Article Text

Statistics from Altmetric.com
- GM-CSF autoantibody
- Opportunist lung infections
- Pulmonary alveolar proteinosis
- Bronchoscopy
- Imaging/CT MRI etc
Case presentation
A 76-year-old man, non-smoker, former bricklayer, was admitted to the Infectious Diseases Unit for cough and mild fever persisting for more than 1 month. The patient had no other significant medical problems and had not recently travelled abroad. There were no significant findings on physical examination.
Biochemical examinations showed an increase in inflammatory markers (CRP 7.9 mg/dl) and neutrophilic leukocytosis (14×109/l). Quantiferon test was negative, as were the autoimmune and the oncological markers. Nodular opacities were seen in both lungs on chest x-ray, and a subsequent CT scan showed multiple nodules located in all areas, but particularly in the subpleural location. Some of these nodules had features of cavitation. No ground-glass opacities were present (figure 1A). Mediastinal lymph nodes were slightly enlarged with a maximum diameter of 20 mm. Two ultrasound-guided percutaneous biopsies of the peripheral subpleural nodules were performed, with histological evidence of a suppurative inflammatory infiltrate with negative culture results. A bronchoscopy with bronchoalveolar lavage and transbronchial biopsy showed an intra-alveolar proteinaceous material and no microorganisms (figure 1B); microbiological cultures were also negative.

(A) Multiple parenchymal nodules with varying diameters primarily in subpleural areas with no signs of infiltration of the chest wall or pleural involvement. (B) Transbronchial biopsy showing intra-alveolar accumulation of granular eosinopilic material. H&E, 200×.
Which is the most probable diagnosis of the pulmonary nodules? ANSWER See page 1082
Answer
QUESTION See page 1078
Abstract
Pulmonary involvement due to Nocardia is generally associated with cell-mediated immunosuppressive conditions and risk factors like HIV infection, lymphoproliferative diseases, diabetes and steroid therapy. Pulmonary alveolar proteinosis (PAP) is a well-known risk factor for Nocardia infection and is usually easily detectable on a high-resolution CT scan as ground-glass opacities with geographical distribution, crazy paving pattern and varying amounts of pulmonary consolidation. Pulmonary nocardiosis should be considered in apparently immunocompetent patients who present with PAP and a suspected opportunistic infection. We report a case of pulmonary nocardiosis occurring in a patient with radiologically inapparent PAP. The serendipitous finding of PAP on transbronchial biopsy further increased the likelihood of a Nocardia infection, subsequently confirmed by a surgical biopsy.
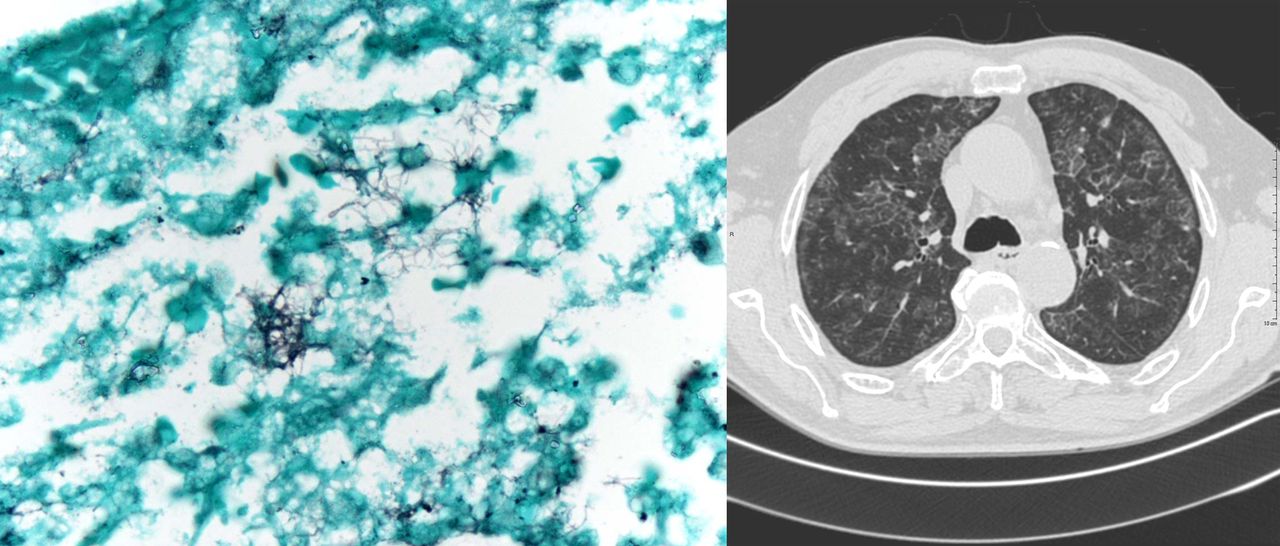
A multidisciplinary team evaluation attributed the bronchoscopic findings to a subclinical pulmonary alveolar proteinosis (PAP); for the undiagnosed pulmonary nodules, a surgical biopsy (video-assisted thoracic surgery) was requested. Grocott staining and culture were positive for Nocardia (figure 2A). The surrounding lung parenchyma showed small foci of PAP. The positivity of serum antibodies against granulocyte -macrophage colony stimulating factor confirmed the diagnosis of acquired autoimmune PAP.

{kind=link}
{kind=link}
(A) Surgical lung biopsy showing branching Grocott-positive filaments in an abscess. Grocott, 1000×. (B) Regression of parenchymal nodules described, with the appearance of ground-glass opacities with superimposed septal thickening (crazy paving) and geographical distribution.
Antibiotic therapy was started with an induction phase with amikacin (7.5 mg/kg once a day) and imipenem (500 mg four times a day) IV for 2 weeks and subsequent maintenance therapy with cotrimoxazole (10mg/kg/day) orally for 6 months. Follow-up CT scan showed a marked reduction in lung nodules, but the appearance of diffuse ground-glass areas with superimposed septal thickening and geographical distribution, typical of PAP (figure 2B).
Pulmonary nocardiosis is favoured by depressed cell-mediated immunity, for example, after transplantation, either in the presence of HIV infection, with haematological or solid malignancies, or in patients who receive prolonged treatments with corticoids or cytotoxic therapy.1 Local factors can be important as well, and Nocardia remains the most frequent opportunistic pathogen that infects the lungs in PAP patients.2
The possibility of pulmonary infection by Nocardia should immediately be considered in patients with a diagnosis of PAP. The presenting symptoms of pulmonary nocardiosis are non-specific, as is its radiological appearance, consisting in alveolar, nodular and cavitary lesions without a specific pattern of zonal distribution.3 On the other hand, high-resolution CT study of PAP usually shows more characteristic, albeit non-specific, signs.4 When the clinical suspicion of a nocardial infection is high, the healthcare professionals should inform the microbiology laboratory to optimise the isolation and identification of the microorganism. The high mortality rate of pulmonary nocardiosis is sometimes due to a delay in the appropriate treatment and to the variable antimicrobial susceptibility patterns, which require antimicrobial susceptibility test to assist decisions and prolonged treatment.5
In conclusion, we report a case of pulmonary nocardiosis occurring in a patient with radiologically inapparent PAP. The serendipitous finding of PAP on transbronchial biopsy further increased the likelihood of a Nocardia infection, subsequently confirmed by a surgical biopsy.
Acknowledgments
Thanks to Ms. Jacqueline Costa for language support, and to Ermanno Gabbi MD2 and Guido Menozzi MD2 for their assistance in the US evaluation of the transthoracic biopsies.
Footnotes
-
Contributors CC performed the bronchoscopy, conceived of the study, participated in its design and coordination and drafted the manuscript. FP performed the transthoracic biopsies and participated in the design of the study and in drafting the manuscript. EC performed the microbiological analysis and participated in the design of the study. AC performed the pathological analysis and participated in the design of the study. LS performed the radiological analysis and participated in the design of the study. GM participated in the design of the study and its coordination, and in drafting the manuscript. All authors have read and approved the final manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves