Article Text

Statistics from Altmetric.com
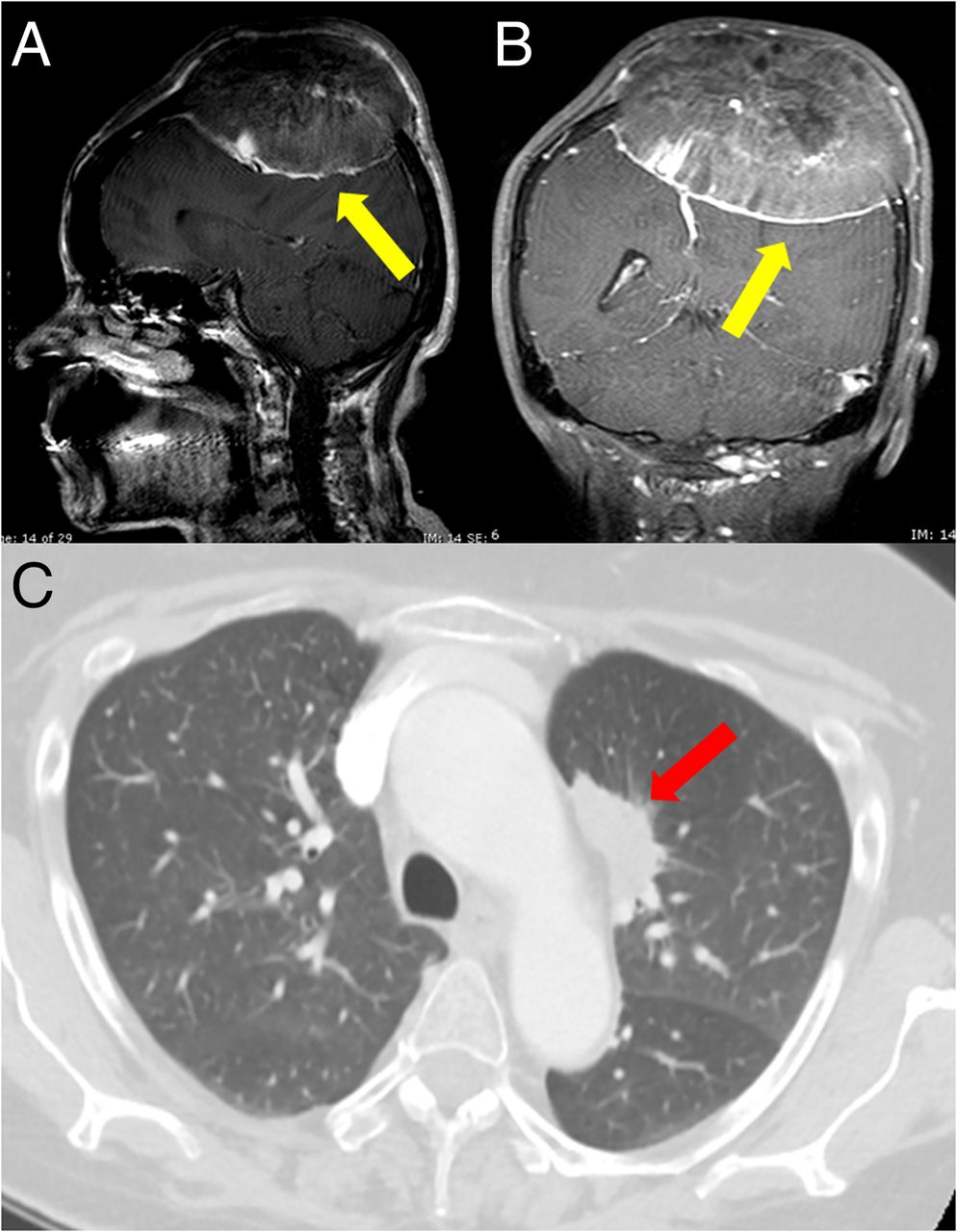
A 55-year-old woman presented with a progressive psychomotor impairment. She spoke slowly and her motor retardation interfered with activities of daily living. The patient reported that 5 months earlier, she had experienced blunt force trauma of vertex with a progressive swelling of the head. At the time of presentation, a painful, fixed and hard lesion was detected at palpation. Encephalic CT and MRI revealed an osteolytic mass of the skull of 10 cm in maximum diameter, infiltrating the left frontoparietal bones with calcifications (figure 1A, B). The lesion caused a mass effect, without infiltration of the brain parenchyma. A whole-body CT discovered a 4 cm pulmonary lesion of the left upper lobe (figure 1C). The biopsy (figure 2) of the skull mass revealed a metastatic pulmonary adenocarcinoma (thyroid transcription factor 1 positive, p40/ΔNp63 negative). Molecular analysis disclosed a sensitising exon 19 (delE746-A750) epidermal growth factor receptor (EGFR) gene mutation. ALK and ROS-1 rearrangements were negative. An EGFR inhibitor (erlotinib, 150 mg once daily) was started. The women experienced a significant clinical benefit with a slight dimensional reduction of the pulmonary lesion (stable disease according to revised RECIST guidelines1) while the skull metastasis was stable with an increased density at 8 months follow-up.

Brain CT scan showed the 10 cm skull mass infiltrating left frontoparietal bones with concurrent calcifications (A and B, yellow arrow). Thoracic CT scan disclosed a 4 cm lesion of the left upper lobe with peripheral ground glass opacities (C, red arrow).

{kind=link}
{kind=link}
Histological examination (H&E) of the skull lesion revealed an adenocarcinoma with glandular pattern of growth (on the left) infiltrating bone (on the right) with nuclear expression of thyroid transcription factor 1 (TTF-1) at immunohistochemistry (inset) consistent with metastatic lung adenocarcinoma to the skull.
In dealing with a skull mass, the first differential diagnosis is between primary and metastatic neoplasms of various cell lineages, including soft tissue tumours, haematologic proliferations, brain tumours and metastasis from several neoplasms.2 A close correlation between clinical and radiological data together with morphological and immunohistochemical stains on biopsy is mandatory.2 Among carcinomas, skull metastases are mostly noted in hepatocellular carcinoma, cholangiocarcinoma, prostate, thyroid and breast cancers.2 Although the rate of bone metastases associated with lung carcinoma is estimated at 36%, only 3% of lung cancers metastasise to skull.3 Skull metastases are usually diagnosed as multiple lesions in the context of a known primary tumour.2 Rarely do they represent the first single manifestation of an unknown carcinoma,4 and lung adenocarcinoma presenting as skull mass is exceedingly rare.3 No significant relationship has been demonstrated between EGFR mutation and this unusual metastatic pattern.
Footnotes
Contributors MCM conceived and wrote the manuscript. GR performed the pathological evaluation. MT performed the literature review. FB supported in the comprehension of the oncological aspects. MP collected radiological imaging. FB was involved in the oncological cares of the patient. FL wrote along with MCM the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.