Article Text

Statistics from Altmetric.com
A previously fit and well 43-year-old man presented with 8 weeks of worsening breathlessness and a dry cough. He was an ex-smoker of 10 pack-years with no history of asbestos exposure, thoracic radiation or recent trauma.
Chest radiograph and CT thorax are shown in figure 1. Pleural aspiration was undertaken and 1.5 L of blood-stained fluid was removed, with symptomatic improvement. The fluid was exudative, with lactose dehydrogenase (LDH) 437U/L (serum 374U/L) and protein 47g/L (serum 77g/L). Infection was excluded by negative microbiological culture and normal inflammatory markers. Cytology revealed numerous red blood cells, scattered lymphocytes and eosinophils, but no malignant cells.

(A) Posterior–anterior chest radiograph showing moderate left-sided pleural effusion and an indistinct opacity at the left hilum with mediastinal shift to the right. (B) Coronal CT images showing a round, encapsulated extrapulmonary mass, with cystic areas within in, surrounded by a pleural effusion. (C) Coronal positron emission tomography-CT images demonstrating high SUV uptake within the mass (maximum 6.6) and physiological uptake in the liver and kidneys. (D) The tumour, visualised at thoracotomy. A large cyst is seen on the tumour surface. Further cysts were seen elsewhere, some of which appeared to have ruptured.
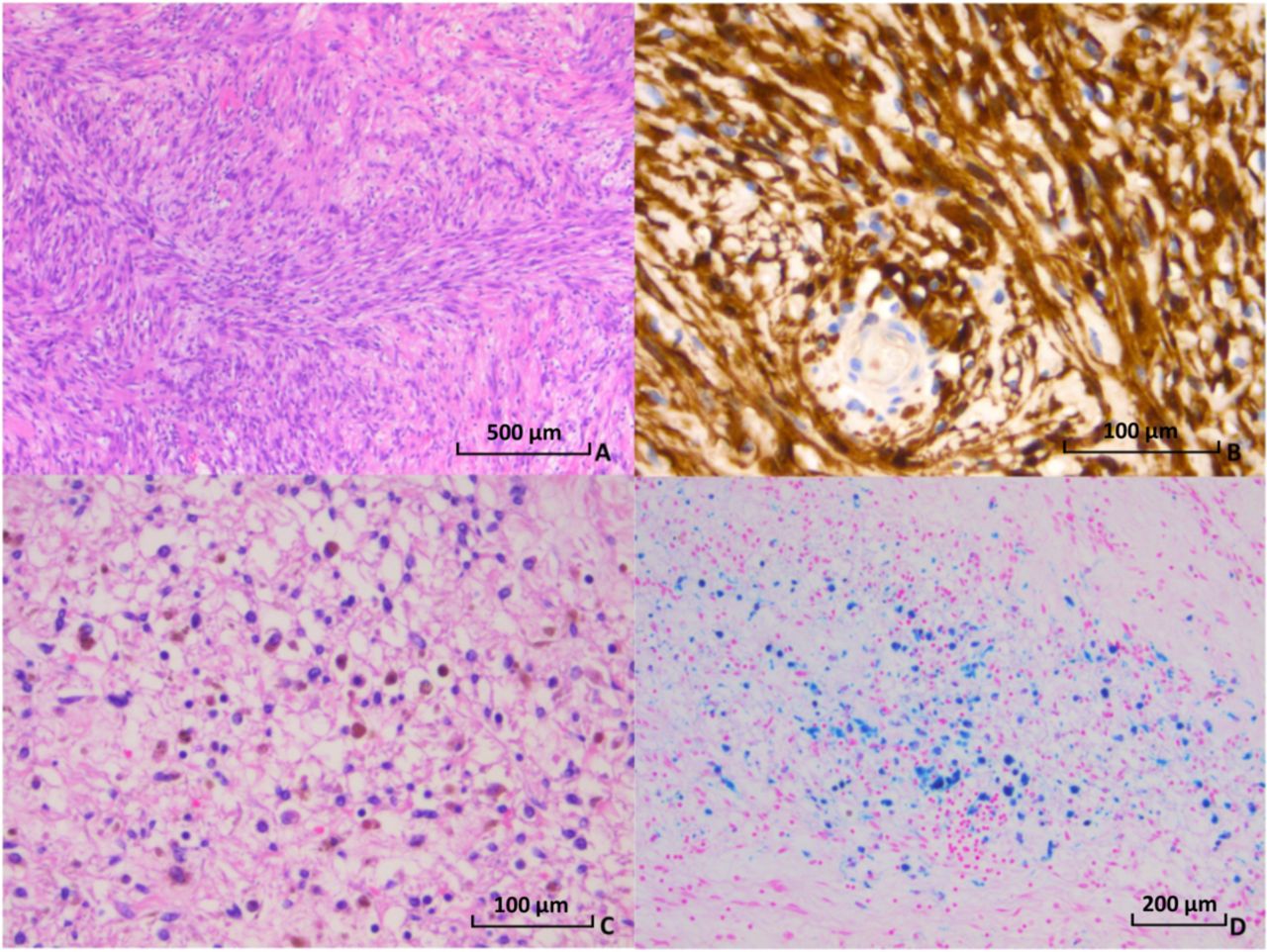
The patient underwent ultrasound-guided core biopsy, which revealed a spindle-cell neoplasm with positive immunohistochemical staining for vimentin and AE1/AE3, and S100 positivity in many nuclei (figure 2). Haemosiderin pigmentation was noted (figure 2). The features were consistent with a low-grade nerve sheath tumour, specifically schwannoma.
Positron emission tomography CT (PET-CT) was undertaken to assess for metastatic disease (figure 1). This confirmed a left paraspinal mass with heterogeneous standardised uptake value (SUV) avidity (maximum 6.6) and a moderately avid internal mammary chain lymph node (maximum SUV 3.0).
{kind=link}
{kind=link}
(A) Microscopic appearance of H&E stained resected tumour showing a moderately cellular spindle-cell neoplasm characterised by variably orientated cells, which in places appear to be arranged in swathes. Cells show a mild degree of variation in nuclear hyperchromasia, mild nuclear pleomorphism and mild anisonucleosis. (B) High-powered image of S100 stain showing diffuse positivity throughout the tumour. (C) Focal haemosiderosis visible as brown deposits on standard H&E stain. (D) Perls’ stained section of tumour demonstrating areas of blue-staining iron deposition, consistent with haemosiderin.
He underwent left-sided single-port video-assisted thoracic surgery to exclude pleural malignancy. The procedure was converted to thoracotomy to allow complete resection of tumour. Macroscopically, the tumour was a heterogeneous, lobulated mass, measuring 105×111×98 mm and encapsulated by a thin fibrous layer (figure 1). Cysts were visible on the surface of the tumour, some of which appeared defective or ruptured. The histological features and immunohistochemical profile confirmed schwannoma, with no evidence of malignancy. The mass was completely excised (R0). The faintly PET-avid lymph nodes were also removed and were benign.
The patient had an uneventful recovery and was discharged 4 days postoperatively. He was asymptomatic when reviewed 3 months later.
Schwannomas are rare tumours arising from Schwann cells—specialised myelin-producing cells of peripheral nerve sheaths.1 They represent 1%–2% of thoracic tumours, usually occurring in the third or fourth decade, with an equal sex distribution.1 Schwannomas are typically benign, slow-growing and asymptomatic and are often diagnosed incidentally. Malignant schwannomas exist, but are significantly rarer, occurring at a ratio of 1:11 compared with benign schwannomas.2
Although malignant schwannomas frequently present with pleural effusions caused by invasion of local structures, effusions are uncommon in benign schwannomas.2 In a recent series of 49 cases, only 1 presented with an effusion.3 Review of the literature revealed just four cases of benign schwannomas with pleural effusion since 1946 (see online supplementary appendix A) In all cases, the effusion was blood-stained. Combined with the frequent histological finding of haemosiderin, this suggests spontaneous tumour haemorrhage as the possible aetiology of effusions. The appearance of the tumour in this case suggests cyst rupture also plays a role in the development of pleural effusions.
Supplementary file 1
An alternative explanation would be chronic pleural irritation by the tumour, causing fluid build-up and intermittent bleeding from capillary beds. This may explain the enlarged mammary chain lymph node seen in this case.
This case confirms that benign nerve sheath tumours such as schwannomas can present with pleural effusions. Effusions may be large and blood-stained, and malignancy should not be assumed on the basis of these factors.
Footnotes
Contributors ACB, EI and NAM conceived the idea for the article. AJE provided the radiology images and wrote the corresponding text. EI supplied the photo in figure 2 and wrote the text regarding the surgical procedure. RD supplied the histological pictures and wrote the corresponding text. ACB wrote the rest of the article, with input and guidance from NAM. All authors reviewed and approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.