Article Text

Statistics from Altmetric.com
Case report
A 26-year-old woman presented with a history of chronic progressive dyspnoea and a non-productive cough. Her medical history revealed recurrent, unexplained pneumonias and treatment for anorexia nervosa. The patient was a lifelong non-smoker and she denied any use of toxic substances.
On examination, her vital signs were as follows: body mass index, 17.6 kg/m2; temperature, 38.4°C; heart rate, 102 beats/min; BP, 100/60 mm Hg; respiratory rate, 24 breaths/min; and oxygen saturation, 91% on 6 L/min oxygen by nasal cannula. On auscultation, decreased breath sounds were heard at the bases bilaterally.
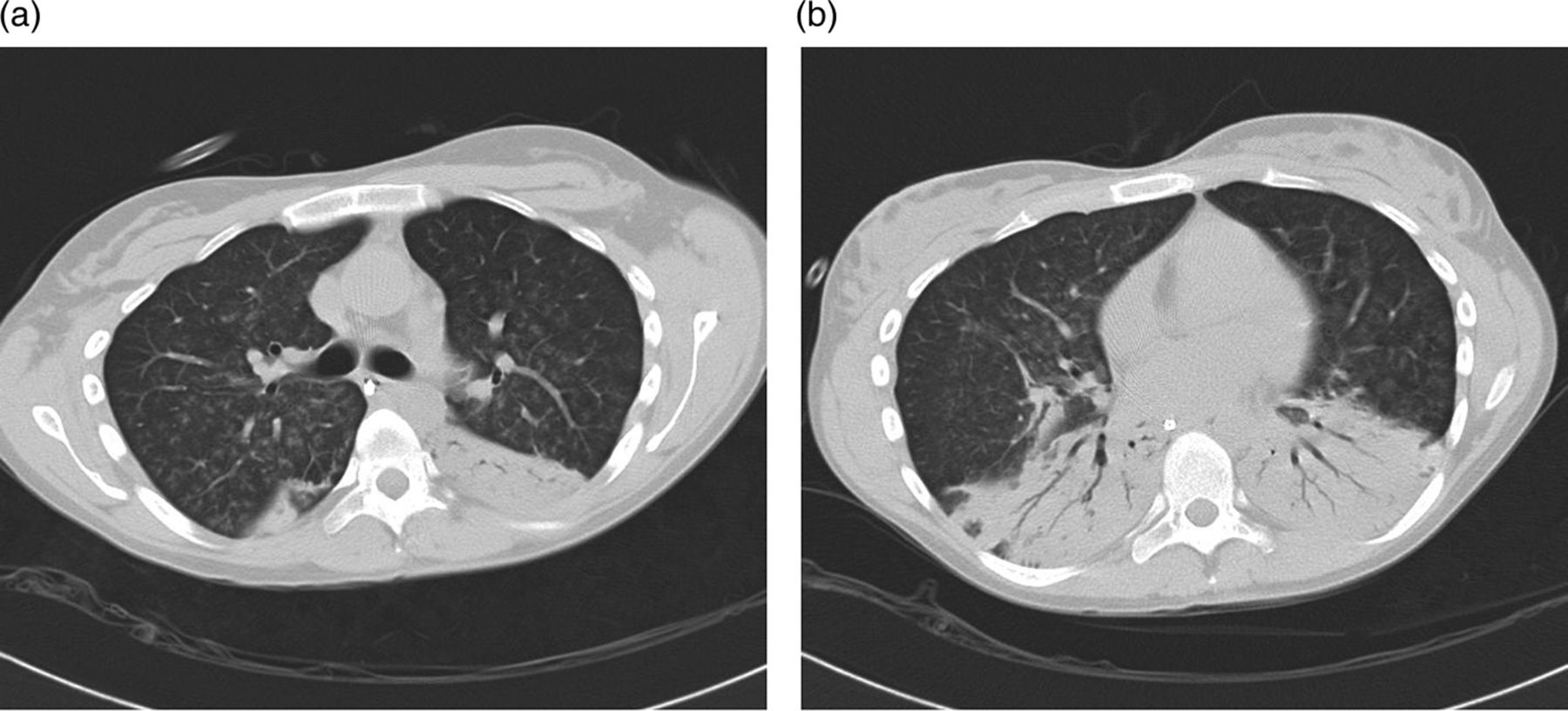
Blood testing for antinuclear antibodies was negative and immunological analysis demonstrated no immunodeficiency. Pulmonary function tests showed a restrictive pattern (total lung capacity: 3.72 L, 73% of predicted). A CT scan of the chest revealed bilateral consolidations with air bronchograms and a tree-in-bud-pattern (figure 1). A bronchoscopy showed a normal tracheobronchial tree. Bronchoalveolar lavage contained large numbers of neutrophils (99% neutrophils, 1% macrophages), and microbiological tests were negative for (myco)bacteria and fungi. Treatment with multiple antibiotics and steroids was ineffective. Subsequently a surgical lung biopsy was performed.

Images of the patient's HR-CT scan. (A) Image at the level of the main carina showing diffuse centrilobular nodules and tree-in-bud pattern. (B) Image through the lower lungs showing bilateral consolidation of the lower lung fields with air bronchograms.
Answer See page 198
Answer
From the question on page 193
What is the diagnosis?
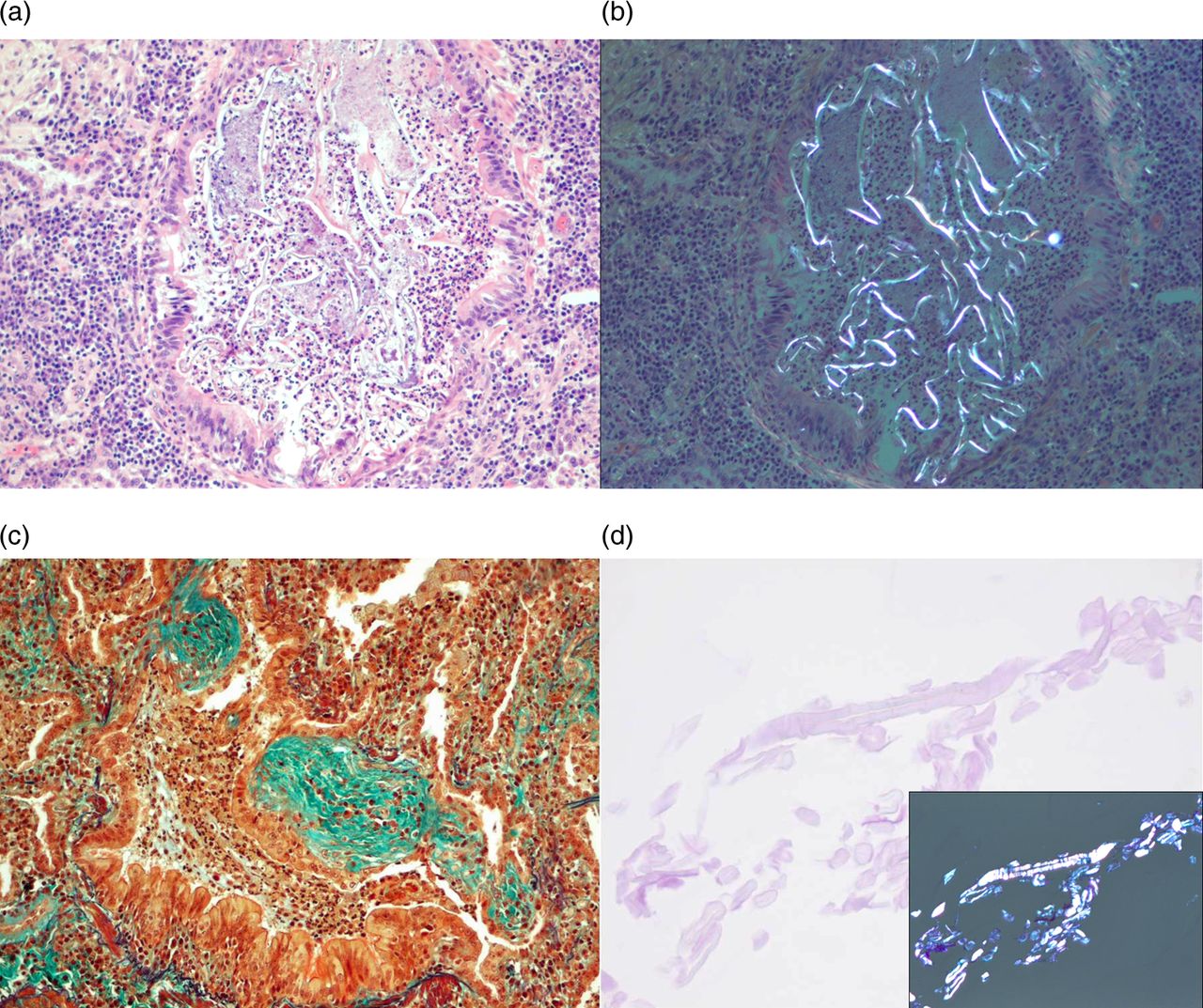
Pathological analysis of the biopsy revealed birefingent, fibrous material in the bronchioli surrounded by a neutrophilic and plasma cell–rich inflammation, microgranulomas with multinucleated giant cells (figure 2A–C) and foci of organising pneumonia. The differential diagnoses include fungal and mycobacterial infections, sarcoidosis, granulomatosis with polyangiitis, foreign-body granulomatous pneumonitis and talc granulomatosis.1 The presence of multinucleated giant cells in the background of organising pneumonia and the particulate matter within the bronchiole are diagnostic for a foreign-body granulomatous pneumonitis.2
{kind=link}
{kind=link}
Photomicrograph from the patient's surgical lung biopsy (A) Photomicrograph showing foreign body material within the lumen of the bronchiole surrounded by a neutrophilic and plasma cell–rich inflammation. Outside the lumen a poorly formed granuloma is seen (H&E stain, 100×) (B) Same section under polarised light showing the bronchioli are filled with birefingent material. (C) Foci of intraalveolar and intrabronchiolar plugs of collagen consistent with an organising pneumonia (EvM stain, 100×) (D) Histology of the patient's cottons swabs and paper tissues in light and polarising microscopy, matching the foreign body material found within the bronchiole (H&E stain, 200×).
Further questioning revealed that for more than 10 years, the patient had shown ritualised compulsive behaviour to clean her nose using cotton swabs and paper tissues. The consultant psychiatrist made a diagnosis of obsessive–compulsive disorder. Additional light microscopy of the patient's cotton swabs and tissues showed an identical morphology to the fibrous material found in the patient's lung tissue (figure 2D).
Cotton swabs and paper tissues mainly consist of cellulose. Chronic aspiration of cellulose may cause foreign-body granulomatous pneumonitis.2 Besides cellulose, other particulate material, such as talc, crospovidone, kayexalate, psyllium and green tea can also cause granulomatous pneumonitis.1–4 Additionally, cotton itself may cause airway-centered fibrosis, byssinosis and gossypibomas, all of which are distinctive from our case.5 We report a unique case of foreign-body granulomatous pneumonitis caused by aspirating cellulose fibres from cotton swabs and tissues in a patient with comorbid obsessive–compulsive disorder. Nasal deposition of cellulose, instead of gastroesophegeal reflux, causing aspiration pneumonitis has been described previously.4 We hypothesise therefore that the long-lasting period of excessive nasal cleaning led to the nasal deposition of cellulose fibres that were subsequently aspirated leading to a granulomatous pneumonitis.
The patient's condition improved after treatment for her obsessive–compulsive disorder. Sadly, she died unexpectedly a couple of weeks later. Autopsy revealed cotton fibres in the large airways and widespread granulomatous pneumonitis surrounding fibrous material, morphologically identical to the cotton swabs and paper tissues. No foreign body material was seen in the stomach.
Footnotes
-
Contributors Management of case: EAJEB, RCdB, ML-S, YFH. Literature search: SOS. Writing the article: SOS, EAJEB, RCdB, ML-S, YFH. Guarantor: YFH.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves