Article Text

Abstract
Introduction Improved nutrition is the major proven benefit of newborn screening programmes for cystic fibrosis (CF) and is associated with better clinical outcomes. It was hypothesised that early pulmonary inflammation and infection in infants with CF is associated with worse nutrition.
Methods Weight, height and pulmonary inflammation and infection in bronchoalveolar lavage (BAL) were assessed shortly after diagnosis in infants with CF and again at 1, 2 and 3 years of age. Body mass index (BMI) was expressed as z-scores. Inflammatory cells and cytokines (interleukin 1β (IL-1β), IL-6, IL-8 and tumour necrosis factor α (TNFα)), free neutrophil elastase activity and myeloperoxidase were measured in BAL. Mixed effects modelling was used to assess longitudinal associations between pulmonary inflammation, pulmonary infection (Staphylococcus aureus and Pseudomonas aeruginosa) and BMI z-score after adjusting for potential confounding factors.
Results Forty-two infants were studied (16 (38%) male; 39 (93%) pancreatic insufficient); 36 were diagnosed by newborn screening (at median age 4 weeks) and six by early clinical diagnosis (meconium ileus). Thirty-one (74%) received antistaphylococcal antibiotics. More than two-thirds were asymptomatic at each assessment. Mean BMI z-scores were −1.5 at diagnosis and 0.5, −0.2 and −0.1 at 1, 2 and 3 years, respectively. Neutrophil elastase and infection with S aureus were associated with lower BMI, whereas age (p=0.01) and antistaphylococcal antibiotics (p=0.013) were associated with increased BMI. On average, each log10 increase in free neutrophil elastase activity was associated with a 0.43 (95% CI 0.06 to 0.79) reduction in BMI z-score.
Discussion Early nutritional status is associated with the underlying pulmonary pathophysiology in CF, and better understanding of these relationships is required. Studies are required to assess whether interventions can decrease pulmonary inflammation and improve nutrition. Early surveillance will enable such targeted interventions with the aim of improving these important clinical outcomes.
- Bronchoscopy
- cystic fibrosis
- paediatric lung disaese
- respiratory infection
Statistics from Altmetric.com
Introduction
Cystic fibrosis (CF) is a common inherited condition that results in a shortened life span. Outcomes for those with CF have consistently improved over the last 40 years such that the median life expectancy is predicted to have reached 50 years for those born after 2000.1 Much of this improvement is due to aggressive treatment of pulmonary infections and closer attention to maintenance of nutritional status. Many countries have now incorporated newborn screening programmes for CF, and attention is focusing on improving quality and extent of life by earlier intervention in children.
Most of the morbidity and mortality in CF results from progressive suppurative lung disease.2 Bronchiectasis leads eventually to respiratory failure. Pulmonary inflammation starts early in infancy in those with CF and is exaggerated in response to pulmonary infection.3 Structural changes also occur much earlier in life than previously thought4 and, even though those diagnosed by newborn screening appear to have normal lung function during the first 6 months of life,5 bronchiectasis can be detected shortly after diagnosis.6 These data are important as they suggest preventing deterioration in lung structure and lung function requires targeted interventions towards improving respiratory health and nutrition as soon as possible after diagnosis, with monitoring of outcomes during the preschool years before pulmonary disease has become extensive.
We have developed a clinically based respiratory early surveillance programme for the detection of lung disease in infants and young children with CF that involves measurement of pulmonary inflammation and infection commencing soon after diagnosis in infants, usually prior to the development of symptoms. As improved nutrition is considered to be associated with better long-term outcomes in CF, and is the major proven benefit arising from newborn screening programmes, we aimed to describe the longitudinal course of pulmonary inflammation from diagnosis following newborn screening over the first 3 years of life and its relationship to the clinically relevant outcome of nutritional status. Specifically, we hypothesised that pulmonary inflammation in infants and young children with CF would be associated with lower body mass index (BMI).
Methods
Subjects
Infants and young children with CF were recruited from the CF clinic of the Princess Margaret Hospital for Children, Perth where an established newborn screening programme has existed since 2000.7 Briefly, this involves the measurement of immunoreactive trypsinogen from a heel prick test performed in the first 48–72 h of life.7 Those with immunoreactive trypsinogen >99th centile undergo cystic fibrosis transmembrane regulator gene mutation analysis. Infants are diagnosed with CF if they are found to be homozygous (or compound heterozygous) for known disease-producing mutations in the CF gene. Infants with one CF-associated gene are referred for sweat testing. Infants were included in the study if they were diagnosed with CF after 2000 by newborn screening, and/or had a positive sweat test. Infants with an early clinical diagnosis (<4 weeks) were also included. Infants were assessed shortly after diagnosis, then around the time of their first birthday and annually thereafter at 2 and 3 years of age. Each visit involved assessment of clinical and nutritional status and bronchoalveolar lavage (BAL). Clinic-recommended policy is for children to use amoxicillin clavulanate as antistaphylococcal prophylaxis during the first 2 years of life.
The surveillance programme was approved by the research ethics committee of The Princess Margaret Hospital for Children, Perth. Written consent was obtained from the parents of all participating subjects for use of clinical data and use of excess BAL and blood samples for research.
Clinical and nutritional data
Weight and crown–heel length were measured on the day of testing and expressed as weight, height and BMI z-scores using international growth reference data.8 A physical examination was performed by a clinician prior to bronchoscopy and BAL. Mode of presentation, genotype, current respiratory symptoms, antibiotic use since the previous assessment and all available microbiology results were reviewed and recorded.
Bronchoalveolar lavage
Flexible bronchoscopy was performed under general anaesthesia as previously described5 6 with a fibre-optic video-bronchoscope (Olympus XP160F) via an endotracheal tube or laryngeal mask as appropriate. Suction was not performed until the tip of the bronchoscope was past the carina. The BAL involved the instillation of 1 ml/kg of sterile normal saline per aliquot and was retrieved using low pressure suction. Three lavages were performed in the right middle lobe, and one in the lingula or most effected lobe on chest CT. The first sample from each side was sent for microbiological assessment, while the second and third samples from the right side were pooled and analysed for inflammatory markers following centrifugation for 5 min at 1500 rpm. The cell pellet was washed if required, resuspended in 1 ml of phosphate-buffered saline (PBS) and cell counts were conducted. A blinded observer then counted 300 cells and the proportion and number of neutrophils were recorded.9
Analysis of inflammatory mediators interleukin 1β (IL-1β), IL-6 and tumour necrosis factor α (TNFα) was conducted using a standard cytometric bead array human inflammation kit (BD Biosciences, San Diego, California, USA) with a working range between 20 and 5000 pg/ml. Analysis of IL-8 was completed using an ELISA (BD Opt EIA, BD Biosciences, San Diego, California, USA) with a working range between 0.01 and 6.40 ng/ml. Myeloperoxidase (MPO) was measured using an in-house ELISA as described previously.10
Free neutrophil elastase (NE) activity was assessed using an activity assay. BAL fluid supernatant was serially diluted 1:2 with Tris buffer in duplicate. Tris buffer was the negative control and human NE diluted to 25 μg/ml was the standard. The substrate N-methoxysuccinyl-ala-ala-pro-val p-nitroanilide (dissolved in N-methyl-2-pyrrolidinone (NMP)) was added to each well. Activity was read immediately at 405 nm. The plate was then incubated at 37°C in a CO2 incubator and read again at 20, 30 and 40 min. The results were calculated using AssayZap and the best time point was taken. The lower limit of detection for this assay was 0.2 μg/ml.
Microbiological samples were cultured on agar plates in the following manner: blood agar, cytosine lactose electrolyte-deficient agar, and blood agar + ticarcillin (for resistant Pseudomonas aeruginosa identification) then incubated at 35°C for 48 h in a CO2 incubator; a PC plate (selective plate for Burkholderia cepacia complex) was incubated at 35°C for 48 h in a CO2 incubator, then at room temperature for a further 24 h; mannitol salt agar for Staphylococccus aureus was incubated at 35°C for 48 h in an aerobic atmosphere; Sabarouds agar (for fungi isolation) was incubated at 35°C for 48 h, then at 28°C for a further 14 days; Fildes agar (for Haemophilus isolation) was incubated at 35°C for 48 h in an anaerobic environment (to prevent overgrowth by P aeruginosa). Bacteria were identified by colony morphology, Gram stain and biochemical tests including oxidase and the C390 screening test specifically for Pseudomonas. Microbiological results were reported as positive if at least 104 colony-forming units were identified per ml. Respiratory viruses (respiratory syncitial virus (RSV), parainfluenza 1, 2 and 3, influenza A and B, adenovirus and cytomegalovirus) were detected using direct immunoflourescence and/or rapid viral tissue culture.
Statistical analysis
Spearman rank correlation was used to assess bivariate cross-sectional associations between each measure of pulmonary inflammation and BMI z-score. For longitudinal analyses, age (in decimal years) was centred around the mean, and continuous variables were log10 transformed to approximate the normal distribution. Due to the small number of samples and incomplete follow-up data, linear mixed effects analysis, with random intercept for subjects, was applied to assess longitudinal associations between BMI z-score and measures of pulmonary inflammation. Models were also adjusted for age, gender, antistaphylococcal antibiotics and presence of symptoms. Linear mixed effects modelling was done in Stata version 10.0, and all other analyses were done through SPSS 15. For the analyses, values for 50% of the lowest limits of detection were substituted where pulmonary inflammation was undetected in BAL.
Results
Forty-two infants (16 (38.1%) male) were diagnosed with CF between the inception of newborn screening and February 2006. This period was chosen to allow for longitudinal data collected up to the age of ∼3 years to be included. Thirty-six of these were diagnosed by newborn screening (at median age 4 weeks) and six by early clinical diagnosis (all with meconium ileus diagnosed <4 weeks). Twenty-four (57%) were homozygous and 16 (38%) heterozygous for the Phe508del mutation, respectively. Thirty-nine (92.9%) infants were pancreatic insufficient. Parent-reported respiratory symptoms (cough, wheeze or any breathing difficulty) were present at the time of the assessments in 38, 36, 31 and 36%, respectively, of the 36 infants diagnosed by newborn screening. A total of 40, 77, 63 and 57% of infants, respectively, were receiving prophylactic antistaphylococcal antibiotics at assessment.
Nutritional indices
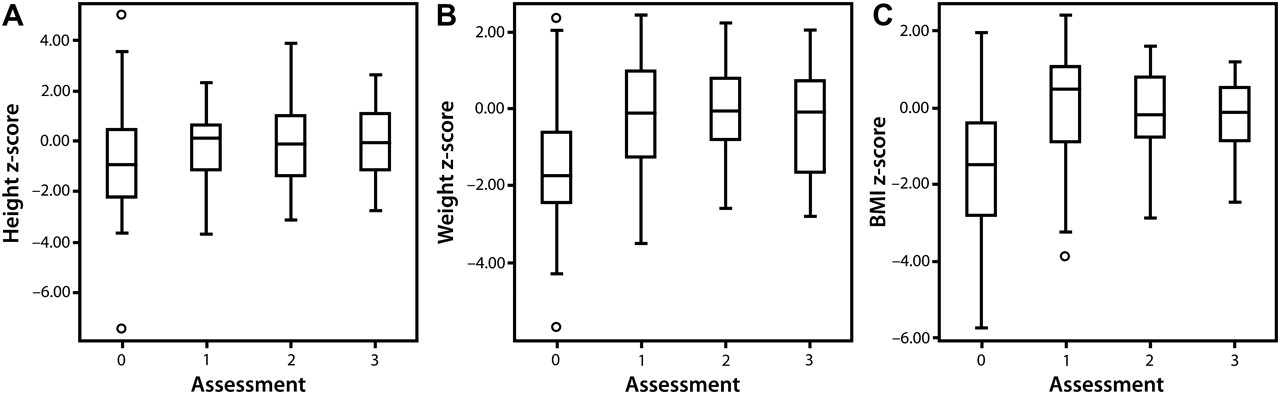
Height was well preserved during the course of the study. Median weight z-scores were reduced at diagnosis but increased and normalised during subsequent evaluations. BMI z-scores followed a similar pattern to weight z-scores (figure 1 and table 1).

(A) Height, (B) weight and (C) body mass index (BMI) z-scores measured soon after diagnosis and at 1, 2 and 3 years of age. The box and whiskers represent the median, IQR and range respectively.
Nutrition, inflammation and infection data
Association between pulmonary inflammation and BMI z-score
Pulmonary inflammation identified at each assessment is shown in table 1. Neutrophils were detected in all BAL samples. There were no obvious trends over time in the proportion of neutrophils in the BAL total cell population or in the number of neutrophils in the BAL. IL-1β, IL-6 and MPO were detected in most BAL samples and no obvious trend could be identified at the different assessments. NE was detected in approximately a third of BAL and less frequently than IL-8 which was detected in ∼80% of BAL (table 1). When detected, levels of NE increased over the first 2 years but then fell slightly at the final BAL, whereas IL-8 increased throughout the study (table 1 and figure 2).

{kind=link}
{kind=link}
(A) Log transformed interleukin 8 (IL-8; pg/ml) and (B) neutrophil elastase (ng/ml) measured soon after diagnosis and at 1, 2 and 3 years of age. The box and whiskers represent the median, IQR and range, respectively.
Significant correlations were seen between the different indices of neutrophilic inflammation: neutrophil number (and proportion), IL-8, NE and MPO. Thus, the effects of inflammation variables on BMI were examined individually. There was no obvious correlation between pulmonary inflammation and BMI z-score at any of the individual assessments (correlations shown for NE and IL-8 in table E1 of the online supplement). In longitudinal analyses (table 2), log10 neutrophil number, log10 IL-6, log10 IL-8, log10 MPO, log10 IL-1β and log10 TNFα were not significantly associated with reduced BMI z-score, whereas log10 free NE was associated with a lower BMI z-score (p=0.022). On average, each log10 increase in NE was associated with a 0.43 (95% CI 0.06 to 0.79) reduction in BMI z-score, as shown in table 2. Details of the full adjusted mixed effects model for the association between NE and BMI z-score is shown in table E2 of the online supplement.
Adjusted associations between measures of pulmonary inflammation and BMI z-score
Age (p=0.01) and treatment with antistaphylococcal antibiotic prophylaxis (p=0.013) had a significant positive association with BMI z-score, whereas gender, genotype and presence of symptoms were not associated with BMI z-score.
Association between pulmonary infection and BMI z-score
Apart from one infant in whom RSV was isolated, viruses were not detected in BAL. The known CF airway pathogens, S aureus and P aeruginosa, were the most commonly detected bacteria in BAL (table 1). Other organisms detected in the respective BAL were in the first BAL: Escherichia coli (n=1), Aspergillus fumigata (n=1), Haemophilus influenzae (n=1), Enterobacter cloacae (n=4), Klebsiella spp. (n=1); in the second BAL: A fumigata (n=1), H influenzae (n=1), E cloacae (n=1); in the third BAL: A fumigata (n=1), Moraxella catarrhalis (n=1), Stenotrophomonas maltophilia (n=1); in the fourth BAL: E coli (n=1), A fumigata (n=1), H influenzae (n=3), Klebsiella spp. (n=1).
A mixed effects analysis was used to evaluate the influence of pulmonary infection (S aureus and P aeruginosa) on BMI z-score after adjusting for potential confounders (table 3). Infection with S aureus was associated with a mean reduction of 1.04 z-score for BMI. No association was observed for infection with P aeruginosa (p=0.918). Thus, respiratory tract infection with S aureus identified in BAL was associated with lower BMI z-scores after accounting for age, gender and antistaphylococcal antibiotic prophylaxis.
Associations between pulmonary infection and body mass index (BMI) z-score
Infection with either S aureus (mean 0.39; 95% CI 0.12 to 0.66; p=0.004) or P aeruginosa (mean 0.78; 95% CI 0.460 to 1.09; p<0.001) was significantly associated with increased log10 free NE, but treatment with antistaphylococcal antibiotic prophylaxis was not (−0.021; 95% CI −0.226 to 0.185; p=0.842).
Discussion
Many countries in Europe and the majority of the USA have now adopted newborn screening programmes for CF. Improved nutritional status is an important clinical outcome in CF and is the most obvious benefit afforded by an early diagnosis from newborn screening. In the present single-centre study in infants and young children with CF diagnosed mainly by newborn screening we have shown that early pulmonary inflammation characterised by free NE and infection with S aureus are associated with worse nutritional status in the first few years of life, in the absence of clinically apparent respiratory disease in most children. This association was evident despite modern CF care that included an aggressive clinical approach to improving nutrition, apparent normalisation of nutritional status in the vast majority of subjects and treatment of any pulmonary exacerbations. The results of our study are crucial in informing future clinical practice if further benefits from newborn screening are to be realised.
Several studies have demonstrated that pulmonary inflammation is evident soon after diagnosis in CF, but the longitudinal nature of our study allowed us to investigate its relationship with BMI over the first 3 years of life. This is important as any relationship between pulmonary inflammation and BMI z-score is likely to be temporally complex. Assessment of inflammation in the BAL provides a single-time ‘snap-shot’ of the inflammatory processes occurring in the lungs. However, BMI provides a cumulative assessment of nutrition. Thus the lack of correlation between these at single time points is not surprising. BMI z-scores or percentiles have been shown to be a valid measure of nutritional status in CF and predict nutritional failure more sensitively and accurately than conventional anthropometric measures.11 12 In the post-screening era, where infants generally maintain normal height in contrast to children diagnosed following clinical presentation, we believe that BMI z-score can be used instead of other measures of nutritional status such as weight-for-height. However, more comprehensive measures of nutritional status such as measurement of body composition may provide a better insight into early nutritional status and should be considered for future studies. In older subjects, improved nutritional status has been shown to be associated with improved survival in those with CF.13 In childhood, increased BMI is associated with better lung function.14 Recent data from the Wisconsin group identified that patients with CF who achieved early growth recovery within 2 years of diagnosis had fewer cough symptoms, better lung function and better chest radiograph scores at 6 years of age, whereas growth patterns between the ages of 2 and 6 years were not associated with pulmonary measures at age 6.15 Their finding that benefits of newborn screening on pulmonary status at 6 years of age depend on early nutritional outcomes emphasises the need for comprehensive and aggressive treatment implemented as soon as possible after diagnosis. Thus, it is likely that improving BMI during the first few years of life could have further significant positive health benefits in later life for those with CF. Although treating fat malabsorption due to pancreatic insufficiency results in apparent normalisation of nutritional status in the majority, our study highlights the need to investigate the association between pulmonary inflammation and nutritional status further in order to find new strategies for optimising clinical outcomes.
We measured cytokines, cells and inflammatory products known to be associated with pulmonary disease in CF. We found that NE was significantly associated with a reduction in BMI even though it was detected in a small number of subjects. NE is a serine protease with broad target specificity. Free NE indicates that the antiproteinase mechanisms have been overwhelmed, exposing proteins associated with the basal lamina, extracellular matrix and cell-associated glycocalyxses to hydrolysation. We have shown previously that detection of free NE in the infant CF airway is associated with bronchiectasis.6 We also identified a significant association between NE and lower respiratory tract infection with S aureus. Whether interventions to suppress pulmonary inflammation improve early nutritional status remains to be determined. Few centres specifically target the neutrophil-dominated pulmonary inflammation of CF during the first few years of life. A number of non-specific anti-inflammatory treatments, for example macrolides, or specific treatments, such as inhibitors of NE, have been proposed. The results of the present study inform such potential studies and suggest that the BMI z-score may be useful as a practical outcome measure of response to early interventions.
Aggressive treatment of infections, in particular those due to P aeruginosa, has been shown to decrease pulmonary inflammation.16 We detected this organism in only four children and were limited in our ability to study such associations. Early detection and eradication of infection with P aeruginosa has become routine in many centres irrespective of symptoms. The small numbers of patients infected with P aeruginosa, the use of aggressive eradication and the possibility that the generally later acquisition of P aeruginosa compared with infection with S aureus were reasons why we were unable to show an association between infection with this organism and worse nutritional status in this study. While antipseudomonal strategies are clearly important, infection with S aureus is more common in infants, and efforts to treat this organism more aggressively need to be investigated. We identified a significant association between early lower respiratory infection with S aureus and worse BMI z-scores. Intravenous antibiotics in infants are associated with a reduction in pulmonary inflammation detected on BAL,17 but are not usually recommended for infection with S aureus in the absence of symptoms. Although it has become the standard of care in many centres to use orally administered prophylactic antibiotics against S aureus during the first year or more of life,18 this practice is not universal and its benefits have not yet been subjected to a systematic randomised control trial.19 In our study, treatment with antistaphylococcal antibiotics was associated with significantly better BMI, but we must emphasise that it was not specifically designed to test this association. While clinic policy was to use antistaphylococcal prophylaxis for the first 2 years of life, variations in prescribing these antibiotics were partly determined by the importance attached to this strategy by treating physicians and the willingness of parents and carers to administer long-term antibiotics to apparently well children. As we have shown that infection with S aureus is associated with both pulmonary inflammation and worse nutritional status, specifically designed studies are needed to determine whether a more aggressive approach of prevention, early detection and treatment of infection with this organism results in improvement in BMI and other clinical outcomes in the first years of life.
Surveillance bronchoscopy with BAL is not routine in CF, and so many would consider our approach to be rather invasive. As organisms such as S aureus may be found routinely in the upper airway even in healthy children without CF, we believe that BAL is the ‘gold standard’ technique for identifying this organism in the lower respiratory tract rather than reliance on upper airway microbiological samples, especially as infection with S aureus can occur in the absence of symptoms. Accurate and early detection of infection with S aureus is important, and so our results offer support for more routine use of BAL in pulmonary surveillance. Pulmonary inflammation can also occur in the absence of clinical symptoms or signs.20 To our knowledge there is no validated alternative to performing BAL for the detection of pulmonary inflammation in clinical practice in infants. Despite our more invasive approach, one limitation of our study is that we were only able to conduct BAL on a few occasions due to the requirement for general anaesthesia for this procedure. Thus, we can only provide a ‘snap-shot’ of the true relationship between infection, inflammation and nutritional status.
We conclude that pulmonary inflammation in infants with CF diagnosed by newborn screening is associated with worse nutritional status. Aggressive surveillance and controlled trials of targeted interventions in early life are required to better understand the relationships between pulmonary inflammation and nutrition. Studies are required to assess whether such interventions can improve clinical outcomes for those with CF.
Acknowledgments
We would like to thank all the families who kindly participated. The full authorship of this manuscript includes the members of AREST CF, who are listed below: Elizabeth Balding, Luke J Berry, Dr Siobhain Brennan, Professor John B Carlin, Rosemary Carzino, Professor Nick de Klerk, Dr Tonia Douglas, Clara Foo, Dr Catherine L Gangell, Luke W Garratt, A/Professor Graham L Hall, Dr Jo Harrison, Dr Anthony Kicic, Dr Ingrid A Laing, Karla M Logie, A/Professor John Massie, Dr Lauren S Mott, Dr Conor Murray, Faith Parsons, Dr Srinivas R Poreddy, A/Professor Sarath C Ranganathan, Professor Colin F Robertson, Professor Roy Robins-Browne, A/Professor Philip J Robinson, Billy Skoric, Professor Peter D Sly, Professor Stephen M Stick, Dr Erika N Sutanto and Dr Elizabeth Williamson.
References
Supplementary materials
Web Only Data thx.2010.139493
Files in this Data Supplement:
Web Only Data thx.2010.139493
Files in this Data Supplement:
Footnotes
Funding This study has been funded by grants from the US Cystic Fibrosis Foundation (SLY04A0 and STICK09A0), the National Health and Medical Research Council (3211912, #458513) and the Murdoch Children's Research Institute, Australia.
Competing interests None.
Ethics approval This study was conducted with the approval of the Princess Margaret Hospital Research Ethics Committee, Perth.
Provenance and peer review Not commissioned; externally peer reviewed.