Article Text

Abstract
Background The natural history of asthma includes in some patients periods of disease remission, but the underlying mechanisms are unknown.
Objectives We explored whether type 1 myeloid dendritic cell (mDC) dysfunction could be involved in the persistence of asthma, studying the controlled setting of occupational asthma after allergen avoidance.
Methods We recruited 32 patients with occupational asthma to flour or latex ascertained by specific inhalation challenge and who were no longer exposed to the causal allergen. Leukapheresis was performed in each patient to isolate and characterise blood type 1 mDCs, and their functionality was studied in coculture with allogeneic CD4+ T cells from controls.
Results At follow-up, 11/32 patients (34%) were characterised by the absence of symptoms and non-specific bronchial hyper-responsiveness to histamine and were considered to be cured. When compared with cured patients, mDCs from patients with persistent disease increased the production of interleukin (IL) 5 and IL-13 by CD4+ T cells, and upregulated programmed death ligand 2 (PD-L2) upon allergen pulsing. In addition, IL-5 and IL-13 responses could be reversed by exogenous IL-12, as well as by PD-L2 blockade.
Conclusions This study indicates that pro-Th2 features of mDCs correlate with disease activity in asthma after cessation of exposure to the causal allergen. The findings also highlight that the Th2 programming by dendritic cells is flexible and partly mediated by PD-L2.
- Allergic lung disease
- Asthma
- Asthma Mechanisms
- Occupational Lung Disease
Statistics from Altmetric.com
Key messages
What is the key question?
The natural history of asthma includes in some patients periods of disease remission, but the underlying mechanisms are unknown.
What is the bottom line?
We studied myeloid dendritic cell (mDC) functionality in a well controlled setting, namely patients with occupational asthma with either remission or persistence following complete allergen avoidance.
Why read on?
This study shows that blood mDCs from patients with occupational asthma and persistent disease despite allergen avoidance are imprinted with pro-Th2 activity.
Introduction
The mechanisms associated with asthma recovery or persistence have almost never been explored. In addition, although allergen avoidance is recommended in the management of allergic asthma, strategies to reduce allergen exposure failed to show a clear benefit.1 In this regard, IgE-mediated occupational asthma (OA) induced by high molecular weight agents is a specific condition that offers the possibility to strictly control exposure to the causal allergen. Nonetheless, the outcome of OA following cessation of exposure is disappointing, with only about a third of the patients recovering from their symptoms and non-specific bronchial hyper-responsiveness (NSBHR).2 ,3 Studies on OA have shown that failure to improve NSBHR upon allergen avoidance was associated with higher levels of inflammatory cytokines in sputum and persistent airway inflammation,4 ,5 but the immune mechanisms involved remain unknown.
Type 1 myeloid dendritic cells (mDCs) are professional antigen-presenting cells that play a key role in the initiation of immune responses. Their role in asthma inception has been highlighted for 15 years.6 Besides their ability to present allergens to naïve T cells, mDCs are able to shape the immune response through the secretion of cytokines and expression of costimulatory molecules. The role of some costimulatory molecules has been recently explored in human asthma,7 including the first and second ligands to programmed death-1 (PD-L1 and PD-L2)8 ,9 and the ligand to immune costimulator,10 as factors involved in the intrinsic pro-Th2 bias of mDCs from patients with asthma.11 ,12 mDCs from patients with allergic asthma also have an intrinsic propensity to respond to proallergic epithelial cytokines such as thymic stromal lymphopoietin.13
Given the pivotal role of mDCs in asthma inception and progression, we hypothesised that these cells might be involved in asthma recovery or persistence following allergen avoidance. In this study, the phenotype and function of mDCs were correlated to the clinical outcome of asthma (ie, persistence vs remission) in the well controlled setting of allergen-driven OA following cessation of exposure to the causal allergen.
Material and methods
For detailed information, please refer to the online supplementary materials.
