Article Text

Abstract
Telomere shortening is associated with COPD and impaired lung function in cross-sectional studies, but there is no longitudinal study. We used data from 448 participants recruited as part of the French follow-up of the European Community Respiratory Health Survey. We found no relationship between telomere length at baseline and FEV1 decline after 11 years of follow-up. However, heavy smoking was associated with an accelerated FEV1 decline in individuals with short telomeres, but not in subjects with longer telomeres (p for interaction p=0.08). Our findings suggest that short telomere length in peripheral leucocytes might be a marker for increased susceptibility to the effect of smoking.
- Tobacco and the lung
- COPD epidemiology
Statistics from Altmetric.com
Introduction
Not all smokers will develop COPD but the reasons why some individuals are more susceptible to accelerated loss of lung function when exposed to tobacco smoke are still largely unexplained. Telomeres are structures at the chromosomal ends involved in chromosomal stability. Patients with COPD have been shown to have shorter telomeres compared with healthy smokers, and correlations between telomere shortening, premature senescence and lung inflammation have been reported.1–6 Experimental studies show that telomere dysfunction may result in replicative senescence and release of proinflammatory mediators,4 7 leading to hypotheses that telomere shortening might contribute and maintain the inflammatory process causing airway remodelling and COPD. Consistent with this, mice with short telomeres secondary to knocking down telomerase hTR-/- were more likely to develop emphysema after cigarette smoke exposure than wild type controls.5 Altogether, these data suggest that individuals with short telomere might be at increased risk of accelerated lung function decline when exposed to smoking. Telomere shortening has been associated with impaired lung function in cross-sectional studies of patients with COPD and in cross-sectional analyses of large population-based samples.2 8 9 We are unaware of any longitudinal study that has examined this.
Using information from 448 middle-aged adults randomly selected from the general population and followed up as part of the European Community Respiratory Health Survey (ECRHS) in three French centres,10 we assessed whether lung function decline after 11 years of follow-up was associated with telomere length at baseline (2000–2002), and whether the effect of smoking was modified by telomere length. Relative telomere length in peripheral leucocytes was measured by quantitative PCR (details in the online repository), and categorised into tertiles. The methods for ECRHS, statistical analysis, and participants’ characteristics are described in the online supplementary material.
Results
Cross-sectional analysis at baseline
At baseline, relative telomere length was negatively associated with age, but was not associated with sex, pack-years smoked, body mass index (BMI), physical activity, atopic sensitisation, asthma or other respiratory symptoms or comorbidities (see online supplementary table E1). There was no relationship between telomere length and FEV% or FVC%predicted. The percentage of subjects with prebronchodilator (BD) FEV1/FVC <lower limit of normal (LLN) at baseline was quite low (18/444) and did not vary with telomere length (see online supplementary table E2).
Telomere length at baseline and lung function at follow-up
Participants with short and long telomeres showed similar patterns of smoking and BMI change over the follow-up (see online supplementary table E1). At follow-up, there was a non-significant increased risk of pre-BD FEV1/FVC <LLN in individuals with telomere in the first tertile (short telomeres) as compared with those in the third tertile (see online supplementary table E2), (OR adjusted for age, sex, centre, BMI, physical activity and smoking status: 2.18 95% CI 0.85 to 5.57, p=0.10). When considering post-BD spirometry (only performed at follow-up), the percentage of subjects with fixed airflow obstruction was low (n=17/404) and did not vary with telomere length.
Lung function decline by smoking and tertiles of telomere length
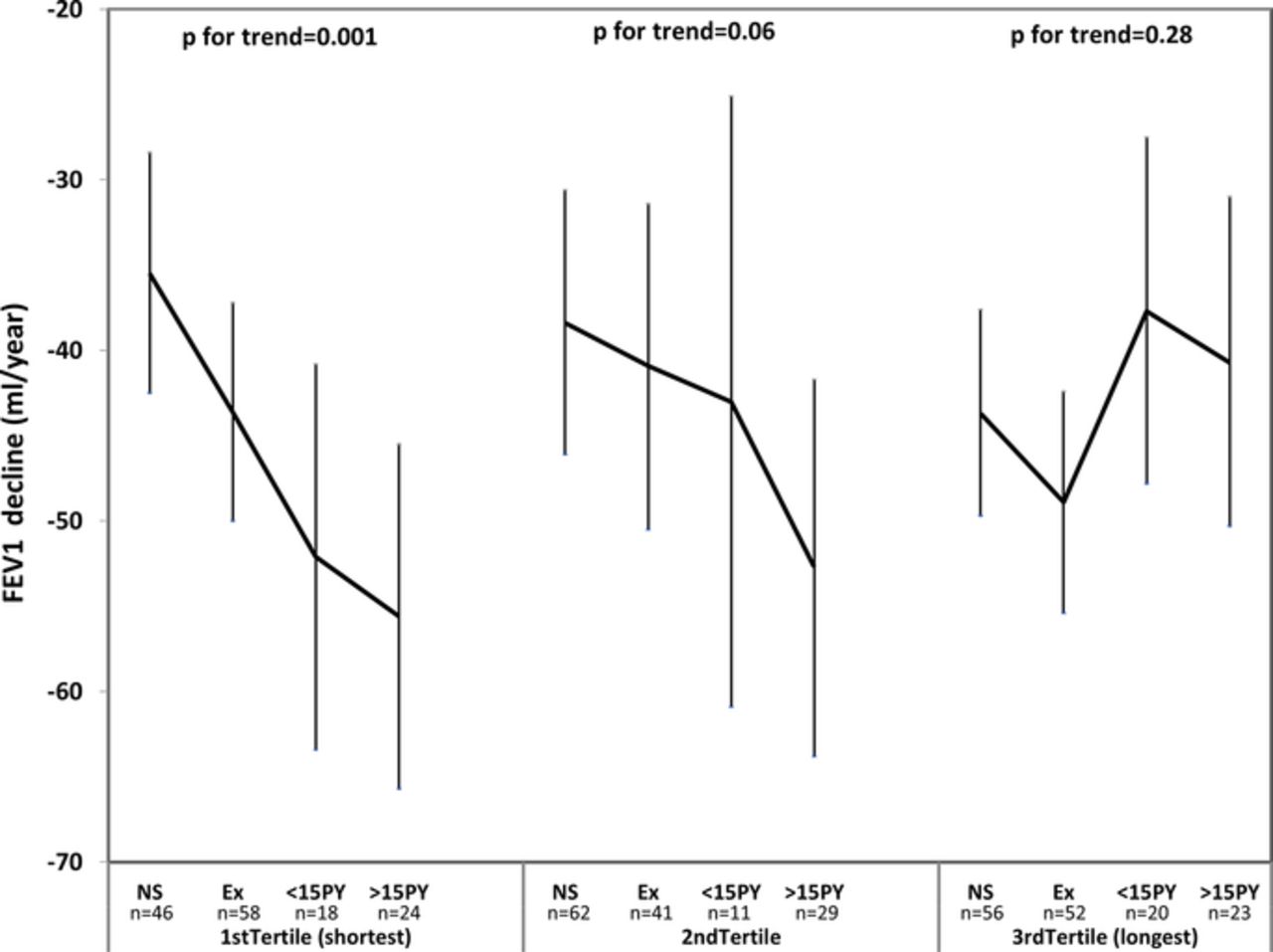
There was no association of FEV1 decline with telomere length at baseline (see online supplementary table E2). FEV1 decline was strongly associated with smoking. However, there was some evidence that this association was modified by telomere length. As shown in figure 1, the effect of smoking on lung function decline was highly significant in subjects with short telomeres (first tertile), and largely reduced and non-significant in subjects with long telomeres (third tertile). In subjects with short telomeres, heavy smokers had an accelerated decline of FEV1, with an additional loss of −20.1 mL/year (95% CI −32.7 to −7.5) as compared with never smokers (table 1). In contrast, no effect of smoking was observed in subjects with long telomeres. Test for interaction showed significant interactions of short telomere length with both moderate (p=0.03) and heavy smoking (p=0.02) (see online supplementary table E3). Similar patterns were seen in the sensitivity analyses (table 1). Consistently, heavy smoking was associated with a reduction in FEV1%predicted at follow-up of −14.9 (95% CI −22.3 to −7.4) in subjects with short telomere length, but no reduction (+2.3%) in those with long telomeres (see online supplementary table E4).

{kind=link}
Adjusted mean* (95% CI) annual FEV1 decline according to smoking status and tertile of telomere length. Smoking status is defined according to smoking history at follow-up: Never smokers (NS); Ex-smokers (Ex); Current smokers or recent quitters with ≤15 pack-years smoked (<15 PY); Current smokers or recent quitters with >15 pack-years smoked (>15 PY). Telomere length is assessed at baseline. *Adjusted for age, gender, centre, body mass index, physical activity and baseline FEV1.
Difference in annual decline in smokers as compared with never smokers, stratified by tertiles of telomere length
Discussion
We believe this is the first population-based longitudinal study investigating the relationships between telomere length and lung function decline. We found that smoking was associated with an accelerated loss in lung function in individuals with short telomeres and with little/no effect in those with longer telomeres.
In our cross-sectional analyses, we found no association of telomere length with FEV1%predicted or FVC%predicted. In a very large sample of the Danish population (comprising +20 000 participants aged over 60 years), there were significant associations of telomere length with FEV1 and FVC but these were largely attenuated after adjustment for age and other covariates.8 A meta-analysis of seven European studies unselected for lung disease showed cross-sectional associations of telomere length with FEV1, FVC and FEV1/FVC ratio, but that were significant only in women.9
Epidemiological studies suggest that variability in telomere length is partly determined by genetic factors, and by modifiable lifestyle factors such as smoking, obesity, physical activity or diet. However, to date, few prospective studies have investigated these relationships. In our sample of mostly healthy individuals, we did not find association between telomere length and lifestyle habits. Telomere length was lower in older participants, which supports the validity of measurements. Our study has some limitations including the relatively small sample size and the limited number of heavy smokers. Because of the relatively young age of the sample, we used a low cut-off (>15 pack-years) to define heavy smokers. Lung function was measured following international guidelines, but spirometers were changed between baseline and follow-up. However, the sensitivity analyses considering smokers with >20 pack-years as heavy smokers, or using lung function corrected for change in spirometers yielded similar relationships.
While tobacco smoke may influence telomere dysfunction, our findings are consistent with the hypothesis that short telomere length might contribute to the differences in susceptibility to the deleterious effect of cigarette smoke in the lung.5 This is consistent with the large cross-sectional Danish study in which participants with COPD had shorter telomere length as compared with subjects with the same history of smoking but who had not developed COPD.8 It is also supported by Savale et al showing shorter telomere length in patients with COPD but no difference in telomere length between control smokers without COPD and control non-smokers.3
To summarise, this population-based longitudinal study suggests that people with shorter telomere length are at increased risk of spirometrically defined COPD. Furthermore, smoking was associated with an accelerated loss of lung function only in individuals with shorter telomeres, suggesting that telomere shortening might be a marker for increased susceptibility to the effect of smoking on lung function decline. Further prospective studies, with repeated measures of both telomere length and lung function, and including sufficient smokers, are warranted to further investigate the predictive value of this biomarker.
References
Footnotes
Contributors PA: Study design, interpretation of data and manuscript writing. JB: Idea of the study, participation in the editing and correction of the final text. DC: Study design, interpretation of data, statistical analysis and manuscript writing. BL: Study design, interpretation of data, and manuscript writing and coordination of the ECRHS study and data collection in French centres. IP: Coordination of the ECRHS study and data collection in French centres and participation in the editing and correction of the final text. PD: Coordination of data collection in a French centre and participation in the editing and correction of the final text. CN: Coordination of data collection in a French centre and participation in the editing and correction of the final text. DJ: Coordination of ECRHS international and participation in the editing and correction of the final text. GT: Participation in the editing and correction of the final text. EM: Biological analysis. EB: Biological analysis. LB: Biological analysis and participation in the editing and correction of the final text. SA: Participation in the editing and correction of the final text. All authors participated in the interpretation of the findings, reviewed the manuscript critically and approved the final version.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Comité de Protection des Personnes Sud Est V.
Provenance and peer review Not commissioned; externally peer reviewed.