Article Text

Abstract
Malignant pleural mesothelioma causes the greatest societal burden of all the asbestos-related diseases. Progress in better understanding tumour biology will be facilitated by the availability of quality-assured annotated tissue. MesobanK has been created to establish a bioresource of pleural mesothelioma tissue linked to detailed anonymised clinical data. When complete, the bioresource will comprise a 750-patient tissue microarray and prospectively collected tissue, blood and pleural fluid from 300 patients with mesothelioma. Twenty-six new cell lines have also been developed. MesobanK meets all appropriate ethical and regulatory procedures and has recently opened to requests for tissue and data.
- Mesothelioma
- Histology/Cytology
- Asbestos Induced Lung Disease
- Pleural Disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
The UK has the highest incidence of asbestos-related disease per head of population in the world. Of the various asbestos-related diseases, malignant pleural mesothelioma (MPM) imposes the greatest societal burden. Despite the import of asbestos into the UK having been banned for two decades, Health and Safety Executive data for 2012 shows that MPM caused 2535 deaths in England, Wales and Scotland.1 This is a legacy of the latency period from exposure to disease of up to 50 years. While cases of MPM in Western Europe and North America should begin to fall over the next 30–40 years, the use of asbestos in Asia, South America and states of the former Soviet Union is increasing and it is believed that some 125 million people globally are exposed in the workplace.2 Therefore, lessons learnt about MPM will have a major impact on global health for decades to come.
Until recently there has been a relative paucity of basic and translational research into MPM, but it is now widely accepted that progress in diagnosis and treatment is only likely to be achieved with a better understanding of tumour biology. As with many other rare cancers, the fundamental mechanisms regulating the processes underpinning cell growth and death in MPM are poorly understood owing to a lack of appropriate high-quality clinical samples. Such research will be facilitated by the availability of quality-assured annotated tissue.
Although there are several mesothelioma tissue collections in various countries, most operate as ‘virtual’ collections of tissue rather than as a centralised collection. This means that rather than being held in a central location, samples are stored in a variety of institutions under non-standardised conditions having been collected to differing operating policies. Similarly, although a few UK-based clinical/research groups hold fresh tissue from small numbers of patients with MPM, these collections are not formally linked and do not involve the collection of tissue and data in accordance with any universal standard operating procedures (SOPs).
MesobanK UK (http://www.mesobank.com) has been established through funding from the British Lung Foundation (BLF) and the Mick Knighton Mesothelioma Research Fund as a result of a BLF/National Cancer Research Institute call for a bioresource to underpin research into asbestos-related disease.3
The overall goal of MesobanK is to provide a framework for the systematic collection, curation and quality assurance of well-annotated mesothelioma tissue that will facilitate high-quality basic science, translational and clinical research into mesothelioma.
The objectives are to:
Establish a bioresource of MPM tissue and blood linked to a detailed clinical database.
Develop novel annotated mesothelioma cell lines.
Put in place a web-based information technology infrastructure for annotating and searching the bioresource.
Develop a robust infrastructure to allow long-term sustainability at reasonable cost to facilitate research that will develop novel therapies and diagnostic tools more efficiently and quickly.
Tissue bioresource
The tissue bioresource comprises two parts:
In order to facilitate high-throughput analysis of biomarkers suitable for real-world clinical use, we are constructing a tissue microarray (TMA) containing tumour samples from 750 known patients with MPM. This is being constructed using formalin-fixed paraffin-embedded blocks with high-quality anonymised-linked clinical data from cases that have been diagnosed in hospitals across the UK in the last 10 years. A minimum of four cores is taken from each block to allow for tumour heterogeneity. The TMA is being constructed in modular form so that researchers can readily test their biomarkers of choice on a selection of cases and then validate their results on a separate large cohort. TMA slides will be scanned into a digital pathology imaging system to facilitate remote web-based viewing and scoring of stained TMA sections. In order to preserve antigenicity cut slides will be dipped in paraffin wax and stored at 4°C.
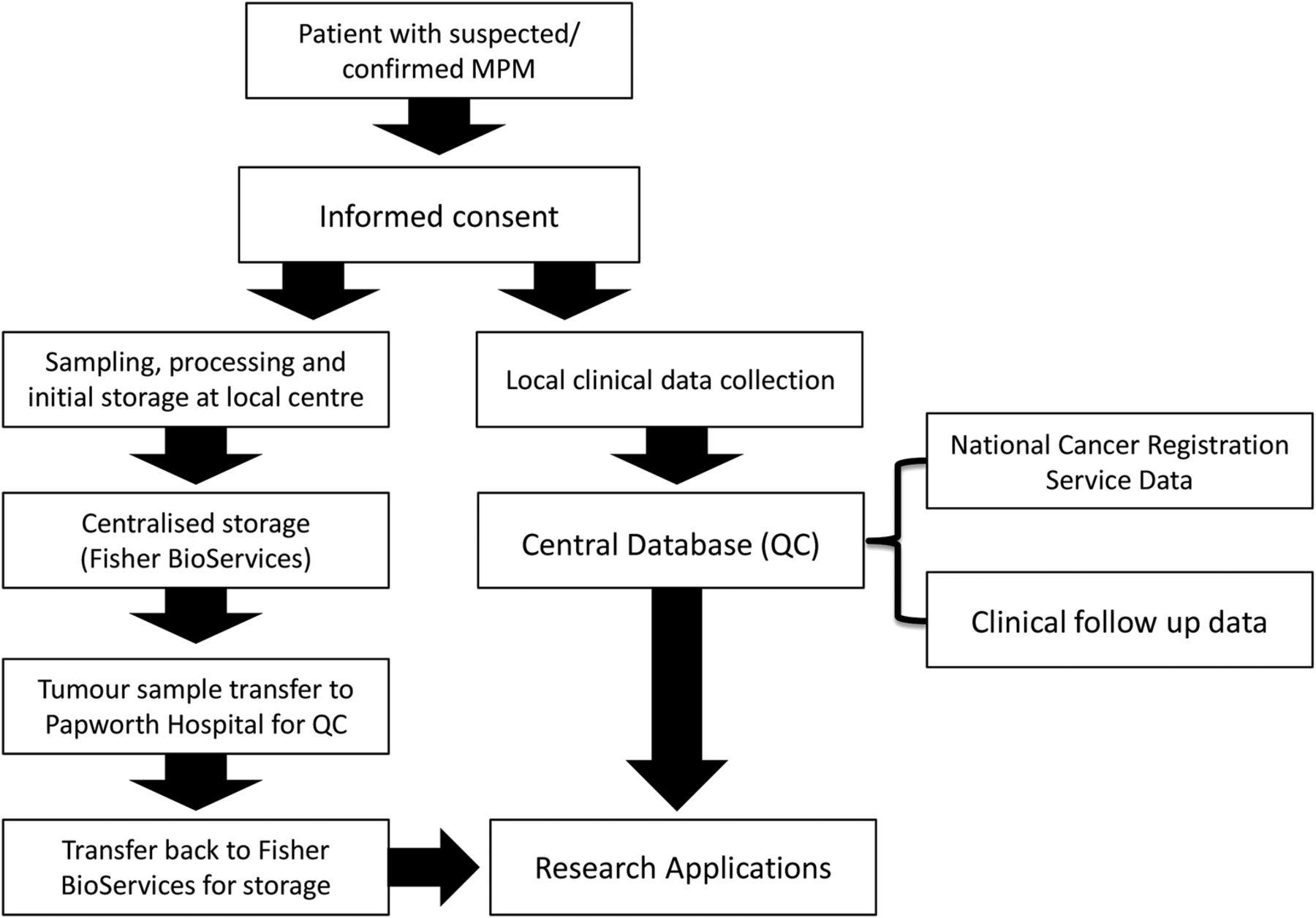
In parallel, we are prospectively collecting tissue, blood, pleural fluid and data from 300 patients across the UK with confirmed or suspected MPM undergoing routine diagnostic or treatment procedures as shown in figure 1.
{kind=link}
Flow diagram for patient samples and data. QC, quality control.
Multiple surgical tissue samples are being collected from each patient and stored in a manner suitable for histological, proteomic, genomic or transcriptomic analysis at a later date. Prior to archiving, each tissue sample is being reviewed centrally by our histopathologist for size, percentage tumour nuclei and percentage necrosis so that researchers can select those samples most suited to their project goals. In addition, blood is stored as serum, plasma and buffy coat fractions along with matching pleural fluid (cell pellets and supernatant) when available. When processed, all samples are stored under strictly controlled conditions at −80°C at Fisher BioServices, UK, ready for shipment to researchers on request. To facilitate sample collection we provide standardised collection kits containing a complete set of prebarcoded blood, pleural fluid and tissue sample pots. Once samples are processed according to MesobanK SOPs, they are scanned into the centralised secure database which links each sample and patient code without the need for sample containers to be labelled with patient identifying information. Details of MesobanK SOPs are available at http://www.mesobank.com. In addition to our planned collection, bespoke sample collection can be arranged on request.
Anonymised-linked clinical data for every prospective and retrospective case are entered into a purpose-built database. Although retrospective data collection for TMA samples is frequently challenging to obtain, a minimum data set of commonly recorded clinical information has been defined (see online supplementary appendix 1). The local clinical data set will be supplemented by data drawn from the National Cancer Registration Service (NCRS). This will ensure that the MesobanK TMA will be the world's most comprehensive resource of this type. To ensure comprehensive and accurate data accompanies every prospective sample, the NCRS will provide MesobanK with six monthly data updates about subsequent treatment episodes and survival.
Cell lines
Another important hindrance to clinical research into MPM is a lack of high-quality cell lines for in vitro studies. Many of the existing lines were generated a number of years ago and no longer represent good models for their original tumours. To address this, in collaboration with Professor Marion MacFarlane, Medical Research Council (MRC) Toxicology Unit, University of Leicester and Dr Zsuzanna Tabi, University of Cardiff, 26 new MPM cell lines have been generated for MesobanK.
Primary tumour surgical tissue or pleural fluid cells are grown in Roswell Park Memorial Institute (RPMI) medium supplemented either with 10% fetal calf serum (FBS) or with 2% FBS, 2% hydrocortisone, epidermal growth factor and heparin depending upon the source laboratory. Cells have been passaged between six and nine times to expand their number and remove fibroblast contamination. The original tumour subtype, patient gender and age are provided along with cell line immunoreactivity to mesothelin, calretinin and cytokeratins and in some cases 5T4, podoplanin and HBME1. Neither karyotyping nor short tandem repeat PCR has been performed, but when provided by user laboratories we will make this available. Depending upon the source laboratory of each cell line further characterisation has been performed on selected lines including human leucocyte antigen typing and scanning electron microscopy. End users will be asked to monitor the characteristics and behaviour of each cell line over time in order to ensure that they remain true to the original cultures details of which are available from the central MesobanK distribution laboratory (SJM, Cambridge Institute for Medical Research).
Governance
MesobanK follows the ‘Guiding Principles’ laid out by the National Cancer Research Institute Confederation of Cancer Biobanks4 and the MRC Operational and Ethical Guidelines on ‘Human Tissue and Biological Materials for Use in Research’.5 The Health Research Authority Confidentiality Advisory Group has granted MesobanK permission to extract data from the NCRS using exemption from Section 251 of the Health and Social Care Act 2001 for TMA samples of patients who are deceased without having to ask living relatives for consent. For prospective specimen collection ethical approval has been granted to set up MesobanK as a Research Tissue Bank. The Human Tissue Authority (HTA) and National Research Ethics Service have agreed a position whereby National Health Service (NHS) research ethics committees can give generic ethical approval for a research tissue bank's arrangements for collection, storage and release of tissue, providing the tissue in the bank is stored on HTA-licensed premises. This approval can extend to specific projects receiving non-identifiable tissue from the bank. The tissue does not then need to be stored on HTA-licensed premises nor does it need project specific external ethical approval for research being undertaken in the UK. Prior to contributing any samples, all patients are requested to give informed consent for blood and tissue banking in accordance with the Human Tissue Act (2004)/Human Tissue (Scotland) Act 2006. Each patient is provided with detailed written information about the nature of the tissue bank along with any risk, discomfort or potential benefit derived from participation. A tiered consent process is in place with participants able to consent to which sample types they are prepared to donate. All subjects are asked to consent to collection of data about their subsequent clinical care and outcome. The patient information sheet and consent form make specific reference to collection of data from the NCRS and other sources. All subjects are made aware of their right to withdraw their consent for the use of their tissue/blood or clinical information at any time. The principles of good clinical practice are adhered to throughout the biobanking process.
A steering committee with an independent chair has been appointed to oversee the tissue bank. A project manager supported by a project team, both based at Papworth Hospital NHS Foundation Trust, assumes day-to-day responsibility for MesobanK and oversees all operational aspects of the bioresource.
Access to samples
Requests for access to samples and data can be made to MesobanK. Applications are reviewed by the project team who can call upon a Research Advisory Board comprising scientific, clinical and lay members to advise upon the ethical and scientific integrity of projects, when necessary. Subject to these caveats and tissue availability, samples will be made available whenever possible. Researchers will be encouraged to make findings obtained using MesobanK samples freely available to other researchers. Although MesobanK is a not-for-profit project, a cost-recovery model is in place to recover direct and indirect costs incurred in collection, processing, quality control and curation. All fees are used to offset future running costs of MesobanK in order to ensure long-term sustainability.
In summary, we have established a international bioresource to assist the biomedical community tackle this devastating cancer. Although retrospective and prospective tissue collection is not yet complete, we are already in a position to supply researchers with these valuable samples. Finally, we wish to thank all those patients and relatives who have so kindly made this possible.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Collaborators The MesobanK collaborators group: Fiona Black, Kevin G Blyth, Richard Booton, Paul Cane, Anoop Chauhan, Helen Doran, John G Edwards, Dean A Fennell, John R Gosney, Peter Hamilton, Vikki Hughes, Sam M Janes, Keith M Kerr, Alan Kirk, Marion MacFarlane, Nick A Maskell, Mohammed Munavvar, Babu Naidu, Apostolos Nakas, Naj M Rahman, Trevor Rogers, Marco Scarci, Michael Shackcloth, Irshad Soomro, Kim Suvarna, Peter W Szlosarek, Zsuzanna Tabi, William A Wallace and David A Waller.
Contributors RCR had the original concept for the article and wrote the initial draft. JG, DMR and SJM reviewed and revised the manuscript. All authors approved the final manuscript. RCR is the guarantor of the overall content.
Funding British Lung Foundation (ABR 12-1), Mick Knighton Mesothelioma Research Fund. RCR and DMR are part funded by the Cambridge Biomedical Research Centre and the Cambridge Cancer Centre. RCR is also funded by the NIHR Clinical Research Network: Eastern.
Competing interests None declared.
Ethics approval National Research Ethics Service; Health Research Authority Confidentiality Advisory Group.
Provenance and peer review Not commissioned; externally peer reviewed.