Patients and clinical assessments
The study included patients with OA to natural rubber latex (n=18) or flour (n=14) confirmed by a specific inhalation challenge, who completely avoided exposure to the causal allergen after the diagnostic evaluation. At initial and follow-up assessments, the patients were administered a questionnaire aimed at collecting detailed information on workplace exposure, asthma symptoms and antiasthma medications. Spirometry was assessed in accordance with the standards of the American Thoracic Society,14 and the level of BHR to histamine was measured through the tidal breathing method15 and expressed as the concentration of histamine inducing a 20% decrease in FEV1 (PC20). The outcome was defined as: (1) ‘cured asthma’ (sometimes also mentioned as ‘asthma recovery’ or ‘remission’ in the text) when the patients no longer experienced asthma symptoms, did not use antiasthma medication and showed a histamine PC20 value >8 mg/mL; and (2) ‘persistent asthma’ when the patients failed to meet any one of these criteria. In addition, the serum from the 18 patients with latex allergy was tested for its sensitivity to the major latex allergen Hev b 6.02, using Immunocap (Thermo Scientific, Waltham, Massachusetts, USA).
Dendritic cell purification
The patients underwent a leukapheresis to obtain a buffy coat. Peripheral blood mononuclear cells were isolated after centrifugation on Lymphoprep (Axis-Shield, Oslo, Norway). Type 1 mDCs were isolated using immunomagnetic separation (MACS, Miltenyi Biotecs, Bergisch Gladbach, Germany). After B cell depletion with anti-CD19 microbeads, mDCs were positively selected with anti-CD1c (blood dendritic cell antigen (BDCA) 1) microbeads. This technique yields type 1 mDC purity above 95%, as shown in online supplementary figure S2A.
For phenotyping, DCs were cultured overnight in 48-wells plates (500 000 cells/well at 1 million cells/mL) in RPMI-1640 medium supplemented with 10% of fetal calf serum, Streptomycin (100 U/mL), Penicillin (100 U/mL) and L-glutamine at a 2 mM concentration (Lonza, Verviers, Belgium), further referred to as complete RPMI. DCs were cultured either alone, with the relevant allergen extract (ie, latex or flour, 10 µg/mL, Stallergènes, Antony, France) or with LPS (TLR4 agonist) at 1 µg/mL (Sigma Aldrich, Saint-Louis, Missouri, USA). In eight patients sensitised to the Hev b 6.02 allergen component of latex (Biomay, Wien, Austria), this recombinant allergen protein was also used at a final concentration of 2 µg/mL.
To investigate the regulation of T cell responses by DCs, the model of coculture with allogeneic CD4+ T cells was used as it previously showed that the allergic origin of DCs may overcome the effect of HLA mismatch, as evidenced by the induction of Th2 cytokine release by control CD4+ T cells.11 ,12 ,16 CD4+ T cells were purified from peripheral blood mononuclear cells of non-allergic, non-asthmatic donors using anti-CD4 microbeads (Miltenyi Biotec, Bergisch Gladbach, Germany). Resting or stimulated mDCs were washed and cultured with these allogeneic CD4+ T cells in 96-well plates at a ratio of 1:5 (40 000 mDCs for 200 000 T cells) for 5 days in complete RPMI supplemented with 100 nM β–mercaptoethanol, as previously described.10 ,13 In selected experiments, a blocking mAb to human PD-L2 (Biolegend, San Diego, California, USA) or a mouse IgG1 as isotype control (eBioscience, San Diego, California, USA) were used (10 µg/mL), as well as recombinant human interleukin (IL) 12 p70 (10 ng/mL; R&D Minneapolis, Minnesota, USA).
Cell analysis and cytokine measurements
After surface staining, mDC phenotype was studied on a FACS Canto II flow cytometer (BD Biosciences, San Diego, California, USA).
IL-5, IL-13, IL-9, IL-10 and interferon γ levels at the end of mDC-T cell coculture were measured by ELISA.
Statistics
Quantitative data are presented as median with IQR. Flow cytometry data are expressed as the percentage of positive cells compared with isotype control. For non-parametrical data, multiple comparisons were completed using the Kruskal-Wallis test followed by Dunn's multiple comparison test. For single comparisons, unpaired data were analysed by the Mann-Whitney U test and paired data by the Wilcoxon matched pairs test. A p value under 0.05 was considered as statistically significant. Statistical analyses were performed using GraphPad Prism V.5.00 for Windows (GraphPad Software, San Diego, California, USA; http://www.graphpad.com) and IBM SPSS Statistics V.21 (Armonk, New York, USA). Statistics were reviewed by a statistical platform (Support en Méthodologie et Calcul Statistique—SMCS, Université catholique de Louvain, Louvain-la-Neuve, Belgium).
Results
Clinical characteristics of the participants
Table 1 summarises the clinical features of the subjects defined as having persistent versus cured asthma at the follow-up visit. When comparing their characteristics at the time of the initial assessment, the two groups did not differ significantly with regard to the causal allergen, age, gender, atopy, smoking history or duration of exposure before onset of asthma. The only difference was that patients with persistent disease at follow-up had a significantly lower FEV1 and FEV1/FVC ratio at the initial visit, whereas NSBHR (histamine PC20) was similar in both groups.
Clinical characteristics of the patients
When comparing initial and follow-up assessments, cured subjects showed significant improvements in FEV1 from a median (IQR) value of 100 (96–104)% to 105 (97–107)% (p=0.04) and histamine PC20 from 1.4 (0.9–5.8) mg/mL to 17.0 (16.0–21.0) mg/mL, p<0.001. Subjects with persistent asthma also demonstrated a significant increase in histamine PC20 compared with baseline values from 1.2 (0.4–2.6) mg/mL to 4.7 (1.7–7.5) mg/mL (p=0.002), while FEV1 remained unchanged.
mDCs from patients with persistent asthma induce Th2 responses upon allergen pulsing
The capacity to polarise T cell responses was used as read-out for mDC functionality. DCs from cured versus persistent OA subjects were pulsed with the relevant allergen or with LPS as a control, washed and then cocultured for 5 days with allogeneic CD4+ T cells from (non-atopic) control donors.11 ,12 ,16
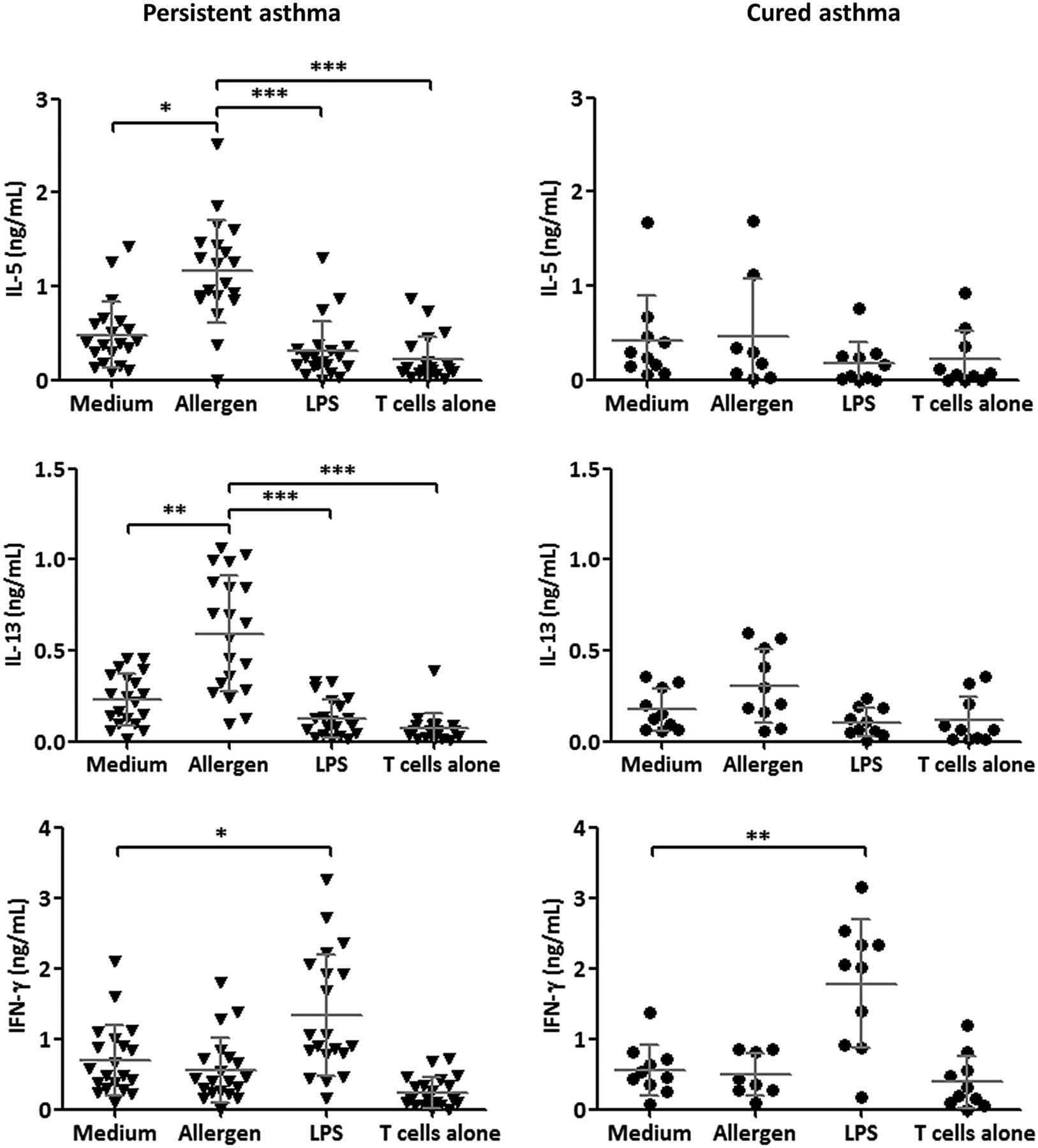
Upon allergen pulsing, mDCs from patients with persistent asthma upregulated IL-5 (from 0.4 (0.2–0.6) ng/mL to 1.1 (0.9–1.4) ng/mL, median (IQR), p<0.001) and IL-13 (from 0.2 (0.1–0.4) ng/mL to 0.6 (0.3–0.9) ng/mL, median (IQR), p<0.001) secretion by CD4+ T cells, whereas mDCs from cured patients did not affect these cytokines (figure 1). LPS-activated mDCs induced the production of interferon γ in both groups (figure 1), while no difference was observed for IL-9 and IL-10 (see online supplementary figure S1).

Cytokine production after 5 days of coculture between myeloid dendritic cells (mDCs) and allogeneic CD4+ T cells. Allergen-pulsed mDCs from patients with persistent asthma induce interleukin (IL) 5 and IL-13 production by allogeneic CD4+ T cells. LPS-pulsed mDCs from both groups induce significantly higher levels of interferon γ in the coculture. Statistics: Kruskal-Wallis multiple comparison test followed by Dunn's multiple comparison test (*p<0.05; **p<0.01; ***p<0.001).
To investigate whether upregulation of IL-5 and IL-13 was allergen-dependent, the same coculture experiments as for figure 1 were performed in eight patients with persistent asthma who were sensitised to the latex allergen Hev b 6.02. When their mDCs were pulsed with this recombinant allergen, the induction of IL-5 (from 0.5 (0.3–0.6) ng/mL to 1.0 (0.9–1.4) ng/mL, median (IQR), p<0.001) and IL-13 (from 0.3 (0.1–0.4) ng/mL to 0.7 (0.4–0.9) ng/mL, median (IQR), p=0.01) was similar to that observed with the complete latex extract (figure 2).

Interleukin (IL) 5 and IL-13 production is allergen-dependent: myeloid dendritic cells from patients with persistent asthma, allergy to latex and sensitisation to Hev b 6.02 were pulsed with latex extract or Hev b 6.02 allergen. The latex extract and recombinant Hev b 6.02 were able to induce the secretion of IL-5 and IL-13 by CD4+ T cells in the coculture. Statistics: Kruskal-Wallis multiple comparison test followed by Dunn's multiple comparison test (*p<0.05).
Upregulation of PD-L2 upon allergen pulsing of mDCs in persistent asthma
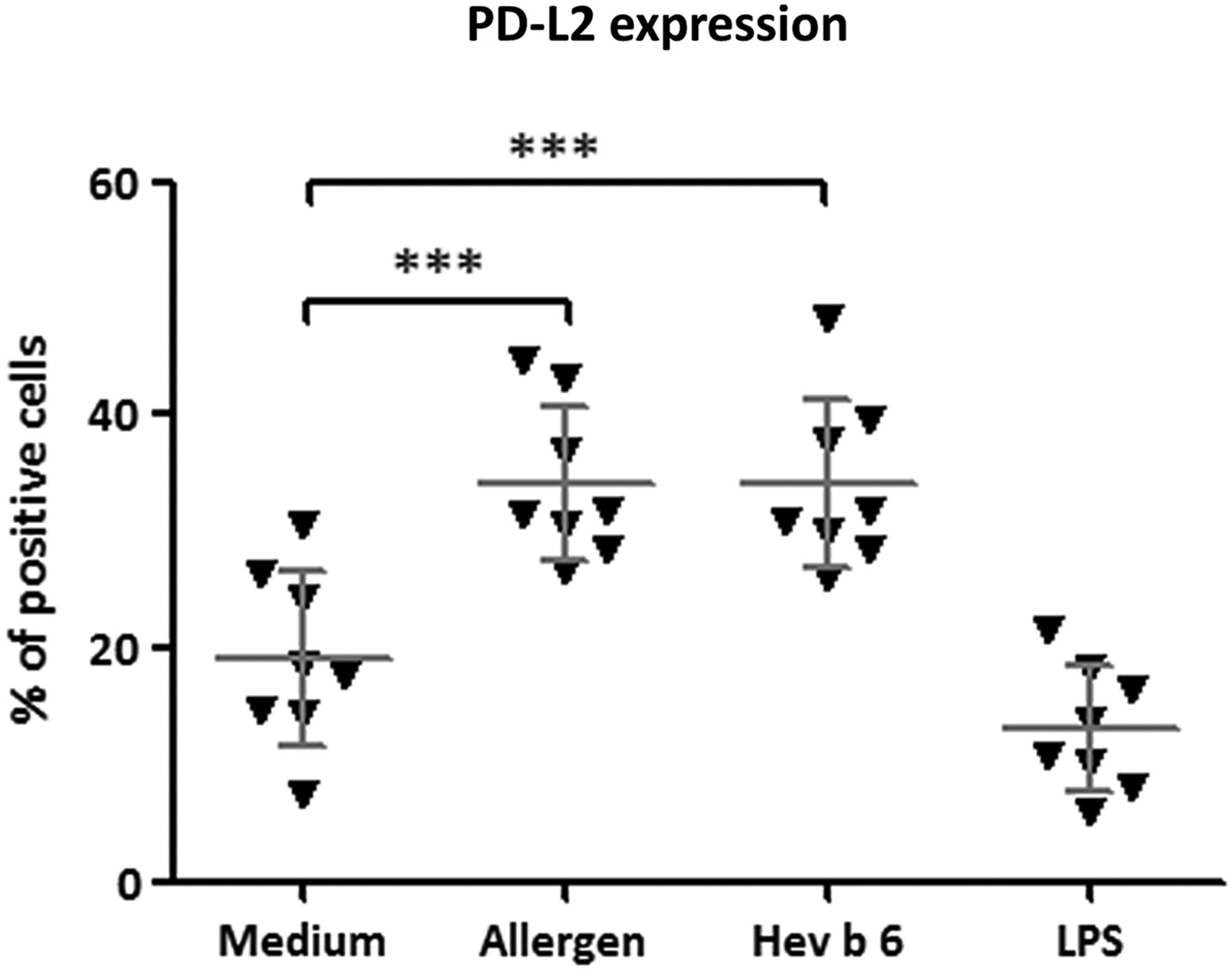
Type 1 mDCs were defined as CD1c+CD11c+HLA-DR+ Lin1 (CD3, 14, 19, 56)− cells (see online supplementary figure S2A). At baseline, the expression level of the costimulatory molecules CD80, CD86, PD-L1 and PD-L2 was not significantly different between mDCs from patients with persistent or cured asthma (see online supplementary figure S2B). However, upon in vitro stimulation with the relevant allergen extract (ie, flour or latex), mDCs from patients with persistent asthma upregulated the surface expression of PD-L2 (figure 3) (from 21.9 (15.4–29.4)% to 34.2 (29.2–41.0)%, median (IQR), p=0.003), in contrast to the mDCs from patients with asthma recovery (from 22.8 (20.4–33.2)% to 27.9 (20.5–32.8)%, median (IQR), p=0.3). Upon allergen stimulation, no change was observed for the costimulatory molecules CD80, CD86 and PD-L1 (data not shown).

Programmed death-ligand 2 (PD-L2) expression on myeloid dendritic cells from patients with persistent asthma is increased after exposure to allergen extract. Statistics: Kruskal-Wallis multiple comparison test followed by Dunn's multiple comparison test.
We then performed similar experiments on mDCs from patients with persistent asthma who were sensitised to the allergen Hev b 6.02. When using the recombinant allergen, the effect observed on PD-L2 expression was similar to what was obtained with the allergen extract: proportion of PD-L2+ mDC rose from 18.1 (14.4–25.9)% to 31.5 (28.9–41.4)% and to 31.2 (28.8–39.0)% (median (IQR), p<0.001 when pulsed with allergen extract and Hev b 6.02, respectively (figure 4).
Programmed death-ligand 2 (PD-L2) expression on myeloid dendritic cells from patients with persistent asthma and sensitised to latex is increased after exposure to recombinant allergen Hev b 6.02. Statistics: Kruskal-Wallis multiple comparison test followed by Dunn's multiple comparison test.
Th2 programming by mDCs from persistent patients is reversed by exogenous IL-12 or PD-L2 blockade
Seven patients with persistent asthma (four sensitised to flour and three sensitised to latex) gave their consent to undergo a second leukapheresis. The online supplementary table S1 provides the characteristics of patients selected for this set of functional experiments. To explore PD-L2 upregulation as an underlying mechanism of Th2 priming upon allergen pulsing of mDCs from patients with persistent disease, a blocking antibody against human PD-L2 was added in the cocultures (figure 5), blocking PD-L2 during the coculture led to a strong (∼75%) decrease in the production of IL-5 (from 1.4 (0.9–1.5) ng/mL to 0.5 (0.4–0.7) ng/mL, median (IQR)) and IL-13 (from 0.8 (0.6–0.9)) ng/mL to 0.3 (0.2–0.3)) ng/mL, median (IQR)), whereas control mouse IgG had no effect. The flexibility of Th2 programming by mDCs from patients with persistent disease was studied upon addition of exogenous IL-12 p70, which could abolish IL-5 and IL-13 production in this model (0.05 (0.02–0.09) ng/mL, median (IQR) for IL-5 and 0.03 (0.02–0.08) ng/mL, median (IQR) for IL-13).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Programmed death-ligand 2 (PD-L2) mediates Th2 cytokine induction by myeloid dendritic cells (mDCs) from patients with persistent asthma. Blocking antibody against PD-L2 inhibited about 70% of interleukin (IL) 5 and IL-13 production by mDCs from seven patients with persistent asthma, unlike control murine IgG. Addition of IL-12p70 in the coculture completely abolished IL-5 and IL-13 production. Statistics: Kruskal-Wallis multiple comparison test followed by Dunn's multiple comparison test.
Discussion
This study shows that mDCs from patients with asthma and persistent disease despite avoidance of the causal allergen display proTh2 features, being able to induce the Th2 signature cytokines IL-5 and IL-13 in allogeneic CD4+ T cells, and upregulating the costimulatory molecule PD-L2 upon allergen pulsing. In addition, the Th2 programming (induction of IL-5 and IL-13 production by T cells) is flexible in vitro upon addition of exogenous IL-12 and partly dependent on PD-L2. To our knowledge, these findings represent the first direct evidence of a relationship between DC functionality and asthma persistence in man.
Longitudinal studies looking at the outcome of asthma were based on self-reported symptoms and questionnaires and used variable definitions of asthma remission.17 ,18 In particular, most did not take the possible persistence of NSBHR into account, although this salient feature of asthma frequently persists despite symptomatic improvement.19 In this study, we used a strict definition of asthma remission based on the absence of symptoms and medication use, and, more importantly, on the resolution of NSBHR to histamine. In our population of subjects with OA due to flour and latex, the proportion of those with persistent NSBHR (66%) after cessation of exposure for a median of 8 years was similar to what has been reported in previous systematic reviews on the outcome of OA.3 ,20 In addition, we found that the persistence of asthma was associated with a significantly lower FEV1 and lower FEV1/FVC ratio at baseline, suggesting that the severity of airway obstruction at the time of the diagnosis is burdened with an increased risk of persistent disease, as reported in population-based cohort studies.17 ,21 In contrast, other features such as duration of symptoms before allergen avoidance failed to predict the outcome, as previously observed.3
Little attention has been given to the mechanisms leading to asthma remission,22 probably because current therapies are not able to induce such an outcome, with the exception of allergen immunotherapy in very selected patients.23 Moreover, the lack of a proper experimental model makes it difficult to explore the mechanisms underlying disease remission,22 particularly in humans. In 2004, Maghni et al4 correlated sputum inflammatory markers with disease outcome in patients with OA who were no longer exposed to the causal allergen. They showed that lack of improvement in BHR was linked to the presence of persisting inflammatory features in sputum, including higher eosinophil and neutrophil counts, as well as a higher concentration of myeloperoxidase and IL-8. Furthermore, a greater impairment in lung function at baseline and a longer time lapse since diagnosis were both risk factors for asthma persistence. Recently, another group explored immunological features in subjects with complete remission of asthma (no symptoms and no NSBHR), clinical remission of asthma (with ongoing NSBHR), or ongoing mild asthma, as well as non-asthmatic controls. No difference was found between ‘complete remission’, ‘clinical remission’ and ‘ongoing asthma’ groups regarding sputum eosinophil and neutrophil counts.24 As compared with controls, all asthmatic groups had significantly higher blood IgE and eosinophils, even those with ‘complete remission’. In addition, no difference was found in the number and function of blood regulatory T cells between these asthma groups. The authors speculated that the persistence of low suppressive T reg numbers in asthma might constitute a risk factor for relapse in the ‘complete remission’ group. Thus, no study has so far identified a specific cell type involved in asthma remission.
Standing at the crossroad between innate and adaptive immunity, DCs are able to skew immune response through cytokine secretion and costimulatory molecules. For instance, the OX40 ligand is a pro-Th2 signal induced by thymic stromal lymphopoietin stimulation,16 whereas immune costimulator expression on DCs seems protective for asthma by promoting regulatory T cell generation.25 In the present study, we show that allergen pulsing of DCs from patients with persistent asthma induces the upregulation of PD-L2. PD-1 family includes PD-L1 (also named B7-H1), expressed by B cells, DCs and T cells, PD-L2 (B7-DC), expressed by DCs and macrophages, and PD-1, expressed by T cells and other lymphoid cells.26 PD-1 signalling blocks T cell clonal expansion by inhibiting phosphatidylinositol-3-kinase and Akt activation.26 However, although PD-L1-driven inhibition is largely documented, notably in cancer immunity,27 the precise role of PD-L2, the other ligand for PD-1, remains elusive since studies on PD-L1 and PD-L2 pathways in murine asthma resulted in conflicting results. Whereas both molecules upregulate upon challenge,28 Akbari et al9 showed that PD-L1−/− mice had reduced BHR, while PD-L2−/− mice were protected against ovalbumin-induced experimental asthma. Recently, Lewkovitch et al demonstrated that a high PD-L2 expression on lung mDCs in humans correlated with disease severity8 and peaked in mice around 24 h post challenge while PD-L2 (and not PD-L1) blockade resulted in decreased NSBHR and inhibition of IL-13-induced gene expression. However, as PD-L2 blockade failed to inhibit Th2 cytokine expression, the authors postulated about unidentified ligand(s) to PD-L2 that might have different effects. In addition, viral infections, that represent a classical risk factor for asthma,29 also trigger upregulation of PD-L1, PD-L2 and OX40-L on airway DCs in mice,30 and this correlated with inflammatory cytokines in bronchoalveolar lavage (BAL). Our data show that allergen stimulation upregulated PD-L2 on human mDCs. Interestingly, this response was selectively observed in DCs from patients with persistent OA, and PD-L2 blockade could almost completely abrogate DC-driven IL-5 and IL-13 production in vitro by allogeneic CD4+ T cells. Therefore, the PD-L2/PD-1 axis could represent a pro-Th2 pathway involved in human asthma.
The molecular mechanisms underlying persistent abnormal DC function and asthma, however, remain elusive. A possibility is that patients with more severe airway disease at the onset display sustained cellular changes due to epigenetic modifications of Th2-related genes. A second hypothesis is that environmental factors independent from the culprit antigen, such as bacterial superantigens, directly maintain DC activation31 and ‘take over’ the allergens following avoidance of exposure. However, no change in costimulatory molecule expression has been reported upon DC stimulation by superantigens. Also, although these data provide potential mechanisms involved in asthma recovery, some limitations should be considered. First, the design of the study did not allow to determine at which time point those differences in mDC biology occurred since the mDCs were not assessed before cessation of exposure. Prospective studies, starting from the time of OA diagnosis, should be conducted in the future to address this issue. These studies should also take into account other potential confounding factors, such as the potential effects of intermittent occupational or even non-occupational exposures to the causal allergens and the effects of environmental exposure to ubiquitous allergens in atopic subjects on the outcome of asthma. It is, however, very unlikely that such exposures may have significantly affected the outcome of asthma in this population of subjects since the participants were carefully questioned and those who reported repeated exposures were excluded from the study. Also, the proportion of atopic subjects was similar among the participants with cured and persistent asthma. In addition, a recent systematic review of existing evidence failed to document any effect of atopic status on the outcome of OA.32 Second, only blood mDCs were studied; although several studies indicate a link between systemic and local DCs,33 ,34 it is likely that blood DCs only partly reflect airway DCs, due to the absence of mucosal factors potentially involved in DC regulation within the bronchial mucosa.35 Third, while OA represents a very interesting model, it remains uncertain whether findings could be extrapolated to allergic asthma driven by common allergens.
In conclusion, our findings show that in subjects with IgE-mediated asthma driven by occupational allergens, the disease outcome (persistence vs remission) is associated with distinct phenotypical and functional features of blood mDCs. mDCs from patients with persistent disease are imprinted with the aberrant capacity to induce Th2 cytokine responses in vitro. In addition, they upregulate, upon allergen pulsing, the expression of PD-L2, which partially mediates this pro-Th2 activity. Therefore, these data contribute to unveiling immune mechanisms involved in asthma remission in man, pointing to PD-L2 as the key molecule promoting persistent Th2 immunity in this disease. Whether targeting this pathway could promote improvement, and potentially remission, in allergen-driven asthma needs further investigation.
Acknowledgments
The authors thank Professor C Hermans (Haematology Department, Cliniques universitaires Saint-Luc, Brussels) for his help with leukapheresis procedures, and Mss Lecocq and Mr B Detry (same group as the authors) for their excellent technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
Footnotes
OV and CP contributed equally.
Contributors CP had full access to all the data and assumes responsibility for the integrity and accuracy of the data analysis. AF participated in the study design, performed the in vitro experiments, contributed to data collection, interpretation and analysis, and wrote the manuscript. VD and GE recruited patients and performed clinical and physiological evaluations. OV and CP designed the study, supervised experiments, contributed to data interpretation and analysis, as well as writing and reviewing of the manuscript.
Funding AF is funded by the Fondation Saint-Luc, Cliniques universitaires Saint-Luc and Fondation de Vooght, Université catholique de Louvain (UCL), Belgium. OV, VD, and GE were funded by the Fondation Mont-Godinne. CP is postdoctoral specialist of the Fonds National pour la Recherche Scientifique (FNRS 1.R.016.14), Belgium, and of the institute for Walloon Excellence in Lifesciences and Biotechnology (WELBIO CR-2012S-05). This work was supported by a grant (FRSM 3.4522.12) of the Fonds National pour la Recherche Scientifique (FNRS), Belgium.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol was approved by the Ethical committees (approval numbers 2008/27AOUT/234 and B039201213297).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves