Article Text

Abstract
Objective To determine whether environmental control using nocturnal temperature controlled laminar airflow (TLA) treatment could improve the quality of life of patients with persistent atopic asthma.
Design Randomised, double-blind, placebo-controlled, parallel-group trial.
Setting Nineteen European asthma clinics.
Participants 312 patients aged 7–70 with inadequately controlled persistent atopic asthma.
Main outcome measure Proportion of patients with an increase of ≥0.5 points in asthma quality of life score after 1 year of treatment.
Results TLA devices were successfully installed in the bedrooms of 282 (90%) patients included in the primary efficacy analysis. There was a difference in treatment response rate between active (143 of 189, 76%) and placebo (56 of 92, 61%) groups, difference 14.8% (95% CI 3.1 to 26.5, p=0.02).3 In patients aged ≥12, on whom the study was powered, the difference in response rate was similar-active 106 of 143 (74%), placebo 42 of 70 (60%), difference 14.1% (0.6 to 27.7, p=0.059). There was a difference between groups in fractional exhaled nitric oxide change of −7.1 ppb (−13.6 to −0.7, p=0.03). Active treatment was associated with less increase in cat-specific IgE than placebo. There was no difference in adverse event rates between treatment groups.
Conclusion Inhalant exposure reduction with TLA improves quality of life, airway inflammation and systemic allergy in patients with persistent atopic asthma. TLA may be a treatment option for patients with inadequately controlled persistent atopic asthma.
Trial registration number Clinical Trials NCT00986323.
- Asthma
- exposure control
- temperature controlled laminar air flow
- protexo
- quality of life
- allergic lung disease
- paediatric physician
- paediatric asthma
- asthma pharmacology
- aspergillus lung disease
- copd mechanisms
- eosinophil biology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Asthma
- exposure control
- temperature controlled laminar air flow
- protexo
- quality of life
- allergic lung disease
- paediatric physician
- paediatric asthma
- asthma pharmacology
- aspergillus lung disease
- copd mechanisms
- eosinophil biology
Key messages
Can effective environmental control measures improve quality of life for people with asthma?
Treatment of patients with persistent atopic asthma for 1 year using nocturnal temperature controlled laminar airflow improved asthma-related quality of life and reduced airway inflammation.
Temperature controlled laminar airflow is a new technology which may be effective for treating patients with allergic asthma.
Introduction
In patients with atopic asthma, the abnormal immune response to inhalant allergens is an important contributor to symptoms.1 Studies undertaken at high altitude suggest that long-term avoidance of allergens and other exposures can lead to reduced asthma symptoms.2–6 Despite positive reports from comprehensive home environmental control programmes,7 blinded placebo-controlled studies of air filters and other single-device interventions have failed to demonstrate significant benefit, suggesting that the reduction in allergen exposure is insufficient to impact on airway inflammation.8 9 A new device Protexo (Airsonett, Ängelholm, Sweden) has recently been shown to markedly reduce levels of inhaled allergen and other particles using temperature-controlled laminar airflow (TLA) (personal communication, Dr Robin Gore, 2011). The device distributes a filtered cooled laminar airflow, descending from an overhead position, which displaces aeroallergens from the breathing zone. We undertook a phase III multicentre randomised controlled trial of nocturnal TLA treatment for 1 year to quantify the effect in patients with atopic asthma on quality of life, symptom control, lung function, airway inflammation and markers of systemic allergy (specific IgE and eosinophil count).
Methods
Participants
We enrolled patients with atopic asthma in a randomised, controlled, parallel-group trial of add-on treatment with TLA or placebo between April 2008 and February 2009. Patients were recruited from 19 European centres. Inclusion criteria were physician's diagnosis of asthma ≥1 year prior to study; age 7–70 years; Mini Asthma Quality of Life Questionnaire (mini-AQLQ) or Paediatric Asthma Quality of Life Questionnaire (PAQLQ) (together termed ‘AQLQ’) score ≤5.5 at inclusion; allergic sensitisation to a pet allergen (cat or dog) or house dust mite demonstrated by specific IgE level ≥0.70 kU/litre or positive skin prick test (weal diameter ≥histamine control); daily inhaled corticosteroid ≥200 μg/day budesonide/beclomethasone or ≥100 μg/day fluticasone for last 6 months; and features of partly controlled asthma according to Global Initiative for Asthma (GINA) 2006.10 Exclusion criteria were current active or passive cigarette smoke exposure; inclusion in another allergen avoidance programme or drug trial; treatment with allergen immunotherapy or omalizumab in previous 2 years (1 year for children); inhaled corticosteroid dose >1200 μg/day budesonide/beclomethasone or >1000 μg/day fluticasone. A history of frequent severe asthma exacerbations was not an inclusion criterion for the study. The study was approved by responsible institutional review boards and written informed consent was obtained from all patients/parents. An independent Data and Safety Monitoring Board reviewed efficacy and safety data.
Study intervention
Within 4 weeks from inclusion in the study, an active or placebo TLA device was installed in the bedroom of each study patient. The mode of action of the device is described in the online supplementary material. Patients were asked to turn their device on when they went to bed each night and off in the morning, although the device automatically turned off after 12 h. Placebo devices were identical to active devices, but their filter was bypassed and circulating air not cooled. Treatment compliance was assessed by an electronic counter within the machinery of the devices, which recorded total number of device uses, and total hours of use with the microcontroller MCU PIC18F6622 programmed by Voss Engineering AB, Sweden.
Randomisation and masking
Active or placebo treatment was allocated by the device installation technician according to a randomisation list generated by an independent organisation (APL, Stockholm, Sweden) using Design (Trombult Programming AB, Sweden) in blocks of nine at a ratio of two active to one placebo. The study protocol specified that randomisation would be stratified according to age and gender, but this was not done due to an error in communication with the independent study statistician. The planned stratification of randomisation was however taken into consideration during statistical analyses of outcome data. At the time of device installation and servicing the technician ensured patients and family members were absent from the bedroom and masking of treatment allocation was maintained. Patients, investigators, statisticians and the Trial Steering Committee were masked to treatment allocations through the study.
Trial design
The study was a phase III multicentre, double-blind, placebo-controlled, parallel-group trial. Patients were randomised to receive add-on treatment with Protexo or a placebo device for 1 year. Asthma medications were kept unchanged for the first 3 months, and thereafter adjusted to optimise asthma control by local investigators according to GINA guidelines.10 Patients were monitored by medical assessments after 1, 3, 6, 9 and 12 months of treatment, and via completion of a diary.
Outcome measures
The primary outcome measure was quality of life assessed by the mini-AQLQ, or in children ≤11 years, the PAQLQ.11 A change of 0.5 is considered clinically significant,12 and the primary outcome analysed was the proportion of patients with a significant increase in mini-AQLQ or PAQLQ score (‘responders’) after 1 year of treatment. Secondary outcomes were AQLQ score changes, objective measures of airway inflammation (fractional exhaled nitric oxide; FENO), systemic allergy (specific IgE levels to indoor aeroallergens and blood eosinophil count), and airflow obstruction (forced expiratory volume in 1 s, FEV1; forced expiratory flow at 50% of vital capacity, FEF50; peak expiratory flow, PEF). Single-breath, online measurement of FENO (NIOX MINO, Aerocrine AB, Stockholm, Sweden) was performed in accordance with the recommendations of the American Thoracic Society.13 Spirometry was performed in accordance with international guidelines.14 Blood eosinophil counts were measured by local hospital laboratories, and specific IgE levels using ImmunoCAP at a single laboratory (Phadia, Denmark; lower limit 0.35 KU/litre). The study was not designed primarily to evaluate effects of TLA on asthma exacerbations, because a history of frequent or severe exacerbations was not an inclusion criterion.
Statistical analysis
The study hypothesis was tested by examining the difference in outcome variables between active and placebo groups at the end of the 12-month treatment period. All patients who were randomised and had ≥1 day of device treatment were included in the intention-to-treat population and last observation carried forward was used for missing data. Per protocol analyses excluded patients with major protocol violations and/or documented treatment compliance <80%. Results were summarised as mean scores or score changes ±95% CI, or adjusted OR for binary outcomes ±95% CI. The country, gender, years since asthma diagnosis, GINA treatment step at baseline and AQLQ at baseline were variates in the model for adjusted analyses, which were undertaken using analysis of covariance (ANCOVA) for continuous data, and logistic regression for binary data. We calculated the sample size based on a minimum difference of 20% between treatment groups in the proportion of responders (increase in AQLQ ≥0.5 points over the 12-month intervention), and a responder rate of 20% in the placebo group. For 80% power and a type I error of 5%, the sample size needed is 186. Allowing for 20% loss to follow-up we planned to recruit 234 patients aged ≥12 years, and a proportionate number of patients aged <12. Planned subgroup analyses were undertaken by age, by asthma treatment intensity at baseline (GINA treatment step), for those with poor symptom control at baseline (Asthma Control Test; ACT<18) and for those with a combination of high-treatment intensity (GINA 4) and poor symptom control at baseline, where guidelines recommend stepping up treatment.15 16 An interim analysis was undertaken by the Data and Safety Monitoring Board after all participants reached 3 months, which included the primary outcome measure and safety. No action was taken after interim analysis as no safety issues were reported and early stopping criteria were not met.
Role of the funding source
Airsonett AB sponsored the trial. The Trial Steering Committee designed the study and statistical analysis plan. Data were analysed by an independent statistician Fredrik Hansson (Commitum AB). All authors had full access to data and analyses, and vouch for the report's accuracy and completeness.
Results
Three hundred and twelve patients from six countries were randomly allocated to treatment. Treatment groups had similar baseline demographic and clinical characteristics (table 1). Figure 1 shows the flow of patients through the study. A total of 282 of 312 (90%) randomised patients had a study device successfully installed in their bedroom, and were therefore eligible for primary efficacy analysis. Airborne particle counts and mattress dust allergen levels during the study are described in the online supplementary material.
Characteristics of study patients at baseline, presented as mean (SD) unless otherwise stated

Participant flow through the trial.
Effects of TLA on asthma-related quality of life
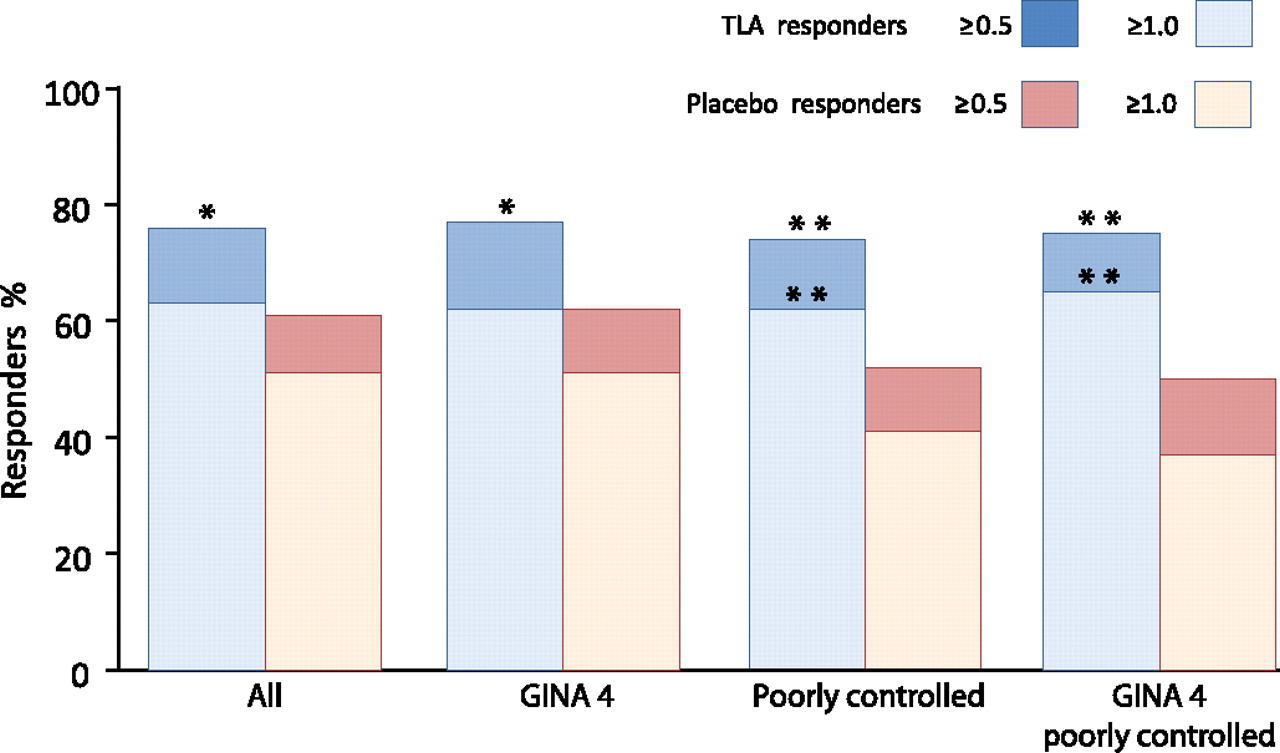
Primary efficacy analysis demonstrated a significant difference in AQLQ responder rate between active (143 of 189, 76%) and placebo (56 of 92, 61%) groups after 1 year—absolute difference 14.8% (95% CI 3.1 to 26.5, p=0.02; figure 2). Analysis of treatment response rate in participants aged ≥12 years (on whom the study was powered), showed a responder rate of 106 of 143 (74%) in the active group and 42 of 70 (60%) in the placebo group—absolute difference 14.1% (95% CI 0.6 to 27.7, p=0.059). In per protocol analysis the difference between treatment groups in responder rate was similar to intention-to-treat analysis, and there were differences of similar magnitude in children <12 when analysed separately, and in those with severe asthma at baseline judged by GINA-defined treatment intensity (table 2).10 The difference in responder rate was greatest in those with both high-treatment intensity (GINA 4) and poor symptom control (ACT<18) at baseline. Data were also analysed using a ≥1.0 point increase in AQLQ to define treatment response, and these showed similar findings to the analyses using the predefined responder definition of ≥0.5 points (figure 2). In analysis of treatment response rate without any imputation of missing data, a treatment response was seen in 129 of 166 (78%) in the TLA group at 12 months, and 50 of 79 (63%) in the placebo group—OR 1.87 (95% CI 1.05 to 3.34, p=0.03). There was a significant difference between groups in change in the symptom domain of AQLQ, with a mean 0.31 point (95% CI 0.01 to 0.61) greater increase after active versus placebo treatment; 0.70 points (95% CI 0.13 to 1.26) in the subgroup with high treatment intensity and poor symptom control at baseline. Figure 3 shows absolute values for changes in AQLQ in the total study population, and for those with highest treatment intensity (GINA 4; 46% of the study population), poor symptom control (ACT<18; 65%) or both (31%) at baseline. When analysed as a continuous variable we did not find a significant difference between treatment groups for AQLQ change in the total study population, but there was a significant difference in the subgroups with highest treatment intensity, poor symptom control or both.

Treatment response rate in patients treated with temperature controlled laminar airflow (TLA) or a placebo device for 1 year, defined as an increase in Asthma Quality of Life Questionnaire score of either ≥0.5 or ≥1.0 point. Data are shown for the total study population (n=282), those with high treatment intensity at baseline (Global Initiative for Asthma, GINA 4; n=129), poor asthma control at baseline (Asthma Control Test, ACT<18; n=184) or both (GINA4/ACT<18; n=87). *p<0.05, **p<0.01 relative to placebo.
Asthma-related quality of life in active and placebo groups after 1 year of treatment

{kind=link}
{kind=link}
{kind=link}
Change in Asthma Quality of Life Questionnaire (AQLQ) score during 1 year of temperature controlled laminar airflow (TLA) (blue line) or placebo (dotted red line) treatment in the whole population (All), those with highest asthma treatment intensity at baseline (Global Initiative for Asthma, GINA 4), those with poor asthma control at baseline (Asthma Control Test, ACT<18), or both (GINA 4, ACT<18). Values are mean ±1 SEM. Baseline AQLQ scores were similar in the TLA and placebo groups (total group mean 4.21 TLA, 4.25 placebo; GINA 4 mean 4.14 TLA, 4.14 placebo; ACT<18 mean 3.97 TLA, 3.92 placebo; GINA 4, ACT<18 mean 4.01 TLA, 3.85 placebo).
Effects of TLA on objective markers of bronchial and systemic allergy and lung function
TLA treatment was associated with a greater decrease in FENO during the study than placebo—mean difference −7.1 ppb (95% CI −13.6 to −0.7; p=0.03; table 3), which was of greater magnitude in patients with abnormally raised FENO (>45 ppb) at baseline (mean difference −29.7 ppb; 95% CI −47.2 to −12.2; p=0.001). There was no significant difference in blood eosinophil counts between treatment groups. We found a rise in cat-specific IgE levels relative to baseline level in the placebo group (mean 35%; 95% CI 18% to 53%) and a significantly smaller rise in the active group (mean 8%; 95% CI 0 to 17%; p=0.01; table 3). Lesser increases in levels of specific IgE to house dust mite and dog allergens were also seen in the active versus the placebo group, but the differences between groups were not statistically significant. There was no significant difference between groups in total IgE level change during the study, nor in measures of lung function FEV1, FEF50 or PEF (table 3).
Objective markers of bronchial inflammation and systemic allergy after 1 year of treatment
Effects of TLA on other asthma medication use and asthma exacerbation rates
Although this study was not primarily designed to evaluate TLA effects on asthma medication use or asthma exacerbation rates, medication use and exacerbations by treatment group are presented in online table S4. These data show relatively low rates of severe asthma exacerbations, no significant difference between groups in use of asthma medications and no significant difference between groups in asthma exacerbation rates.15 When exacerbation data were analysed according to predefined subgroups, there was no significant difference in rate of asthma exacerbations for the whole study population (mean 0.17 TLA; 0.24 placebo; p=0.50), for those with ACT<18 at baseline (mean 0.18 TLA; 0.34 placebo; p=0.28), for those with GINA 4 treatment intensity at baseline (mean 0.24 TLA; 0.40 placebo; p=0.23) or for those with both ACT<18 and GINA 4 at baseline (mean 0.23 TLA; 0.57 placebo; p=0.07).
Adverse events
In total, 153 (74%) patients in the active and 79 (75%) in the placebo group suffered an adverse event, and 32 (17%) patients in the active and 14 (15%) in the placebo group a serious adverse event. None were treatment related. Further details are given in the online supplementary material.
Discussion
Despite advances in asthma treatment, a significant number of patients have asthma that remains poorly controlled.17 Previous studies of allergen avoidance measures for treating asthma have been disappointing, leading the authors of a recent Cochrane systematic review of house dust mite control measures for asthma to comment ‘it is doubtful whether further studies… are worthwhile’.8 In this trial we investigated the effects of a novel treatment using nocturnal TLA in the homes of patients with atopic asthma. Contrary to previous studies, we found that exposure control using TLA treatment at night has an impact on overall asthma-related quality of life, with a significant difference in our primary outcome measure of AQLQ responder rate between active and placebo groups. The reason that nocturnal TLA is successful where so many other approaches have failed may be the profound reduction in inhaled aeroallergen exposure which this treatment achieves. The beneficial effects of TLA treatment on quality of life were not restricted to a specific age group of the study population, although when those aged ≥12 years (on whom the study was powered) were analysed alone, the effect of treatment was of borderline statistical significance. The treatment effect did appear to be greatest in patients with a combination of high asthma treatment intensity and poor asthma control, who represent a significant area of unmet need. Nocturnal TLA treatment also led to reduced airway inflammation measured by FENO, particularly in patients with abnormally raised FENO (>45 ppb) prior to treatment, and interestingly led to modified progression of some allergen-specific IgE compared with placebo. The lesser increase in cat allergen-specific IgE raises the intriguing possibility that nocturnal exposure control may lead to longer-term downregulation of allergic immune responses which has not previously been reported. Given the close relationship between allergen exposure, IgE sensitisation and airway inflammation, these data suggest that nocturnal TLA may work through exclusion of aeroallergens from the breathing zone.18 19 We did not find any effect of TLA treatment on measures of lung function such as FEV1 and PEF, and this is consistent with previous studies which showed that avoidance of aeroallergens can have beneficial effects on asthma symptoms and measures of airway inflammation without affecting lung function.4 7 This study was designed to evaluate the effect of TLA on self-reported quality of life, and the small numbers of patients with acute asthma exacerbations during the study limited our power to evaluate whether TLA treatment reduces exacerbation rates. The effects of TLA on quality of life and FENO are consistent with previous pilot work using TLA.20 The clinical effects of nocturnal TLA treatment appear to be applicable to a broad patient group, because our study population included a wide age range of patients sensitised to a variety of perennial allergens, recruited in six countries. Our inclusion criteria for the study were broad, and did not demand formal demonstration of variable airway obstruction—the trial results can therefore be generalised to settings where an asthma diagnosis is made without use of such criteria. It is however possible that treatment outcomes would differ in a group of patients with asthma included on the basis of meeting objective physiological criteria for airway obstruction or bronchial hyper-responsiveness. We found no evidence of a difference in treatment efficacy between children aged <12 and adolescents/adults. Although the treatment effect in those aged ≥12 was of borderline statistical significance, the effect size was similar to that seen in patients aged <12 and in the whole population. The difference in response rate between treatment groups in those aged ≥12 was not as large as the 20% difference which the study was powered to detect, perhaps due to the very high response rate in the placebo group. Overall our findings support other evidence that nocturnal exposures have a significant impact on inflammation and symptoms in asthma.21–23 This may be a consequence of circadian changes in autonomic function, steroid hormones and immune responsiveness. There is also persistent aeroallergen exposure at night, due in part to aeroallergen transfer to the breathing zone via body convection. Together with other studies of TLA, our findings suggest that the clinical effects of TLA can be explained by its ability to break the persistent body convection and thereby reduce aeroallergen exposure.
In conclusion we have demonstrated that nocturnal control of aeroallergen exposure using a novel non-pharmacological treatment TLA can improve quality of life and reduce airway inflammation in adults and children with atopic asthma, without significant adverse effects. Moreover the treatment limited rises in some aeroallergen-specific IgE levels, which have a close relationship with severity and persistence of asthma.18 19 24 Nocturnal TLA may be a treatment option for patients with uncontrolled atopic asthma despite high treatment intensity, where guidelines recommend stepping up treatment.10 Our findings support the importance of focusing exposure control interventions on the breathing zone, and highlight the role of nocturnal exposures in precipitating airway inflammation and symptoms in patients with atopic asthma.
Acknowledgments
We are grateful to the participants for their assistance in the conduct of this clinical trial.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Trial Steering Committee Professor Olof Zetterström (Chair), University Hospital of Linköping, Sweden; Professor Leif Bjermer, Lund University Hospital, Sweden; Professor Ronald Dahl, Aarhus University Hospital, Denmark; Professor Erkka Valovirta, Terveystalo Turku, Finland; Dr Andrea Von Berg, Marien Hospital, Germany; Professor John Warner, Imperial College London, UK; Professor Magnus Wickman, Sachs' Children's Hospital, Stockholm, Sweden.
Data and Safety Monitoring Committee Professor Jan Lötvall (Chair), Göteborg University, Sweden; Professor Stephen Durham, National Heart and Lung Institute, Imperial College London, UK; Fredrik Hansson, Commitum AB.
↵* 4A Study Group Members Robert Boyle, NIHR Biomedical Research Centre, Imperial College Healthcare NHS Trust and Imperial College London, UK; Christophe Pedroletti, Päivi Söderman and Björn Nordlund, Karolinska University Hospital Solna, Sweden; Per Tunqvist and Magnus Wickman, Sach's Children's Hospital, Sweden; Victoria Strand and Pär Gyllfors, Capio St Görans Hospital, Sweden; Janne Björkander, County Hospital Ryhov, Sweden; Leif Bjermer and Stefan Willers, Lund University Hospital, Sweden; Ann Hammarlund, Hospital of Ängelholm, Sweden; Bill Hesselmar and Nils Åberg, The Queen Silvia Children's Hospital, Sweden; Erkka Valovirta and and Heikki Valkama, Terveystalo Turku, Finland; Kai-Håkon Carlsen, Karin Lødrup Carlsen and Egil Bakkeheim, Ullevål University Hospital, Norway; Malcolm Sue-Chu, Trondheim University Hospital, Norway; Ronald Dahl, Aarhus University Hospital, Denmark; Vibecke Backer and Lotte Harmsen, Bispebjerg Hospital, Denmark; Claudia Gore, and Heather Hanna, Imperial College London, UK; Christian Virchow and Peter Julius, University of Rostock, Germany; Erika Von Mutius and Caroline von Ehrenstein, University of Munich, Germany; Andrea Von Berg and Christina Beckman, Marien-Hospital Wesel, Germany; Per Olof Wernersson, Allergimottagningen Karlstad, Sweden; Uwe Schauer, St Josef-Hospital Bochum, Germany; Olof Zetterström and Ulla Nyström Kronander, University Hospital of Linköping, Sweden; John Warner, NIHR Biomedical Research Centre, Imperial College Healthcare NHS Trust, and Imperial College London, UK.
Funding The study was funded by Airsonett AB. Robert Boyle was supported by a National Institute for Health Research Clinical Lectureship. John Warner is supported by a National Institute for Health Research Senior Fellowship. Robert Boyle and John Warner are supported by a National Institute for Health Research Biomedical Research Centre, and by the MRC and Asthma UK Centre in Allergic Mechanisms of Asthma.
Competing interests None.
Ethics approval Ethics approval was provided by responsible institutional review boards at each site in this multicentre international trial.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves