Article Text

Abstract
Background: Sleep hypoventilation has been proposed as a cause of progressive hypercapnic respiratory failure and death in patients with severe chronic obstructive pulmonary disease (COPD). A study was undertaken to determine the effects of nocturnal non-invasive bi-level pressure support ventilation (NIV) on survival, lung function and quality of life in patients with severe hypercapnic COPD.
Method: A multicentre, open-label, randomised controlled trial of NIV plus long-term oxygen therapy (LTOT) versus LTOT alone was performed in four Australian University Hospital sleep/respiratory medicine departments in patients with severe stable smoking-related COPD (forced expiratory volume in 1 s (FEV1.0) <1.5 litres or <50% predicted and ratio of FEV1.0 to forced vital capacity (FVC) <60% with awake arterial carbon dioxide tension (Paco2) >46 mm Hg and on LTOT for at least 3 months) and age <80 years. Patients with sleep apnoea (apnoea-hypopnoea index >20/h) or morbid obesity (body mass index >40) were excluded. Outcome measures were survival, spirometry, arterial blood gases, polysomnography, general and disease-specific quality of life and mood.
Results: 144 patients were randomised (72 to NIV + LTOT and 72 to LTOT alone). NIV improved sleep quality and sleep-related hypercapnia acutely, and patients complied well with therapy (mean (SD) nightly use 4.5 (3.2) h). Compared with LTOT alone, NIV (mean follow-up 2.21 years, range 0.01–5.59) showed an improvement in survival with the adjusted but not the unadjusted Cox model (adjusted hazard ratio (HR) 0.63, 95% CI 0.40 to 0.99, p = 0.045; unadjusted HR 0.82, 95% CI 0.53 to 1.25, p = NS). FEV1.0 and Paco2 measured at 6 and 12 months were not different between groups. Patients assigned to NIV + LTOT had reduced general and mental health and vigour.
Conclusions: Nocturnal NIV in stable oxygen-dependent patients with hypercapnic COPD may improve survival, but this appears to be at the cost of worsening quality of life.
Trial registration number: ACTRN12605000205639
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) remains a leading cause of death and disability worldwide.1 Long-term oxygen therapy (LTOT) was shown in the 1980s to increase survival.2 3 However, patients with severe COPD continue to suffer major disability and require frequent and costly medical intervention. Once hypercapnia develops, 2-year mortality is approximately 30–40%.4
Many patients with COPD have worsening of hypoxaemia and hypercapnia in sleep, particularly in rapid eye movement (REM) sleep, due to a fall in central respiratory drive and increased upper airways resistance.5–8 Nocturnal gas exchange disturbance in COPD may potentially predispose to cardiac arrhythmias and progressive daytime ventilatory failure. The clear benefit of non-invasive ventilation (NIV) in acute exacerbations of COPD,9 plus the overwhelming evidence that nocturnal NIV improves hypercapnic ventilatory failure, quality of life (QOL) and survival in restrictive chest wall disease and neuromuscular disease,10–12 has raised the possibility that NIV may also improve QOL and survival in patients with end stage COPD. A number of short-term studies have shown improvements in sleep quality, sleep gas exchange and awake arterial carbon dioxide tension (Paco2).13 Two recent longer-term randomised controlled trials of NIV + LTOT versus LTOT alone involving larger patient samples reported small benefits in favour of NIV.14 15 One showed a small improvement in patient dyspnoea scores,14 while the other reported slightly decreased awake Paco2 and improved dyspnoea and health-related QOL.15 The general consensus, however, is that there is insufficient evidence to recommend NIV for routine use in stable hypercapnic COPD.13 16
The present multicentre study was designed to investigate this question further. Patients with COPD with severe airflow limitation and stable hypercapnic ventilatory failure were randomised to either NIV + LTOT or LTOT alone and followed for up to 5 years. The primary outcome measure was survival. Secondary outcome measures included general and disease-specific QOL, mood and awake arterial blood gases.
METHODS
The Australian trial of non-invasive Ventilation in Chronic Airflow Limitation (AVCAL) was a randomised open-label controlled trial conducted between 1998 and 2004 in four Australian university hospitals: the Repatriation General Hospital, Adelaide, South Australia; the Royal Prince Alfred Hospital, Sydney, New South Wales; the Austin Hospital, Melbourne, Victoria; and the Charles Gairdner Hospital, Perth, Western Australia. The first patient was randomised on 30 June 1998 and the last on 28 March 2003. The trial was terminated on 15 May 2004.
Inclusion criteria were: (1) men and women aged <80 years; (2) severe COPD secondary to smoking (forced expiratory volume in 1 s (FEV1.0) <1.5 litres or <50% predicted, <20% improvement in FEV1.0 following aerosol bronchodilator, and ratio of FEV1.0 to forced vital capacity (FVC) <60%); (3) stable hypercapnic ventilatory failure (Paco2 >46 mm Hg at least twice in the previous 6 months during periods of clinical stability; (4) on LTOT17 for at least 3 months and, as required for LTOT prescription, not currently smoking. Exclusion criteria were: (1) significant co-morbidity such as malignancy, left ventricular heart failure or unstable angina likely to affect survival in the 2-year follow-up period; (2) severe psychiatric disorder likely to impair ability to comply with NIV; (3) body mass index (BMI) >40 kg/m2; (4) polysomnographic evidence of sleep apnoea (>20 apnoeas plus hypopnoeas per hour of sleep).
Randomisation and interventions
All patients underwent a full-night attended polysomnography at their prescribed LTOT flow rate that included EEG, EOG, submental EMG, airflow (oronasal thermistors), respiratory effort (chest and abdominal inductance bands), pulse oximetry and continuous transcutaneous Pco2 recording (Radiometer, TCM3, Denmark). Supine resting arterial blood gases were taken in the sleep laboratory prior to sleep and on first waking on both occasions with the patient breathing oxygen via nasal cannulae at their prescribed flow rate. Where necessary, these arterial blood gas values were used to correct for across-the-night transcutaneous carbon dioxide membrane and machine drift using a method of linear interpolation as described previously.7 Unless patients were unwilling or unable to tolerate room air breathing without their oxygen therapy, an awake morning arterial blood gas sample was also taken on room air. Sleep studies were scored by experienced sleep scorers who were blinded to treatment allocation.18 Apnoeas were defined as an absence of oronasal flow for >10 s and hypopnoeas as a >50% reduction in flow lasting more than 10 s with or without arousal or desaturation >3%. Lung function measurements including forced expiratory and static lung volumes and gas transfer were reported as absolute values and as percentage predicted using the normal values employed in the laboratories at the time. General QOL was assessed using the SF36 questionnaire and disease-specific QOL by the St Georges Respiratory Questionnaire (SGRQ).
Patients were randomly assigned to the treatment group which received NIV plus usual care including LTOT, or to the control group which received LTOT and usual care. The central study coordinator generated a random sequence of treatment assignments that were stratified by centre and distributed in blocks of 10 sealed opaque envelopes to the centres. The central coordinator verified that the patient met all eligibility criteria before the site research nurse broke the envelope seal.
The protocol for NIV initiation and aftercare was standardised between centres at an initial workshop of research nurses. Regular telephone conferences were conducted thereafter to assist with protocol queries or specific management issues and another face-to-face calibration workshop was held mid-study. Patients assigned to NIV treatment were admitted to hospital for 3–4 days for education and familiarisation with the patient triggered bi-level positive pressure device (VPAPs-mode, ResMed, Sydney, Australia). Expiratory positive airway pressure (EPAP) was set at the lowest possible level (approx 3 cm H2O) and the inspiratory positive airway pressure (IPAP) gradually increased during daytime and night time trials to the maximum tolerated with a target IPAP–EPAP difference of 10 cm H2O or greater. The choice of nasal versus full face mask and humidification was determined by the nurse to maximise patient comfort and NIV efficiency. On the third or fourth night the subject had another attended polysomnographic study during which EPAP was increased as necessary to abolish snoring and obstructive hypopnoeas/apnoeas. NIV was considered successfully established when at least 3 h of sleep were confirmed on NIV at an IPAP–EPAP difference of at least 5 cm H2O. If these criteria were not met, patients had another therapeutic sleep study. If the criteria were again not met, attempts to provide ventilatory assistance with NIV were considered to have failed and the patient was withdrawn from NIV but follow-up measurements were made and the data included in the intention-to-treat analysis. Patients telephoned the research nurse for advice if difficulties were being encountered at home with NIV, and additional visits with the nurses either in the home or hospital were arranged as required.
Outcomes and follow-up
For all patients a research nurse attempted telephone contact at 6-week intervals to first ascertain live/dead status and, if the patient had died, date of death either from the next of kin, general practitioner or state death register. For surviving patients, the hour meter values on the NIV and/or oxygen concentrator devices were read out by the patient or family member and recorded. Average daily use of NIV and LTOT was calculated as the meter reading increment divided by the total number of days since the last meter reading. The duration of all patient-reported hospital admissions was recorded. Surviving patients were asked to return at 6-monthly intervals for repeat lung function and arterial blood gas measurements and QOL assessments. At these visits, the hour meter on NIV devices was read by the research nurse.
Data analysis and statistics
The study was powered with survival as the primary outcome variable. We attempted to recruit 100 subjects in each group based on the following initial assumptions: 2-year study; underlying 2-year survival rate in the LTOT group of 60%; NIV would increase survival rate to 80%; average loss to follow-up of 15% over 2 years; 80% power using a 0.05 level two-sided log-rank test for equality of survival curves (nQuery Advisor 4.0). In practice, recruitment rates were much slower than anticipated. To adjust for this, the length of the periods for recruitment and follow-up were extended substantially.
Statistical analyses were undertaken using SPSS 16 for Windows (SPSS, Chicago, Illinois, USA) and Stata 10 (College Station, Texas, USA). All primary analyses were conducted on an intention-to-treat basis. However, since a proportion of patients assigned to NIV treatment did not use the treatment regularly or abandoned it altogether after a time, a planned per protocol subanalysis was conducted comparing outcomes of patients in the treatment arm who used NIV consistently (defined as average of >4 h per night) with patients in the control arm.

Flow of participants through the randomised controlled trial of non-invasive ventilation plus long-term oxygen therapy (NIV + LTOT) versus LTOT alone. *At various times in the study a total of eight patients either withdrew their consent to be further contacted or were found to be non-contactable. Their data were included in the survival analysis to the time of the last follow-up. †Three patients in the LTOT alone group crossed over to NIV treatment during the study and were excluded from the per protocol analysis.
A Cox survival analysis was performed. Baseline measures were first assessed for confounding by determining if the addition of the variable to the crude model changed the hazard ratio by 10% or more. Pao2, Paco2 and the SGRQ Total Score were found to be confounding variables and were therefore included in the final model. Missing values were imputed by the approach of expectation-maximisation. A global test of the proportional hazards assumption based on Schoenfeld residuals was undertaken. The crude and adjusted hazard ratios with 95% confidence intervals for NIV + LTOT treatment versus LTOT alone are reported.
Random effects modelling was undertaken on arterial blood gas and FEV1.0 and FVC data. The combined effects of a high mortality rate in the study population and an inability or reluctance on the part of patients to return to hospital for repeat testing towards the end of the follow-up period meant that there were a number of missing data for QOL and physiological measurements after 12 months of follow up. Statistical analyses of these data have therefore been confined to the first 12 months of the trial. Even so, the severity of the patients’ respiratory disease meant that there remained missing values and patients were often unwilling or unable to come off oxygen for blood gas measurements while air breathing or to perform pulmonary function tests both before and after bronchodilator treatment, and prescribed oxygen flow rate had sometimes changed between measurements. To select comparable data from the maximum possible number of patients in both treatment arms, arterial blood gas and lung function data have been matched for equivalent conditions (including oxygen flow rate for arterial blood gas tensions on oxygen) at baseline, 6 and 12 months in each patient. Partial data were included if baseline and one other visit data were available.
Owing to the highly skewed nature of most QOL and mood, ranked analysis of covariance was used to compare mean rank scores at 12 months in the two treatment groups after adjustment for ranked baseline values. Patient hospitalisation rates in the two groups were compared using the large sample Z-test.
RESULTS
One hundred and forty-four patients met the eligibility criteria and were randomised, 72 to the NIV+LTOT group and 72 to the LTOT group. Table 1 shows the baseline characteristics of the patients in the two groups. As expected, approximately two-thirds of subjects with COPD were male, with a mean age in the late 60s. Patients had severe airflow obstruction, very low carbon monoxide gas transfer consistent with severe emphysema and significant awake hypoxaemia and hypercapnia while breathing room air. The baseline SGRQ scores indicate that patients were severely disabled by their respiratory disease.
Table 2 shows the baseline sleep study findings in the two groups and the effects of positive pressure ventilation on sleep architecture and the sleep-related rise in transcutaneous Pco2. As expected, sleep efficiency was very low, there was a marked rise in transcutaneously measured Pco2 during sleep and the frequency of apnoeas and hypopnoeas was low. The sleep study following in-hospital implementation of NIV in the treatment group showed small but significant increases in REM sleep and decreases in the frequency of disordered breathing events and sleep-related rise in transcutaneous Pco2. Patients were able to tolerate moderate IPAP and EPAP levels.
Median follow-up time was 28.5 months in the NIV+LTOT group and 20.5 months in the LTOT group. Only eight patients (5.5%) were lost to follow-up, four in LTOT and four NIV + LTOT treatment arms. The mean (SEM) flow rate and adherence to oxygen therapy computed to the time of death or last follow-up did not differ between the two arms of the study (NIV + LTOT: 1.9 (0.6) l/min, 18.8 (0.6) h/day; LTOT: 1.9 (0.1) l/min, 18.8 (0.6) h/day; p = NS). Mean (SD) adherence to NIV for those assigned to this therapy was 4.5 (3.2) h/night; 41/72 patients (60%) used NIV for >4 h/night and were included in the per protocol analysis.
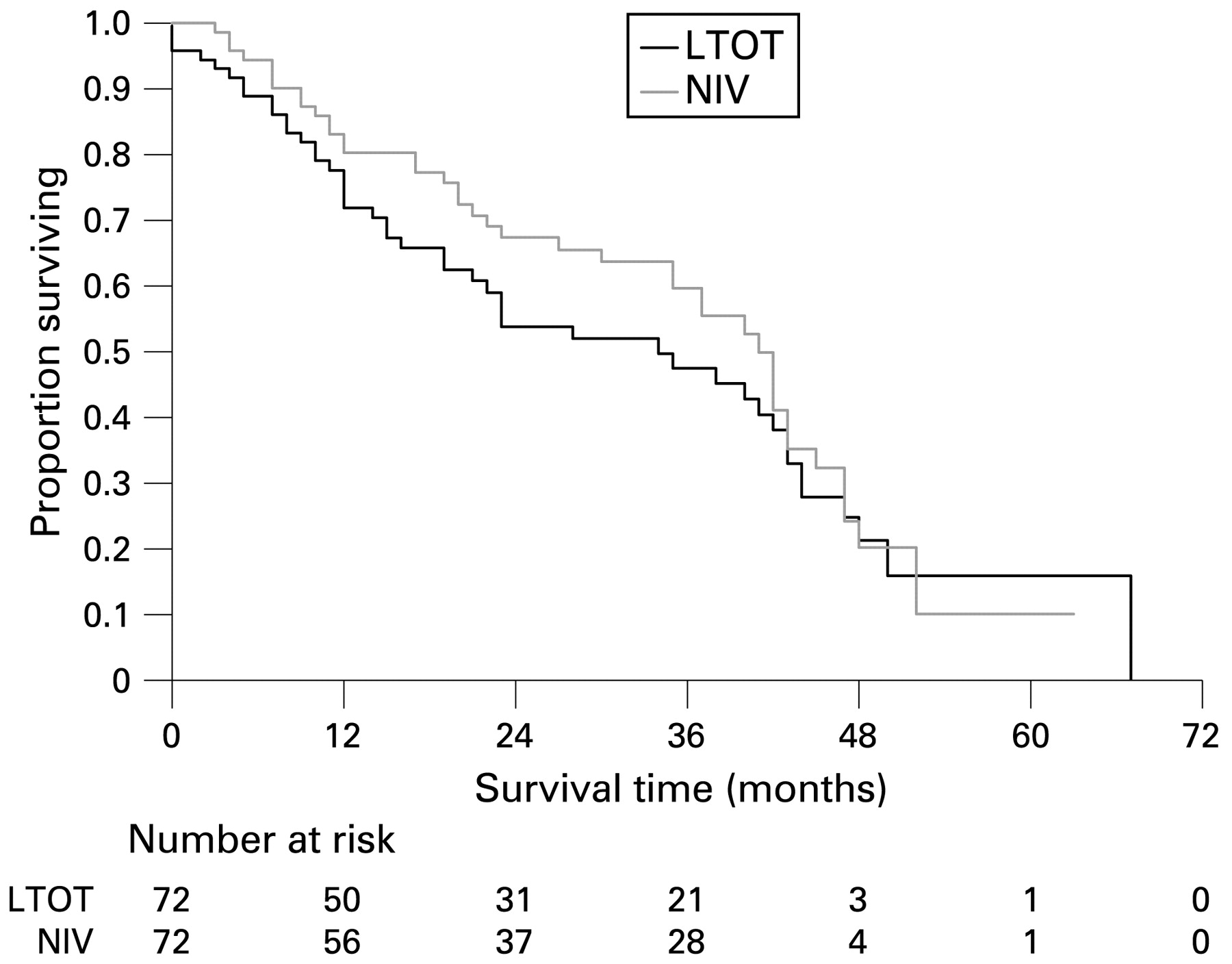
The number of deaths per treatment arm was 40 for NIV + LTOT and 46 for LTOT alone. The adjusted survival analysis showed a survival advantage in favour of the NIV + LTOT group for both intention to treat (hazard ratio (HR) 0.63 (95% CI 0.40 to 0.99); p = 0.045) and per protocol analyses (HR 0.57 (95% CI 0.33 to 0.96); p = 0.036). The unadjusted survival HR was not significantly different from 1 (HR 0.82 (95% CI 0.53 to 1.25)). The adjusted survival curves for the intention-to-treat analysis are shown in fig 2.
{kind=link}
{kind=link}
Survival curves of patients randomised to non-invasive ventilation plus long-term oxygen therapy (NIV + LTOT) and long-term oxygen therapy (LTOT) alone. Curves were constructed after adjustment for confounding by baseline differences in arterial oxygen and carbon dioxide tensions and respiratory quality of life measurements. Because of the small number of patients followed up for 3 or more years, there is considerable uncertainty about the true shape of the extreme right-hand end of the survival plots.
No differences were observed between the two groups in Pao2, Paco2 or FEV1.0 in the first 12 months of follow-up (table 3). Other parameters of lung function (gas transfer factor, static lung volumes) also showed no statistically significant differences.
Disease-specific QOL (SGRQ) at 12 months was not different between the NIV + LTOT and LTOT alone groups. However, statistically significant differences were observed in several subscales of the SF36 (table 4) and profile of mood states (POMS, table 5) questionnaires, suggesting that patients treated with NIV had poorer general and mental health and reported less vigour and more confusion and bewilderment. Hospitalisation rates were not different between the two groups (LTOT vs LTOT + NIV: days on trial 54 708 vs 62 182; days in hospital 1697 vs 2020; rate 0.031 vs 0.032; rate ratio 0.96 (95% CI 0.90 to 1.02), p = 0.161 based on large sample Z-test.
DISCUSSION
This study is the largest randomised controlled trial reported to date of non-invasive bi-level positive pressure treatment during sleep in stable end-stage hypercapnic COPD. At baseline, patients showed evidence of poor quality sleep and significant hypoventilation, and those assigned to NIV treatment demonstrated modest improvements in sleep architecture and sleep hypoventilation with the application of NIV treatment. Patients on NIV adhered well to the therapy (mean 4.5 h/night) over the period of follow-up. After adjusting for baseline differences in clinically important variables, NIV treatment was shown to produce an improvement in survival but no change in daytime arterial blood gas or lung function measurements or hospitalisation rates. Disease-specific and general QOL did not improve as a result of NIV treatment. On the contrary, it appeared that the addition of NIV to usual care in these severely disabled COPD patients resulted in deterioration in general and mental health and some aspects of mood.
This is the first randomised controlled trial to show an improvement in survival with the application of nocturnal NIV in end-stage chronic hypercapnic COPD. The survival advantage was apparent on the adjusted but not the crude survival analysis. Survival advantage was slightly greater in the per protocol analysis (ie, restricted to patients who complied >4 h/night with NIV treatment) than the intention-to-treat analysis, suggesting that the nightly duration of NIV treatment was an important determinant of outcome. That survival improved without any change in daytime arterial blood gases was surprising since clinical gains from NIV in other forms of chronic respiratory disease (eg, obesity-hypoventilation syndrome, neuromuscular weakness) are normally accompanied by improvements in daytime blood gases as well as nocturnal gas exchange. It is possible that in our study the level of ventilatory support was sufficient to be cardioprotective but not to improve awake central respiratory drive. Patients with severe COPD have a high prevalence of cardiovascular disease.19 It is conceivable that patients with severe COPD may be prone to sudden cardiac death secondary to sleep-disordered breathing. Unfortunately we did not collect data on the mode or time of death which may have shed light on this possibility.
Two previous randomised controlled trials of sleep NIV therapy in hypercapnic COPD that followed patients for 12–24 months14 15 reported an improvement in patient dyspnoea scores with NIV and one reported a small improvement in daytime Paco2 on usual oxygen therapy but not while breathing ambient air. Neither study found any survival advantage for NIV, but both studies were significantly underpowered to examine mortality.
The survival benefit observed in our study was of borderline statistical significance. Our data, however, suggest that ventilatory support at night was incomplete, which may have limited the potential treatment benefit. Average NIV compliance was 4.5 h/night and NIV failed to normalise sleep architecture and gas exchange during sleep. Others have suggested that the level of inspiratory pressure delivered by NIV may be a crucial factor in determining treatment response.16 Our average IPAP–EPAP difference was 8 cm H2O and average IPAP 13 cm H2O, which are similar14 or slightly lower15 pressures to those reported in the other two longer term randomised controlled trials. It is possible that the use of higher levels of IPAP may result in greater treatment benefits. Recently, a retrospective study reported using IPAP levels ranging from 17 to 40 cm H2O in patients with hypercapnic COPD20 with subsequent reduction in awake Paco2 and some improvement in FEV1.0 after 2 months and a 2-year survival of 86%. However, there was no control group and patients also received daytime ventilation. There are no randomised controlled trial data available to date in patients with hypercapnic COPD to assess the tolerability of NIV delivered in this fashion or its effects on survival and QOL.
As shown by the SGRQ, our patients had severe disease-specific impairment of QOL and we failed to detect any change in SGRQ in either arm of the study. Clini et al,15 in a similar long-term randomised controlled trial to ours, showed improvement in NIV-treated patients with COPD in disease-specific QOL using the the Maugeri Foundation Respiratory Failure questionnaire (MRF-28) but not the SGRQ.15 It has been suggested that the MRF-28 may be a more sensitive instrument to measure disease-specific QOL treatment effects in patients with respiratory failure.15 21 The other long-term randomised controlled trial of NIV in hypercapnic COPD14 did not report health-related QOL. Two short-term studies of 8 and 12 weeks, respectively,22 23 reported improvements in disease-specific QOL following NIV, but the relevance of these data to long-term NIV use in this patient group is uncertain.
Ours is the first long-term randomised controlled trial of NIV in hypercapnic COPD to assess health status using validated general QOL and mood questionnaires. To our surprise, we found that patients on NIV had more confusion/bewilderment and less vigour on the POMS than those receiving oxygen therapy alone. This deterioration was matched by worsening SF36 measured QOL in the NIV arm of the study with poorer scores for general and mental health. There was no improvement in the vitality subscale of the SF36, in contrast to increased vitality usually seen following NIV intervention in other forms of sleep-related respiratory failure.24 The general worsening of mood and QOL may reflect the relative additional complexity of therapy associated with NIV in the absence of perceived improvement in health status. Alternatively, a survivor effect in the NIV group could lead to an apparent worsening of mood and QOL (ie, patients living longer with end-stage COPD may report more disturbances in mood and QOL) and is hard to distinguish from a true negative effect of therapy. Nevertheless, these findings emphasise the need to closely measure QOL in future randomised controlled trials in this patient group. Small gains in survival from NIV may potentially be negated by decrements in QOL.
A limitation of the study was our difficulty in recruitment and subsequent loss of power for the primary survival analysis. Another limitation was the loss of follow-up data for the secondary outcome measures due to the combined effects of a high mortality rate and an inability or reluctance of patients to return to hospital for repeat testing. This reflects the nature and disability in patients with end-stage COPD and geographical limitations of the study centres in the Australian setting.
In summary, this study is the first to demonstrate a survival advantage for chronic NIV in hypercapnic COPD. While these results are encouraging, our enthusiasm for NIV treatment is tempered by the observation that it was accompanied by reduced self-reported QOL. Whether the latter can be improved by more effective education, ventilator settings or mask technology needs further study. For now, we recommend that NIV in hypercapnic COPD be confined to patients enrolled in new randomised controlled trials.
REFERENCES
Footnotes
See Editorial, p 553
Funding: Australian National Health and Medical Research Council, Air Liquide Healthcare, Australian Lung Foundation.
Competing interests: None.
Ethics approval: The ethics committee of each participating centre approved the protocol and patients gave written informed consent.
Complete list of AVCAL investigators. Adelaide: R D McEvoy, F J O’Donoghue, P G Catcheside, L S Rowland, R Antic, H W Greville, A M Southcott; Sydney: R R Grunstein, D J Barnes, I H Young, E E Ellis, E R Collins, A J Piper; Melbourne: R J Pierce, F J O’Donoghue, K Detering, L B Irving, C F McDonald, C J Worsnop, L M Schachter, S E Rochford; Perth: D Hillman, P Eastwood.
Linked Articles
- Editorial
- Editorial