Article Text

Statistics from Altmetric.com
- Pulmonary physiology
- exercise
- imaging/CT MRI etc
- lung physiology
- bronchoscopy
- cough/mechanisms/pharmacology
- lung volume reduction surgery
Clinical presentation
A 64-year-old woman, never smoker, with a history of fully treated tuberculosis at 20 years of age attended our department for lung function testing. She had recently experienced several episodes of intermittent breathlessness and wheeze presumed to be due to asthma and was referred to a respiratory physician following an emergency department visit during one of these episodes. She did not have any recent weight loss, night sweats, purulent sputum or haemoptysis. Her dyspnoea and wheeze (inspiratory and expiratory) had been refractory to inhaled corticosteroids and both short and long acting β2 agonists.
Lung function using American Thoracic Society criteria1 (Sensormedics, Yorba Linda, California, USA) showed mild air flow obstruction with forced expiratory volume in one second (FEV1) of 1.67 l (82% predicted), forced vital capacity (FVC) of 2.92 l (120% predicted) and a FEV1/FVC ratio of 57%. Total lung capacity was normal (110% predicted). Her maximum flow-volume curves had a peculiar and reproducible appearance, particularly in the inspiratory phase (figure 1). There was no change following the use of a bronchodilator.
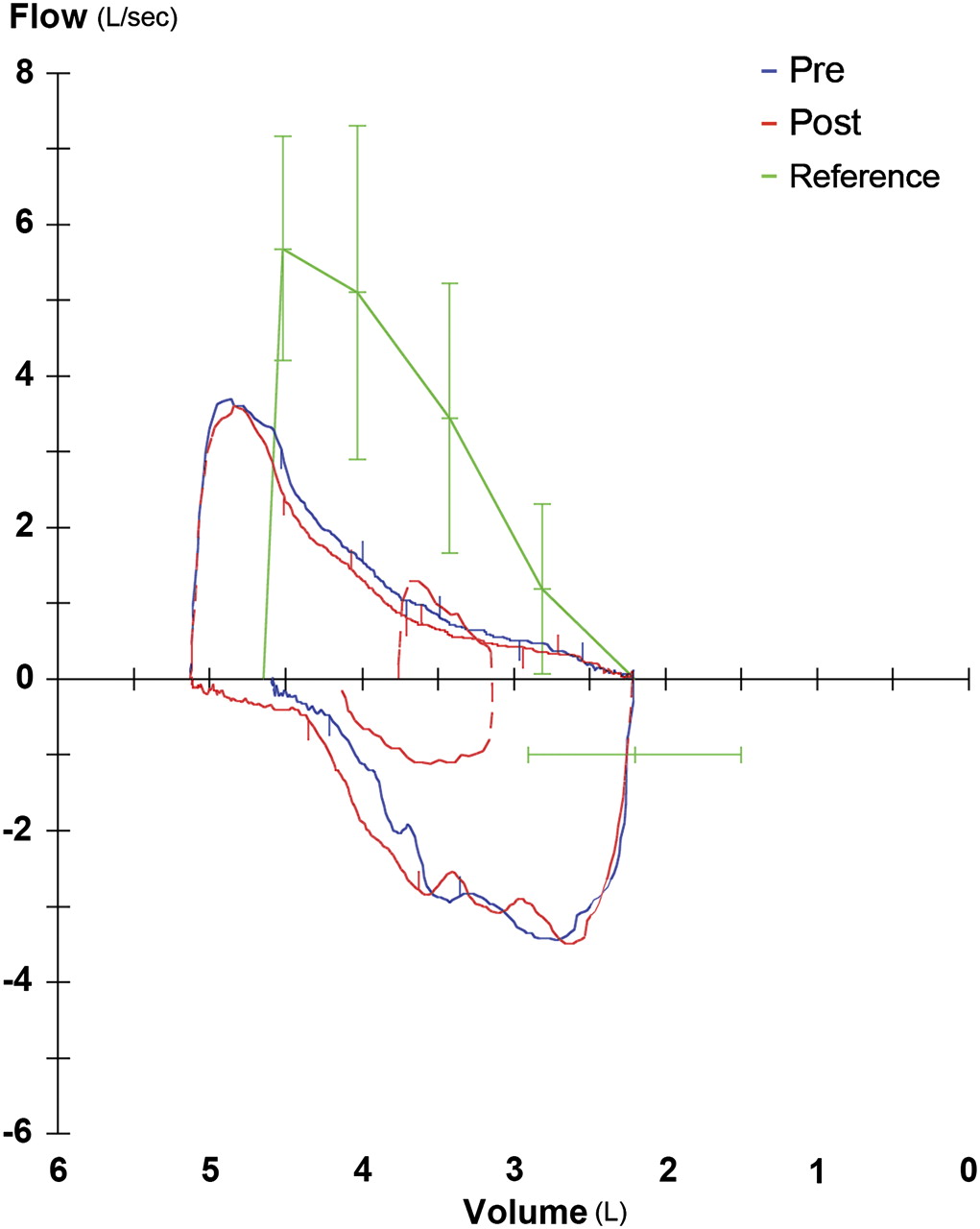
Maximal flow-volume loops before (‘Pre’) and after (‘Post’) bronchodilator. Reference lines (with SD bars) are linked to plethysmographic total lung capacity. There is a long expiratory tail with marked reduction in the end inspiratory flow.
Question
What is the diagnosis and which specific clinical sign might she have had?
See page 567 for the answer
Answer
From the question on page 564
Examination revealed a unilateral monophonic wheeze on the right. A CT chest showed severe narrowing of the right main bronchus (RMB) at its origin, confirmed at subsequent bronchoscopy, where a short segment stricture and web in the RMB stem were evident. Active tuberculosis and malignancy were excluded. The RMB web was resected using endobronchial laser therapy and then the bronchial orifice was dilated with a balloon dilator (figure 2).

Bronchoscopic images of main bronchi and carina taken (A) before and (B) after laser therapy (intervention 1).
Bronchial obstruction, however, remained evident on spirometry 3 months following the initial procedure and bronchoscopy revealed that the original stenosis had returned. This was treated with balloon dilatation (figure 3), and spirometry within 2 weeks of dilation is presented in figure 4. There was significant improvement in both inspiratory and expiratory flow-volume curves. Total lung capacity remained unchanged (108% predicted); however, FEV1 had normalised to 100% predicted with an improved FEV1/FVC ratio of 65%.

Bronchoscopic images of main bronchi and carina taken (A) before and (B) after balloon dilatation (intervention 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Maximal flow-volume loops following balloon dilatation. Reference lines (with SD bars) are linked to plethysmographic total lung capacity.
Discussion
The shape of the initial flow-volume loop is characteristic of ‘two compartment’ filling and emptying, where one lung is normal and the other severely obstructed. The ‘biphasic’ pattern reflects asynchronous filling and emptying of the affected lung. The normal lung dominates the early part of the curve, with the contribution of the slowly ventilated lung becoming evident in the second half of the manoeuvre.2 3
Causes of bronchial stenosis include tumour, single lung transplants, developmental anomalies such as cartilaginous rings and granulomatous disease.2 4 5
The expiratory spirogram may also be biphasic in bronchial obstruction. Constant flow from a fixed resistance becomes apparent as a straight line spirogram in later expiration, once emptying of the normal lung is virtually complete.2 Notably, we did not record this in our case.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Sydney Local Health District Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves