Article Text

Statistics from Altmetric.com
A 38-year-old man presented to a previous hospital in December 2011 with a high fever and acute abdominal pain. He was found to have abdominal lymphadenopathy and was diagnosed with HIV infection. His CD4 count was 25/mm3 and viral load was 490 000 copies/mL. He was transferred to our department for further investigations and treatment. Whole body CT revealed bulky, widespread lymphadenopathy, especially in the abdomen, but no ascites or pleural effusion (figure 1A, B). Stool, bone marrow and an abdominal lymph node specimen were positive for acid-fast bacillus stain. A diagnosis of disseminated non-tuberculous mycobacterial infection (NTM) with Mycobacterium genavense was confirmed by 16S rRNA gene sequence analyses of a sample of bone marrow and a lymph node specimen. Antiretroviral therapy with raltegravir+tenofovir+emtricitabine anti-NTM treatment with clarithromycin+ethambutol+rifabutin+streptomycin and prednisone 0.5 mg/kg/day to prevent immune reconstitution syndrome were introduced. However, bulky abdominal lymphadenopathy persisted despite treatment and led to recurrent intestinal obstruction and ileal strangulation requiring surgical intervention. The abdominal symptoms were markedly relieved after 8 months of treatment, though the bulky lymphadenopathy persisted.

(A) No pleural effusion was identified in 2011. (B) Bulky abdominal lymphadenopathy was identified in 2011. (C) Small amount of pleural effusion was identified in 2012. (D) Abdominal lymphadenopathy enlarged in 2012. (E and F) Chylothorax was confirmed. (G and H) Pleural effusion worsened in 2013.
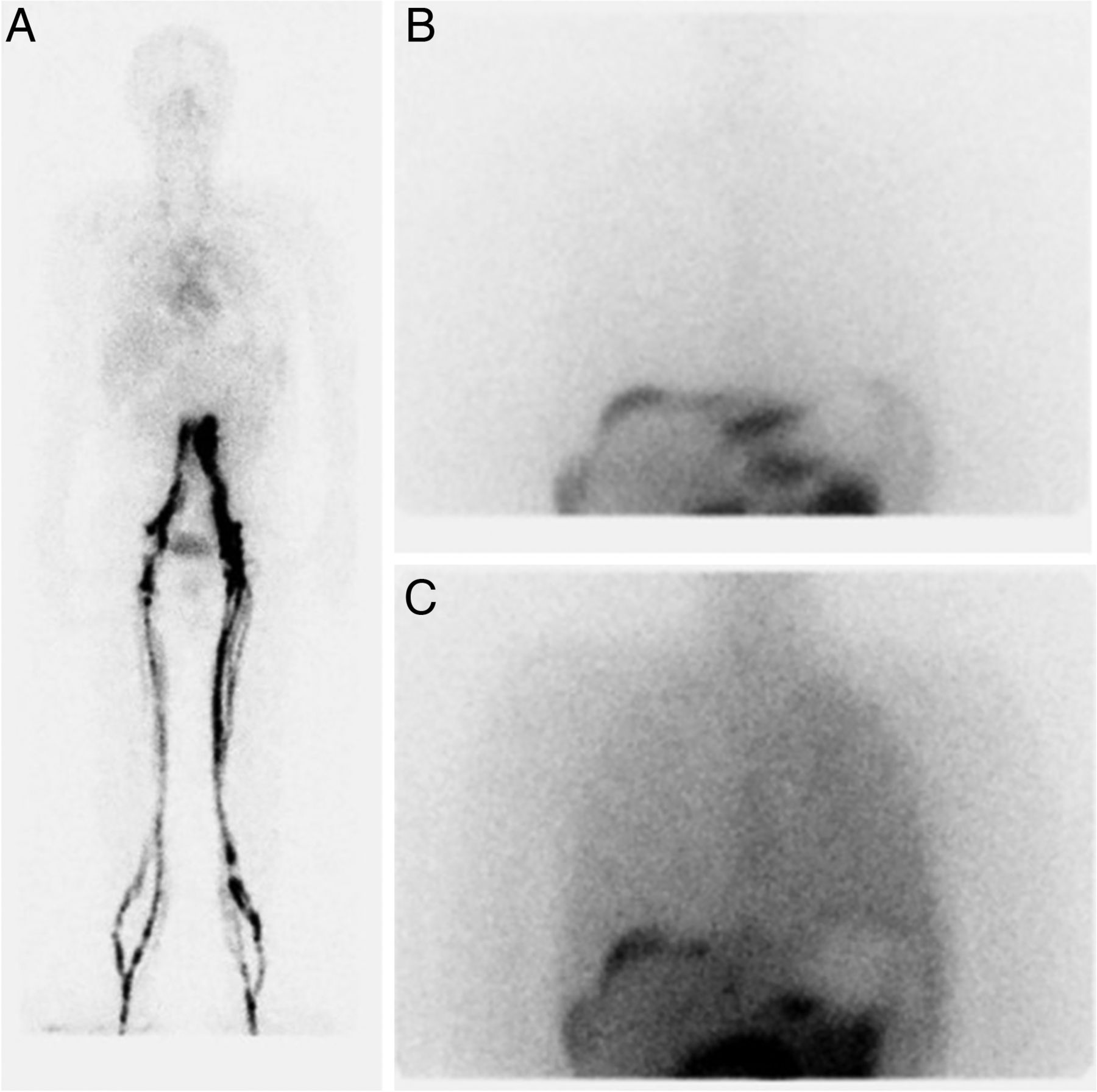
Ascites and a chylous pleural effusion were identified 1 year after treatment initiation, in December 2012 (figure 1C–F). Obstruction or destruction of the thoracic duct by disseminated NTM infection was considered as a possible cause of the chylothorax. The bilateral pleural effusion had progressed further by April 2013 (figure 1G, H). Lymphoscintigraphy confirmed lymphatic obstruction and thoracic duct leakage (figure 2A–C).
{kind=link}
{kind=link}
Dynamic lymphoscintigraphy images. (A) Tc-99m lymphoscintigraphy after tracer injection in the lower limbs showed lymphatic obstruction at the abdominal level. (B) Thoracic duct scintigraphy with oral I123 β-methyl-iodophenylpentadecanoic acid showed tracer accumulation in the intestine, but not in the thorax, at 8 h after administration. (C) Tracer accumulation was identified in the thorax at 24 h after administration.
Non-malignant AIDS-related chylothorax has been reported in association with Kaposi's sarcoma and TB,1 ,2 but no cases related to NTM have been reported. Continued loss of immunoglobulins and T lymphocytes into the pleural effusion leads to immunosuppression, and we anticipate that the survival prognosis in such cases will be poor, unless the chylothorax is controlled.3 A number of additional interventions can be considered for the management of chylothorax, including pleural drainage, dietary modifications (fasting or reduced fat diet), pleurodesis and thoracic duct ligation. However, specific guidelines are lacking, particularly in refractory cases. Long-lasting management guidelines for chylothorax are needed, especially in patients who were immunocompromised, such as those with HIV/AIDS.
Footnotes
Contributors All authors cared for the patient. TT wrote the report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves