 95% confidence bands (grey area) were obtained using local polynomial regression adjusted for age, sex, wealth index, diabetes, asthma, history of post-treatment pulmonary TB and high-sensitivity C-reactive protein levels, daily smoking, daily biomass fuel exposure, having hypertension at baseline, chronic bronchitis, body mass index IQR, urbanisation and high altitude.
Factors that may affect lung function decline
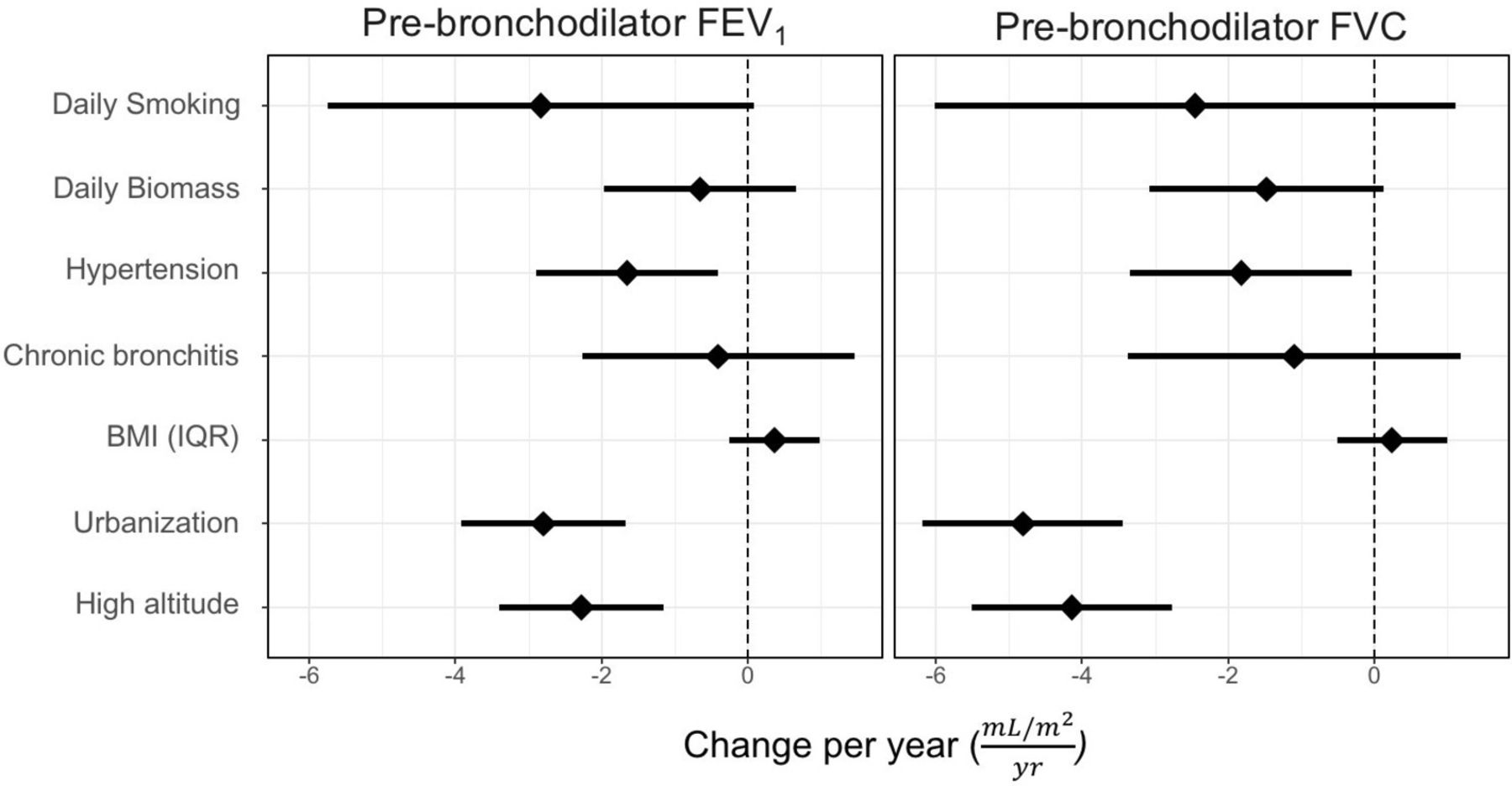
We found varying trends between risk factors when looking at lung function decline with age (figure 3). Urbanisation, high altitude and hypertension were responsible for an additional 2.8 mL/m2 (95% CI 1.7 to 3.9 mL/m2), 2.3 mL/m2 (1.2 to 3.4 mL/m2) and 1.7 mL/m2 (0.4 to 2.9 mL/m2) decrease in overall average annual decline in FEV1/height2, respectively. This corresponds to an additional 25.9% (95% CI 15.7% to 36.1%), 21.3% (11.1% to 31.5%) and 15.7% (3.7% to 26.9%) higher than average annual decline in FEV1/height2, respectively (table 3). When looking at FVC/height2, we found that urbanisation, high altitude and hypertension were responsible for an additional 4.8 mL/m2 (95% CI 3.4 to 6.2 mL/m2), 4.1 mL/m2 (2.7 to 5.5 mL/m2) and 1.8 mL/m2 (0.3 to 3.3 mL/m2), respectively (table 3). This corresponds to an additional 42.1% (95% CI 29.8% to 54.4%), 36.0% (23.7% to 48.2%) and 15.8% (2.6% to 28.9%) higher than average annual decline for urbanisation, high altitude and hypertension, respectively. Daily smokers trended towards having higher annual declines in pre-bronchodilator FEV1 (p=0.06) and FVC (p=0.18). Daily biomass fuel smoke exposure was not associated with a higher than average annual decline in pre-bronchodilator FEV1/height2 (p=0.33), but there was a trend towards a higher average annual decline in FVC/height2 (p=0.08). Urbanisation and high altitude were associated with slower annual decline in pre-bronchodilator FEV1/FVC ratio of 0.07 (0.02 to 0.11) and 0.05 (0.01 to 0.10), respectively. A history of post-treatment pulmonary TB was the only factor associated with a higher annual decline in pre-bronchodilator FEV1/FVC (−0.10, 95% CI −0.20 to −0.01).
Unadjusted and adjusted mean effect of covariates on pre-bronchodilator FEV1/height2 and FVC/height2 over time (mL/m2 per year)

Adjusted mean annual decline in pre-bronchodilator FEV1/height2 (left panel) and FVC/height2 (right panel) as a function of daily smoking (non-smoker or non-daily smoker is reference), daily biomass fuel exposure (no exposure or non-daily is reference), having hypertension at baseline, chronic bronchitis, body mass index (BMI) IQR (difference between 75th and 25th percentile), urbanisation and high altitude. The diamonds represent adjusted mean differences in lung function decline and horizontal lines represent the corresponding 95% CIs. Adjusted means were obtained from regression models that included age, sex, wealth index, diabetes, asthma, history of post-treatment pulmonary TB, high-sensitivity C-reactive protein levels, daily smoking, daily biomass exposure, living at high altitude and urbanisation.
Sensitivity analysis
We performed sensitivity analysis with Z-scores and absolute FEV1 and FVC values and found effect sizes were similar (figures 4 and 5, and table 3). To evaluate the effects of underlying lung disease on lung function decline, we performed a sensitivity analysis using the same regression model but excluding those with COPD. We found similar mean estimates and 95% CIs (online supplementary E-Table 1 and 2).
Supplementary file 1

Adjusted mean annual decline in pre-bronchodilator FEV1 (left panel) and FVC (right panel) Z-scores as a function of daily smoking (non-smoker or non-daily smoker is reference), daily biomass fuel exposure (no exposure or non-daily is reference), having hypertension at baseline, chronic bronchitis, body mass index (BMI) IQR (difference between 75th and 25th percentile), urbanisation and high altitude. The diamonds represent adjusted mean differences in lung function decline and horizontal lines represent the corresponding 95% CIs. Adjusted means were obtained from regression models that included age, sex, wealth index, diabetes, asthma, history of post-treatment pulmonary TB, high-sensitivity C-reactive protein levels, daily smoking, daily biomass exposure, living at high altitude and urbanisation. Z-scores were calculated using National Health and Nutrition Examination Survey Mexican-American reference equations.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted mean annual decline in pre-bronchodilator FEV1 (left panel) and FVC (right panel) as a function of daily smoking (non-smoker or non-daily smoker is reference), daily biomass fuel exposure (no exposure or non-daily is reference), having hypertension at baseline, chronic bronchitis, body mass index (BMI) IQR (difference between 75th and 25th percentile), urbanisation and high altitude. The diamonds represent adjusted mean differences in lung function decline and horizontal lines represent the corresponding 95% CIs. Adjusted means were obtained from regression models that included age, sex, wealth index, diabetes, asthma, history of post-treatment pulmonary TB, high-sensitivity C-reactive protein levels, height, daily smoking, daily biomass exposure, living at high altitude and urbanisation.
Discussion
In this multicentre, population-based longitudinal study of adults in Peru, we found that living at high altitude and living in an urban setting was associated with accelerated lung function decline. Smoking trended towards having accelerated decline in lung function in our population, but may have not achieved statistical significance because of the low prevalence of daily smokers. Biomass fuel smoke exposure also trended towards having accelerated decline in FVC/height2. Having hypertension at baseline was associated with an accelerated decline in both FEV1/height2 and FVC/height2 in our study population. In contrast, other comorbid conditions including obesity, diabetes and chronic bronchitis did not show accelerated lung function decline.
Several findings reported in our study are consistent with existing literature from high-income countries and provide novel reports of longitudinal lung function in LMICs. Average FEV1 decline in our study was 30.3 mL/year; similar to the 33±2 mL/year observed by the ECLIPSE investigators,25 the 27 mL/year observed in a non-smoking population in the Lung Health Study26 and within the age-related decline of 23.7–39 mL/year for adults aged 25–75 years found across multiple US cities.27 The mean rate of FVC decline in our study was 32.5 mL/year, which is also within the range of the National Health and Nutrition Examination Survey age-related predictions.25
There is a paucity of research evaluating lung function decline in LMICs, and the majority of these existing studies focus on biomass fuel smoke exposure. A study in Mexico that followed participants with COPD for 15 years found a lower rate of FEV1 decline (23 mL/year) in their biomass-exposed group compared with the decline observed in our rural Puno group (33.5 mL/year), a setting where biomass fuels are used for cooking on daily basis in approximately 95% of study households.16 A prospective cohort study in China found a similar FEV1 decline of 35 mL/year in participants who used biomass fuels for cooking compared with a much slower decline of 18 mL/year among participants using alternative clean fuels and improved ventilation.12 Other groups have seen associations between biomass fuel and decline in FVC.28 Proposed mechanisms for accelerated decline in FVC involve the development of scarring and interstitial lung abnormalities in the setting of biomass fuel exposure.28 Our study did not show a significant relationship between biomass fuel and FEV1 or FEV1/FVC ratio. Biomass fuel exposure trended towards an accelerated decline in FVC; however, this trend did not achieve statistical significance at the 0.05 level. These discrepancies could be attributed to either shorter follow-up time or the complexity of multiple other environmental and comorbid risk factors found in our cohort that can also contribute to lung function decline. Our findings are similar to the RESPIRE cookstove intervention trial which had a slightly longer follow-up period than our study (5.6 years).11 Furthermore, similar to what we found with cigarette smoke and traffic related air pollution, any effects of biomass on lung function decline may be diminished by the fact that only certain groups are susceptible to such environmental influences.29–31 Gene by environment interactions related to household air pollution need further exploration.
Other environmental exposures highlighted in our study included the effects of high altitude and urbanisation on accelerated lung function decline. At high altitude, hypoxia and inflammation likely play a role in lung function decline.32 33 Hypoxia itself induces systemic inflammation by activating hypoxia-inducible factor 1-alpha in hypertrophied obese adipose tissues.34 35 Higher inflammation has been associated with worse outcomes in COPD populations. In highly urbanised settings, outdoor air pollution and comorbid conditions likely play a role in lung function decline.9 14 Cross-sectional evaluation from the ESCAPE study found that an increase in NO2 exposure was associated with lower baseline FEV1 and FVC,10 whereas work by Rice et al found an association with long-term exposure to traffic and PM2.5.9 However, other studies have found no significant association between ambient PM2.5 levels and lung function decline.36
What causes environmental factors to influence disease in one individual but not in another remains unclear. There has been significant discussion regarding genetic predisposition to COPD leading some, but not all, daily cigarette smokers to develop pulmonary disease. It is likely that indoor air pollution from biomass fuels, outdoor air pollution and other environmental exposure similarly affect predisposed individuals.37 Given the variable effects of exposures on lung function, to develop targeted interventions, it is important to find clinical and biological identifiers for at-risk individuals among high-exposure populations. In this study, we took a novel approach and simultaneously evaluated effects of both environmental and comorbid conditions on lung function decline. Hypertension has been associated with pulmonary disease in previous work from both NHANES III and BOLD.3 38 Similarly, the BOLD study,38 the Whitehall II study39 and the MESA study have reported an association with lower baseline FVC and markers of cardiovascular disease including arterial stiffness and hypertension.40 Going beyond a cross-sectional association, the CARDIA study looked at this same question from a different angle and demonstrated accelerated decline in FEV1 and FVC predicted future incident of hypertension in an otherwise generally healthy population.2 One proposed mechanism connecting cardiovascular disease and lung function is a parallel physiological degradation pathway of arterial and airway elasticity. The MESA study observed a positive association between small arterial elasticity and lung function.40 A second hypothesis proposes systemic endothelial dysfunction mediates the association between FEV1 and atherosclerosis; however, in a recent study, airflow limitation and endothelial dysfunction were found to be unrelated and independent predictors of atherosclerosis.41 Finally, a third related hypothesis poses that systemic inflammation related to lung disease facilities a prothrombotic state and augments atherosclerosis.
Our study has several strengths. First, this is one of few longitudinal studies evaluating lung function decline in LMICs. Second, we collected detailed demographic, clinical and environmental data that allows us to explore competing factors contributing to lung function decline. Third, the low prevalence of tobacco smoking provides a unique opportunity to examine other risk factors contributing to lung function decline. Finally, we used longitudinal analysis methods that model subject specific trajectories.42 43 A specific concern was how to account for baseline lung function in our analyses. To address this concern, we accounted for heterogeneity in subject-specific baseline lung function through the use of random intercepts. This allowed us to evaluate population-averaged trends while accounting for the heterogeneity (ie, variation) in baseline FEVs among individuals.
Our study also has some potential limitations. First, we were not powered to determine risk factors stratified by site; however, we are able to evaluate key components of each site including altitude and urbanisation. Second, because of the number of risk factors evaluated in our analysis, it is possible that we were not powered to measure the effects of competing conditions such as diabetes,44 and chronic bronchitis which have been previously described.45 Third, our follow-up time is only a short to intermediate time frame with respect to decline in FEV1 and FVC and therefore we may not see the significant effects from some risk factors that one might expect like chronic bronchitis. Finally, some of our clinical data including asthma, chronic bronchitis and history of post-treatment pulmonary TB are self-reported and therefore potentially subject to bias and error.
Conclusion
In four diverse settings in Peru with low tobacco use prevalence, we found that urbanisation, high altitude and hypertension were associated with accelerated decline in FEVs. This study highlights possible environmental and comorbid factors that contribute to accelerated lung function decline in LMICs.
References
Footnotes
Contributors CHM, MRG and WC were responsible for conducting analysis. JJM, AB-O, RHG and WC were responsible for study design and conduct. CHM, MRG, TS and WC were responsible for the first draft of the manuscript. CHM, MRG, TS, RHG, JJM, AB-O, RAW and WC participated in the interpretation of findings and development of conclusions. WC is ultimately responsible for the integrity of analyses and quality of data.
Funding This project was funded in whole with federal funds from the United States National Heart, Lung, and Blood Institute, National Institutes of Health, Department of Health and Human Services, under Contract No. HHSN268200900033C. Research reported in this publication was supported by the National Heart, Lung, and Blood Institute of the United States National Institutes of Health under Award Number T32HL007534. CHM was further supported by a Fogarty International Center training grant (5R25TW009340).
Competing interests None declared.
Patient consent Not required.
Ethics approval Johns Hopkins Bloomberg School of Public Health, Universidad Peruana Cayetano Heredia and A.B. PRISMA.
Provenance and peer review Not commissioned; internally peer reviewed.
Collaborators Cardiovascular Disease: Antonio Bernabé-Ortiz, Juan P. Casas, George Davey Smith, Shah Ebrahim, Robert H. Gilman, Luis Huicho, Germán Málaga, J. Jaime Miranda, Víctor M. Montori, Liam Smeeth; Chronic Pulmonary Disease: William Checkley, Gregory B. Diette, Robert H. Gilman, Luis Huicho, Fabiola León-Velarde, María Rivera, Robert A. Wise; Training and Capacity Building: William Checkley, Robert H. Gilman, J. Jaime Miranda, Katherine Sacksteder.