Article Text

Statistics from Altmetric.com
- ARDS
- assisted ventilation
- asthma
- COPD exacerbations
- tuberculosis
- lung cancer
- sarcoidosis
- occupational lung disease
- interstitial fibrosis
- bronchiectasis
- respiratory infection
- pneumonia
Case report
A 61-year-old non-smoking man, presented at our clinic with a 5-year history of chronic dry cough. He had undergone medication with antitussive agents for several years, but the drugs showed little therapeutic response. Chest radiographs did not show any apparent pulmonary parenchymal lesion, except for mildly higher density and irregularity over the tracheal border (figure 1A,B). CT scans showed diffuse submucosal calcified nodules protruding from the anterolateral portion of the trachea; the submucosal calcified nodules were absent in the posterior membranous portion of the trachea (figure 1C). CT virtual bronchoscopy showed numerous protruding nodules, which resembled stalactites with intact mucosa along the entire trachea (figure 2A,B). Multiple biopsies were performed using fiberoptic bronchoscopy (figure 2C), and the nodules were found to be firm and hard in consistency when grasped with the biopsy forceps. Pathological examination of the biopsied tissue showed chronic inflammation without any evidence of amyloidosis, granulomatous inflammation or malignancy. In addition, the tissue cultures of the bronchial biopsy sample and the cultures obtained from bronchial washings showed negative results. Hence, the evidence pointed towards a diagnosis of tracheobronchopathia osteochondroplastica.
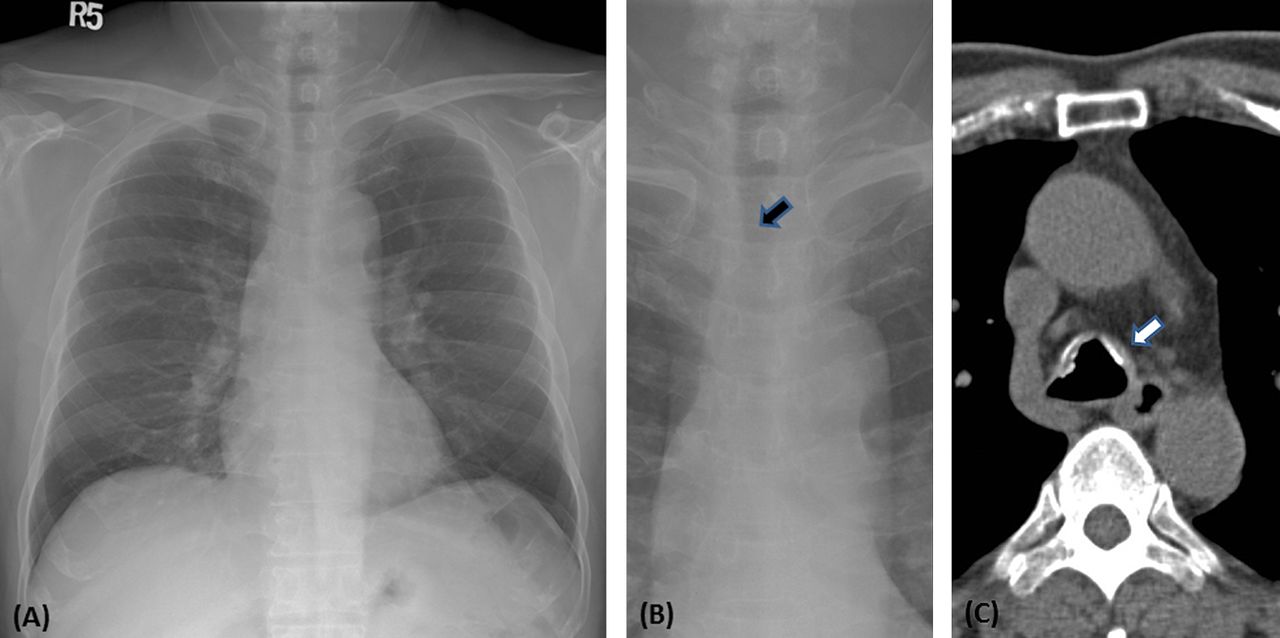
(A) and (B) Chest radiographs showing mild increasing density and uneven border of trachea (black arrow). (C) Chest CT scan showing multiple submucosal calcified nodules (white arrow) protruding from the anterolateral part of trachea while sparing the posterior membranous portion.

{kind=link}
{kind=link}
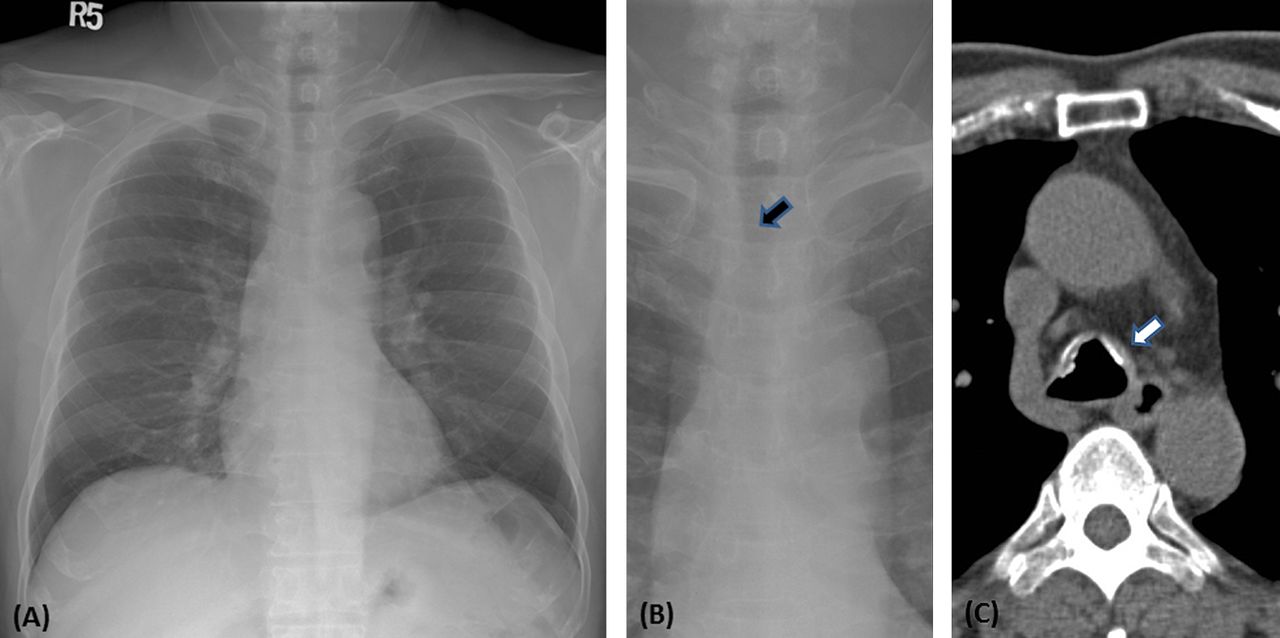
(A) and (B) CT virtual bronchoscopy showing numerous protruding nodules (stalactite-like or rock-garden-like) along the entire trachea that spare the posterior membranous portion of the tracheal wall (the white arrow indicates a line as a border between the anterior and posterior portions). (C) Fiberoptic bronchoscopy for biopsy showing numerous whitish submucosal nodules, which are compatible with the virtual bronchoscopy findings.
Learning points
-
Tracheobronchopathia osteochondroplastica (TPO) is a rare, idiopathic, slowly progressing disease of the trachea and major bronchi, which is usually characterised by recalcitrant cough, dyspnoea, wheezing and occasionally, haemoptysis.1
-
Characteristic chest CT scans in cases of TPO show multiple calcified nodules at the anterolateral wall of the trachea with typical sparing of the posterior membranous part.2 CT virtual bronchoscopy could also be used as a non-invasive tool to detect the typical manifestations of TPO, which resembles stalactites, or manifests with a rock-garden-like trachea.
-
Fiberoptic bronchoscopy should be considered in symptomatic patients with suspicious radiographic findings to confirm the diagnosis of TPO, and to exclude other conditions, such as amyloidosis, sarcoidosis, tuberculosis, relapsing polychondritis and malignancy.1 ,2
-
Treatment of TPO is usually symptomatic and surgical intervention or bronchoscopic laser therapy may be reserved for advanced cases with severe airway narrowing and airflow obstruction.1 ,2
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves