Article Text

Statistics from Altmetric.com
Case report
A 38-year-old previously fit smoker of 10 pack-years presented with 1 month of progressive worsening exertional dyspnoea. He had no cough, chest pain nor constitutional symptoms. Auscultation of the chest revealed widespread crepitations. Oxygen saturation was 96% on room air, desaturating to 88% after mild exertion. Chest radiograph showed diffuse nodular interstitial infiltrates with significant peribronchial cuffing. CT thorax revealed multiple Cheerio signs of varying sizes and wall thickness, distributed evenly bilaterally (figure 1). There was significant interlobular septal thickening with thickened peribronchovascular bundles, and a thick-walled cavitation in the left lower lobe. Flexible bronchoscopy was performed under fluoroscopy via endotracheal tube. Radial endobronchial ultrasound (R-EBUS) examination at all visible subsegmental branches of the lateral segment of the right lower lobe demonstrated multiple scattered hyperechoic linear arcs and dots, representing patent airspaces (figure 2A,B, arrow). Transbronchial lung cryobiopsy was performed uneventfully at the site of the R-EBUS examination. Histopathological examination revealed invasive lung adenocarcinoma with predominantly micropapillary and glandular growth patterns (figure 2C,D). Epidermal growth factor receptor mutation with exon 19 deletion was detected.
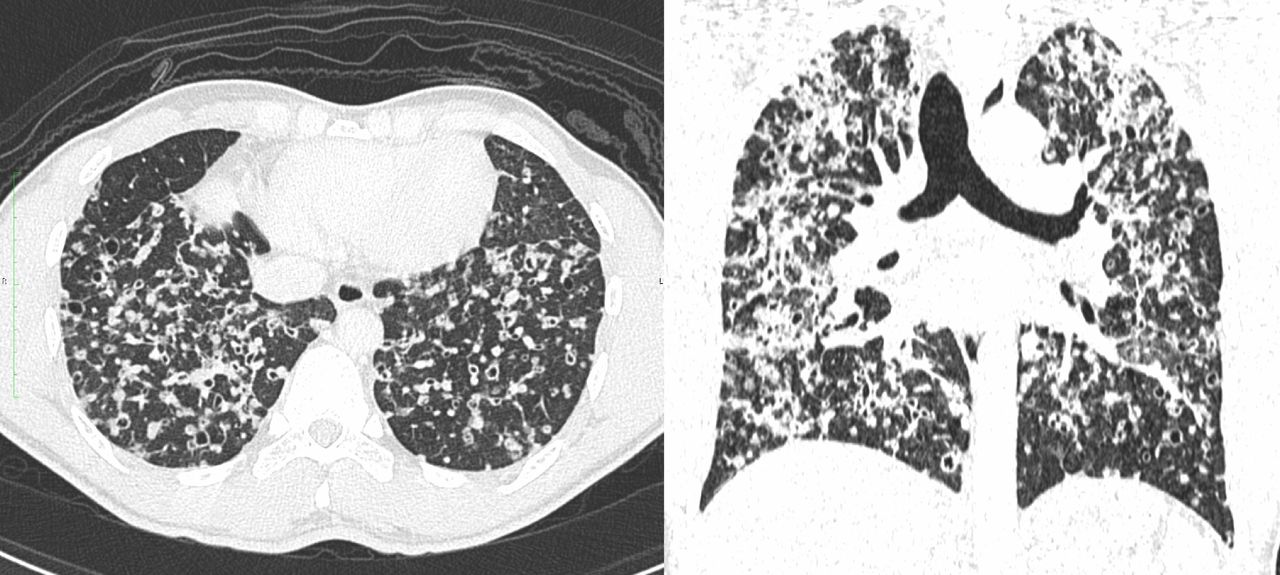
Cheerio sign: multiple diffuse nodules with central lucency of varying sizes and wall thickness distributing evenly in both lung fields.

{kind=link}
{kind=link}
Representative radial endobronchial ultrasound (R-EBUS) and histopathological images. (A,B) Representative R-EBUS images demonstrating multiple hyperechoic linear arcs and dots of adjacent patent airspaces (arrow). (C) Adenocarcinoma lung demonstrating glandular pattern with possible lepidic component giving rise to various intact airspaces. (D) Adenocarcinoma lung demonstrating micropapillary growth pattern with malignant infiltrated airspaces (arrow) kept patent by surrounding desmoplastic reaction.
Discussion
The Cheerio sign was defined as the CT finding of a nodule with a hypodense centre, resembling the ring-shaped Cheerios breakfast cereal.1 Pathologically, it is caused by peribronchiolar cellular proliferation around a patent airway.2 Common causes for Cheerio sign include pulmonary Langerhans cell histiocytosis, lung adenocarcinoma, and occasionally cavitary lesions of the lung, such as fungal infections, metastatic lung cancers, lymphoma, rheumatoid nodules and granulomatosis with polyangiitis.
Cheerio sign is a rare radiographic sign, and adenocarcinoma presenting with multiple Cheerio signs, as reported in our case, is even rarer.2 It is commonly associated with invasive lepidic-predominant adenocarcinoma, as alveolar structures and bronchial patency are usually maintained in this cancer subtype.1 Although our biopsied specimen did not demonstrate a predominating lepidic component, figure 2C shows a glandular growth pattern with possible lepidic component giving rise to multiple intact airspaces. But more prominently, figure 2D shows a predominant micropapillary growth pattern with infiltrated airspaces kept patent by surrounding desmoplastic reaction. Thus, interestingly, this case demonstrates that growth patterns other than lepidic infiltration may also give rise to the Cheerio sign.
To the best of our knowledge, the usage of R-EBUS in evaluating Cheerio sign had not been described previously. R-EBUS allows visualisation of the internal structure of peripheral pulmonary lesions, such as the hyperechoic linear arcs and dots produced by air in patent alveoli and bronchioles.3 R-EBUS examination in our patient revealed these same-said multiple scattered hyperechoic linear arcs and dots, correlating with the patent airspaces seen in the CT full of Cheerios, as well as the histology of multiple intact airspaces. Kurimoto et al 3 have demonstrated the ability of R-EBUS imaging to predict malignant histology by examining the morphology of hyperechoic areas and focusing on internal echoes, vascular and bronchial patency. In the study, lesions that demonstrated hyperechoic dots and linear arcs were proven to be malignant in all cases, with 91.6% adenocarcinoma, which was consistent with our case.3
Transbronchial lung cryobiopsy is an effective tool for the diagnosis of diffuse parenchymal lung disease with a better safety profile than surgical biopsy.4 Cryobiopsy safety could be further improved with R-EBUS visualisation and avoidance of major blood vessels.5 This case highlights the rare manifestation of lung adenocarcinoma as multiple Cheerio signs, with an added perspective of its appearance from the viewpoint of R-EBUS.
Acknowledgments
We thank our colleagues Dr Nur Shazwaniza Binti Awang Basry and Dr Yusri Bin Yusuf from the Department of Pathology, Sarawak General Hospital, for preparing and analysing the histology specimens and comments that greatly improved the manuscript.
Footnotes
Contributors SSK initiated the idea for case reporting and prepared the final copy of the manuscript. MCY is the first assistant of the bronchoscopic procedure and SKC was involved in the overall patient management. STT performed the transbronchial lung cryobiopsy and supervised and reviewed the final manuscript. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves