Article Text

Statistics from Altmetric.com
Epidemiological studies have consistently found cleaners to be at increased risk of new-onset asthma,1 ,2 the risk seems to be particularly high in domestic cleaners using spray bleaches.2 Due to the large numbers employed in cleaning, they constitute a significant proportion of the population attributable risk of occupational asthma. It has, however, been very difficult to identify the precise cause of domestic cleaners' asthma from specific inhalation challenge (SIC) tests. Chlorine-based substances form the basis of many domestic (sodium hypochlorite) and healthcare (sodium dichloroisocyanurate) cleaning agents. Approximately one third of workers exposed to cleaning agents notified to the UK Health and Safety Executive SWORD (surveillance of work-related and occupational respiratory disease) database with occupational asthma are reported to be due to chlorine-releasing agents (personal communication from Raymond Agius, Institute of Occupational and Environmental Health, University of Manchester). At the Birmingham Occupational Lung Disease Service UK, we have seen 12 healthcare professionals and cleaners with occupational asthma who were exposed to chlorine-releasing agents. In the four investigated with SICs, testing was negative to chlorine-releasing tablets mixed with cold water, and other agents to which they were exposed. Chloramines, particularly nitrogen trichloride, have however been shown to be the cause of asthma in swimming pool attendants and teachers where the chlorine in the water reacts with nitrogen in the urine and sweat of swimmers.3 We hypothesised that similar reactions may be responsible for the asthma in domestic cleaners and healthcare workers and therefore carried out further investigations on the fourth worker to recreate more specifically the workplace exposures (by creating chloramines). We report the four cases who underwent SIC testing and present the fourth worker in detail.
After instruction, all workers were asked to record 2-hourly measurements of peak expiratory flow (PEF) from waking to going to bed on days at and away from work for 4 weeks using a mini-Wright digital metre. The data were downloaded into Oasys (Occupational asthma system) software to calculate the four scoring systems available in the Oasys program.4 ,5 SIC testing was carried out as an inpatient after stopping long-acting β agonists and anticholinergics for 5 days, salbutamol for 6 hours and giving regular inhaled corticosteroid as a single dose before sleeping (where required). FEV1 was measured at baseline, and every 5–10 min during the first hour postchallenge and then hourly for the following 10 hours. Non-specific bronchial reactivity to methacholine was measured using the Carefusion Aerosol Provocation System (APS) or Wrights nebulisers using the Yan method. FENO (where measured) was performed on an Aerocrine Niox Mino pre and 24 hours post each challenge, the latter being prior to the next challenge.
The first three workers with occupational asthma and exposure to chlorine-releasing tablets underwent SICs, including exposures to chlorine-releasing tablets dissolved in cold water. All had work-related changes on their serial PEF measurements and all had negative challenges to the chlorine-releasing agent and other substances to which they were exposed. Table 1 shows their results. None were challenged with chloramines. Details of the fourth patient are given below in more detail.
Summary of workers who had negative SIC tests to chlorine-releasing tablets
A 48-year-old lady had worked in several different care homes as a care assistant since 1999. Haztabs were used to clean the floors at work dissolved in hot water and she had work-related respiratory symptoms related to their use. She had a history of childhood asthma, remitting in adolescence and recurring in 2000. Shortness of breath progressed but improved on stopping smoking in 2001. Work exposures also included latex gloves, nitrile gloves, floor cleaning materials and alcohol hand gel. She had been off sick for 6 months when she was first seen in our clinic and her FEV1 was 1.42 L (54% predicted) and FVC 3.04 (99% predicted) with mild airway hyper-responsiveness (0.94 mg methacholine using the Carefusion APS system, normal >1). She was non-atopic with negative IgE to latex. On return to work, her PEF analysis showed significant deterioration following exposures at work, with a positive work-related effect using all four scoring systems available in the Oasys program; Oasys score 3.12 (positive >2.5), area between curves score (ABC) score 26 L/min/hour (positive >15 L/min/hour), rest-work score 7.4% (positive >3.3%), five positive timepoints (positive >0 non-waking). When performing clerical duties in the same care homes with indirect exposure to the Haztabs, the scores were reduced with an Oasys score of 2.24, ABC of 5 L/min/hour, rest-work score of 1.85% and one positive timepoint (the timepoint analysis can identify statistically significant but often small changes related to work exposures).
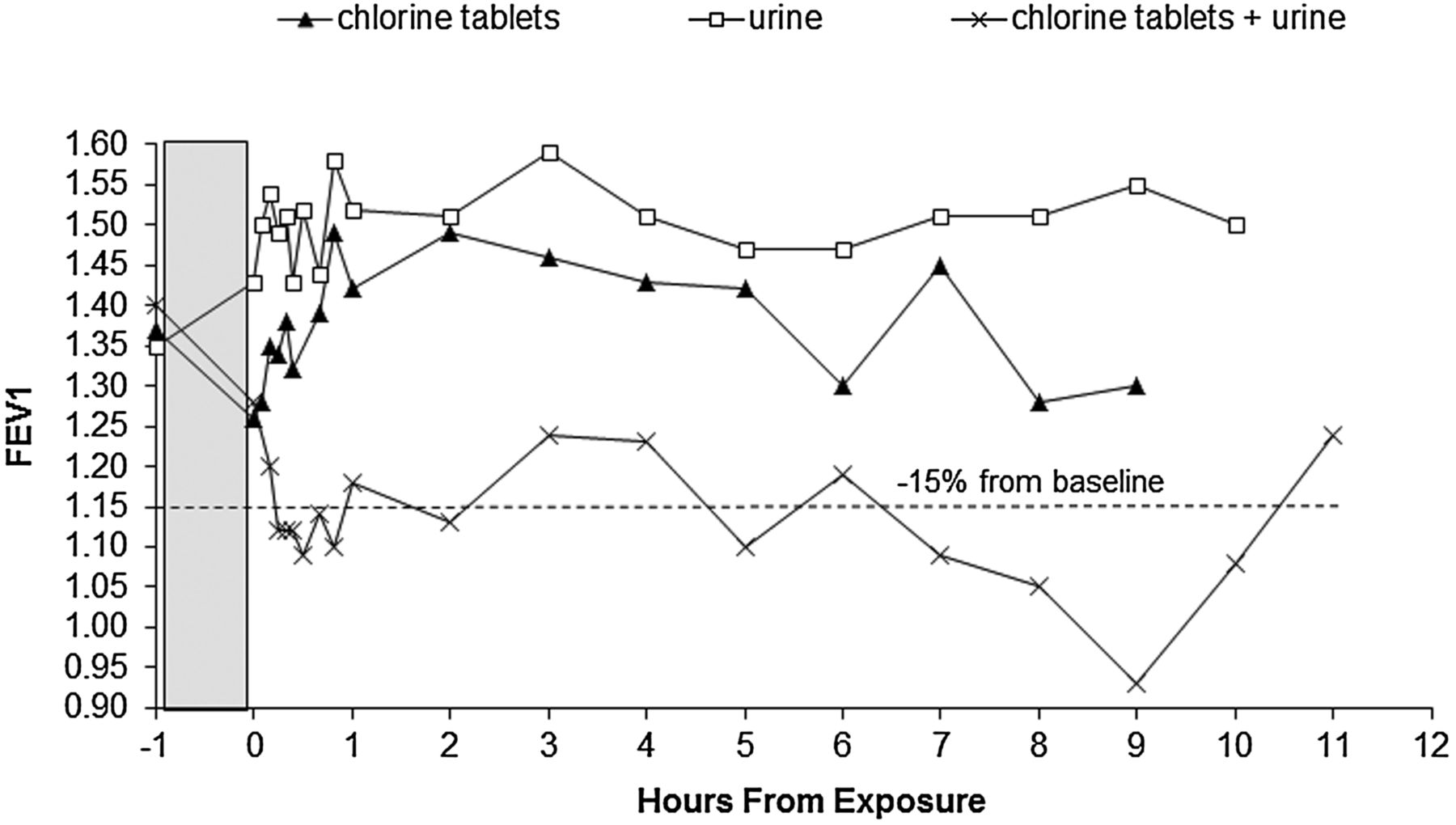
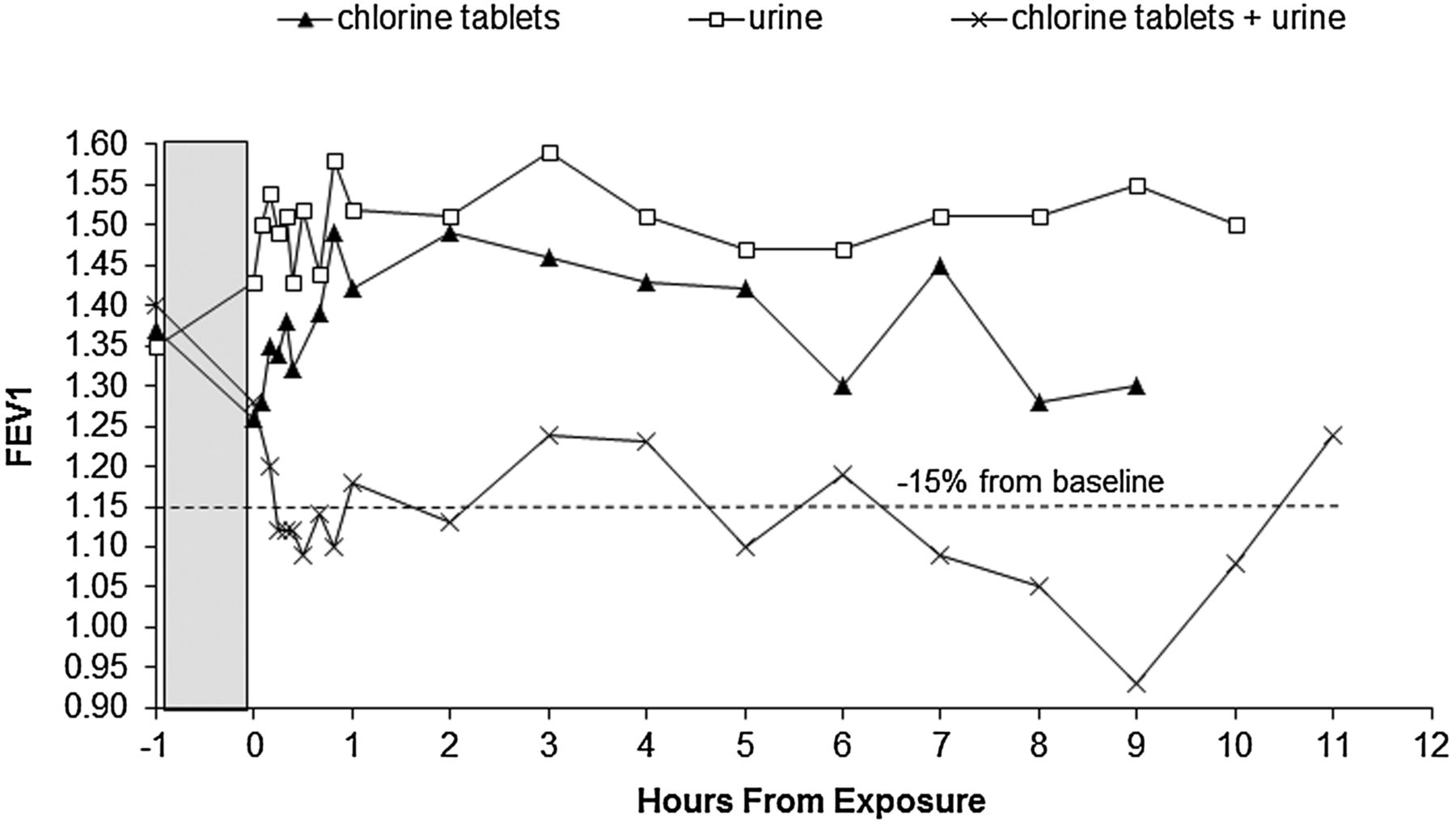
On separate days, exposures for the SIC consisted of neutral detergent solution (as a control), ‘Haztab’ chlorine solution (at a concentration of 10 000 ppm as recommended for blood spills), undiluted urine and a mixture of the diluted Haztab solution with 5% urine. These were painted onto cardboard for a total of 70 min. There were no reactions following exposure to Haztabs or urine alone, nor the neutral detergent. The chlorine and urine mixture provoked a dual asthmatic reaction and a sustained drop in FEV1 to a maximum of 34% from baseline (figure 1). Hyper-responsiveness was not repeated postchallenge as her FEV1 was too low at 1.02 L (39% predicted) 24 hours later. Her FENO declined slightly from 27 ppb before all challenges to 22 ppb 24 hours after the chlorine and urine mixture challenge. Her FEV1 improved back to her prechallenge baseline the following day. She returned to work but found that indirect exposures to chloramines still caused some symptoms, so she was retired on medical grounds. Her asthma continues but is considerably improved; her most recent spirometry showed FEV1 1.51 L and FVC 3.31 L.
{kind=link}
Specific inhalation challenge results to chlorine tablets, urine alone and the chlorine and urine mixture showing a sustained fall in FEV1 of up to 34% from baseline. The shaded box denotes the exposure.
Lessons
SIC tests to the chlorine-releasing agent and urine individually produced negative results. However, the combination of urine with the chlorine-releasing agent, replicating the actual workplace exposure, produced a positive asthmatic reaction. It is likely that the chlorine and urine mixture produced chloramines. Chloramines are known sensitisers causing occupational asthma in swimming pool attendants and teachers, where SICs have shown chloramines to be the cause.3 We believe that this explains the previous negative tests to chlorine-releasing agents alone in healthcare workers, where chloramines produced in cleaning operations at work are the likely cause of much of their occupational asthma. Any SIC tests to chlorine tablets should be performed with a nitrogen source when exposures to the chlorine-releasing substance alone do not elicit an asthmatic reaction. The optimal management of a worker with occupational asthma requires identification of the specific cause, so that exposures can be reduced for others and eliminated for the sensitised worker. In this case, the cause was identified but unfortunately removal from direct exposure was insufficient to eliminate all work-related symptoms and small changes in peak flow (as shown by the positive timepoint analysis). With the help of her occupational health department, our patient decided to retire on medical grounds, which is sometimes the best solution.
Informed consent
The care assistant with positive challenges has provided informed consent for this case-based discussion.
Acknowledgments
The authors would like to thank Edward Parkes for performing some of the specific inhalation challenge tests.
Footnotes
Contributors VCM is the main author and clinical scientist carrying out the majority of the specific inhalation challenge tests. ASR, PSB and GIW have seen the workers clinically and have contributed to the writing of the paper.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.