Article Text

Abstract
Background: While clinical trials with antileukotrienes have shown overall beneficial effects in asthma, the factors that determine leukotriene dependent asthma are still unclear. A study was undertaken to determine whether or not leukotriene responsiveness in the airways correlates with endogenous leukotriene biosynthesis.
Methods: Bronchial responsiveness to leukotriene (LT) D4 was assessed as PD20FEV1 in 20 subjects with mild asthma and 10 healthy controls, and compared with bronchial responsiveness to methacholine and two global measures of leukotriene production—urinary LTE4 and ex vivo production of LTB4 in whole blood.
Results: In patients with asthma the bronchoconstrictor activity of LTD4 was about 1300 times greater than methacholine (geometric mean PD20 0.69 nmol v 887 nmol). Those who were most responsive to LTD4 were relatively less responsive to methacholine (p<0.01). There was, however, no correlation between bronchial responsiveness to LTD4 and urinary LTE4 or blood ex vivo LTB4 levels in asthmatic subjects or healthy controls. Subjects with asthma treated with inhaled corticosteroids produced higher levels of LTB4 (p<0.05).
Conclusions: General measures of leukotriene production cannot predict bronchial responsiveness to LTD4. The unique bronchoconstrictive potency of LTD4 on human airways may relate to the locally regulated expression of the cysteinyl LT1 receptor.
- CysLT, cysteinyl leukotriene
- FEV1, forced expiratory volume in 1 second
- Feno, fractional exhaled nitric oxide
- ICS, inhaled corticosteroids
- MCh, methacholine
- PD10, PD15, PD20, provocative dose causing a 10%, 15% and 20% decrease in FEV1
- asthma
- bronchial responsiveness
- leukotrienes
Statistics from Altmetric.com
- CysLT, cysteinyl leukotriene
- FEV1, forced expiratory volume in 1 second
- Feno, fractional exhaled nitric oxide
- ICS, inhaled corticosteroids
- MCh, methacholine
- PD10, PD15, PD20, provocative dose causing a 10%, 15% and 20% decrease in FEV1
The leukotrienes (LT) and, in particular, the cysteinyl leukotrienes (CysLTs; LTC4, LTD4 and LTE4) mediate central components of asthmatic airway inflammation such as bronchospasm, mucus production, eosinophil recruitment, and vascular reactions leading to tissue oedema.1 Over the past decade antileukotrienes—that is, drugs which block the formation or actions of leukotrienes—have been introduced as new treatments for asthma. Antileukotrienes therefore have a completely different mode of action from that of other asthma medications.1
The further clinical use of antileukotriene drugs is, however, hampered by a lack of understanding of which patients benefit from this treatment.1 There is a distribution of clinical responsiveness to antileukotriene drugs that suggests the presence of responders and non-responders.2–5 Attempts to correlate the treatment response with genetic polymorphism in 5-lipoxygenase (the first enzyme in the leukotriene pathway) or leukotriene C4 synthase (the enzyme initiating production of CysLTs) have produced conflicting results.6–8 So far, no major genetic determinant of leukotriene dependent asthma has been identified.
Another strategy in the quest to define responsiveness to antileukotriene drugs has been to define more precisely the phenotypic characteristics of such patients. The focus has been on the possibility that the propensity to generate leukotrienes during asthmatic inflammation is a marker of leukotriene dependent asthma. This hypothesis has received some support from the observations that subjects with aspirin intolerant asthma (AIA) respond well to antileukotriene treatment and have a high basal production of leukotrienes measured as urinary LTE4 (U-LTE4).5,9–11 It has also been claimed that the degree of ex vivo release of CysLTs from blood leucocytes is correlated directly with the clinical response to the leukotriene receptor antagonist pranlukast.12 However, in patients with AIA there was no correlation between U-LTE4 and the treatment response to the leukotriene antagonist montelukast.5
While it is uncertain whether the production of leukotrienes correlates with the beneficial effect of antileukotrienes, the responsiveness to leukotrienes in the airways has not been taken into account. It is not known if increased bronchial responsiveness to leukotrienes is an indicator of a predominant leukotriene component in asthmatic inflammation. We have therefore embarked on a series of studies of factors that determine leukotriene responsiveness in the airways. The aim of the first investigation in this project was to assess whether or not the responsiveness of an individual to inhaled LTD4 is related to the general propensity to synthesise leukotrienes. As CysLTs cause bronchoconstriction and many other biological effects by activation of the G protein coupled CysLT1 receptor, it was hypothesised that there might be a relation between the endogenous level of agonist (CysLTs) and the airway responsiveness to inhaled LTD4.13 It is common for agonist levels to influence the degree of receptor expression.14 For this study, two different global measures of leukotriene production—U-LTE4 and blood ex vivo LTB4 generation—were assessed. LTE4 is the end product of the CysLTs excreted into the urine and its level is a reflection of whole body biosynthesis of CysLTs.15 As circulating levels of leukotrienes in the blood are very low and far below the detection limit of reliable assays, standardised ex vivo stimulation of whole blood with secretagogues such as a calcium ionophore has been introduced as an indirect method of assessing the biosynthetic capacity of blood cells for leukotriene production.16 In this setting LTB4 is the main leukotriene formed, and its synthesis is thought to reflect the degree of 5-lipoxygenase activity.
This cross sectional study of 20 subjects with asthma and 10 healthy controls therefore tested whether bronchial responsiveness to LTD4, expressed as the PD20 value, was correlated with leukotriene production measured as U-LTE4 and blood ex vivo production of LTB4. Bronchial responsiveness to LTD4 was also compared with responsiveness to methacholine (MCh), selected as a general marker of airway responsiveness, and with the fraction of expired nitric oxide (Feno) as a surrogate marker of airway inflammation, both being common asthma outcome variables in treatment studies. Although descriptive data on LTD4 responsiveness are available in the literature, there is almost no mechanistic information about factors that determine leukotriene responsiveness in humans.17
METHODS
Subjects
Twenty subjects with intermittent to mild asthma according to GINA criteria18 and documented airway hyperresponsiveness to MCh and 10 healthy individuals were included in the study. Subjects with asthma were recruited from a general practitioner’s clinic and the healthy volunteers through advertisements. All subjects were never smokers or non-smokers for the last 2 years with a smoking history of less than 5 pack years who had not had a respiratory tract infection during the 4 weeks before screening. Atopic subjects were not studied during seasonal allergen exposure and subjects with allergy to animal dander were required to avoid animal contact for >2 weeks before and during the study.
The 20 subjects with asthma were in a stable condition with forced expiratory volume in 1 second (FEV1) ⩾70% of predicted. Ten of the asthmatic subjects used a stable dose of inhaled corticosteroids (ICS) and short acting β2 agonists as rescue, and 10 used short acting β2 agonists as their sole medication (table 1).
Subject characteristics
The healthy individuals were skin prick test negative to 10 common allergen extracts and did not display significant bronchoconstriction with a fall of ⩾20% in FEV1 when challenged with a cumulative dose of 45 282 nmol MCh.
The study was approved by the ethical review board at the Karolinska University Hospital (EtDnr 00-267) and the subjects gave written informed consent before taking part.
Study design
The screening visit included subject characterisation with documentation of history, a MCh challenge, and a skin prick test. Three further visits were scheduled 2 weeks apart, and the subjects always reported to the clinic at the same time in the morning. At visit 1 Feno was measured according to the ATS/ERS standard,19 dynamic spirometric tests were performed, blood samples were collected for analysis of whole blood ex vivo LTB4 production, and urinary samples were collected for analysis of baseline U-LTE4 concentrations. In the subjects with asthma, quality of life was measured using the Asthma Quality of Life Questionnaire (AQLQ) devised by Juniper et al.20 The patients were asked to indicate the extent to which their quality of life was limited on a 7-point scale where 1 indicates maximal impairment and 7 no impairment at all. At visit 2, blood and urine samples were collected and spirometric tests performed as the subjects underwent a bronchoscopic examination as part of a separate ongoing mechanistic investigation of the leukotriene pathway in the lung. At visit 3, inhalation challenge with LTD4 was performed in addition to blood and urine sampling. Short acting β2 agonists were withheld for at least 6 hours before visits except for visit 2.
Inhalation challenge
Pulmonary function was measured as FEV1 on a spirometer (Vitalograph MDI Compact; Förbandsmaterial, Stockholm, Sweden) and the baseline defined as the best of three recordings. All bronchoprovocation tests were performed using a dosimeter controlled jet nebuliser (Spira Elektro 2; Intramedic, Bålsta, Sweden). Challenges always began with inhalation of the respective diluent. Provided FEV1 did not change by more than 10%, incremental doses of the provocative agent were administered until FEV1 had fallen by at least 20% from post-diluent baseline. For LTD4 bronchoprovocation tests, approximately half-log increments in the cumulative dose (3, 10, 30 pmol) were inhaled every 10 minutes (dose range 3–335 780 pmol). This was achieved by using six solutions of good manufacturing practice (GMP) grade LTD4 (sealed colour coded vials each containing 1 ml of solution; concentrations increasing by tenfold from 4.2×10−9 M to 4.2×10−3 M; 4:1 solvent water:ethanol; Cascade Biochemicals; Reading, UK) and a varying number of breaths (2–7) from each solution.9 Spirometric tests were performed 5 and 10 minutes after each dose and the peak fall used for calculation of PD20. Airway responsiveness to MCh was assessed with a similar protocol but with dose increments every 3 minutes and single FEV1 measurements.9 Three concentrations (6.24, 50, 400 mM prepared at Norrlands University Hospital Pharmacy) were used to create increasing doses (range 89–45 282 nmol).
Collection of urine samples and analysis of urinary LTE4
Urine was collected on arrival on each of the three study days, two samples at visit 1 with 1 hour in between and one sample at visits 2 and 3. The total volumes of the urine samples were measured, aliquoted, immediately frozen without preservatives, and stored at −20°C until analysis. The concentration of LTE4 was determined using a previously validated enzyme immunoassay method with data expressed in relation to creatinine excretion determined colorometrically.21 The rabbit polyclonal CysLT antiserum used in the present study cross reacted with LTE4 (67%), LTC4 (100%), and LTD4 (100%). Acetylcholine esterase linked LTE4 was used as tracer and unlabelled LTE4 as standard. Baseline U-LTE4 refers to the mean value of the four baseline samples.
Ex vivo ionophore induced formation of LTB4 in whole blood
Blood samples were obtained by venepuncture into heparinised vaccutainer tubes upon arrival at visits 1, 2 and 3. Ex vivo stimulation of freshly drawn peripheral whole blood was performed with a modified version of previously described protocols.16,22 The blood was kept at room temperature for 1 hour before incubation to minimise fluctuations in values due to decreased capacity for leukotriene formation within the first hour of blood collection.16 The calcium ionophore ionomycin was dissolved in 95% ethanol to a stock concentration of 10 mM. The stock solution and vehicle (95% ethanol) were diluted 10 times with autologous plasma. Aliquots of blood (1 ml) were preincubated at 37°C for 2 minutes, followed by addition of vehicle or ionomycin in 50 µl autologous plasma. The final concentration of ionomycin was 50 µM. Incubations were continued for 15 minutes at 37°C and interrupted on ice. Plasma was obtained by centrifugation at 714g for 5 minutes at 4°C and stored at −70°C until assayed for LTB4 by enzyme immunoassay (Cayman Chemical, Ann Arbor, MI, USA). Data were expressed in relation to the white blood cell (WBC) count on each blood collection day. The mean values of the three visit days were used for comparisons between groups, whereas correlation with PD20LTD4 was tested for values obtained on the day of the bronchoprovocation (visit 3).
Statistical analysis
The provocative doses causing falls of 10%, 15% and 20% in FEV1 (PD10, PD15, PD20) were derived by linear interpolation from the respective log cumulated dose-response curves. Calculations of geometric mean values were performed on log transformed raw data. Urinary LTE4 and ex vivo LTB4 concentrations are expressed as median values with ranges. Correlations between bronchial challenges were performed with Pearson product moment correlation and all others with Spearman rank order correlation. The Mann-Whitney rank sum test was used for comparison between groups and Kruskal-Wallis one way analysis of variance on ranks was used to assess variability in values of ex vivo LTB4 and U-LTE4 at baseline. Differences were considered significant if p<0.05.
RESULTS
Bronchial responsiveness to LTD4 and MCh
The dose-response relations for inhaled LTD4 and MCh in all individuals are shown in fig 1A–C, and group mean data for different measures of responsiveness are given in table 2.
Geometric mean (range) bronchial responsiveness data
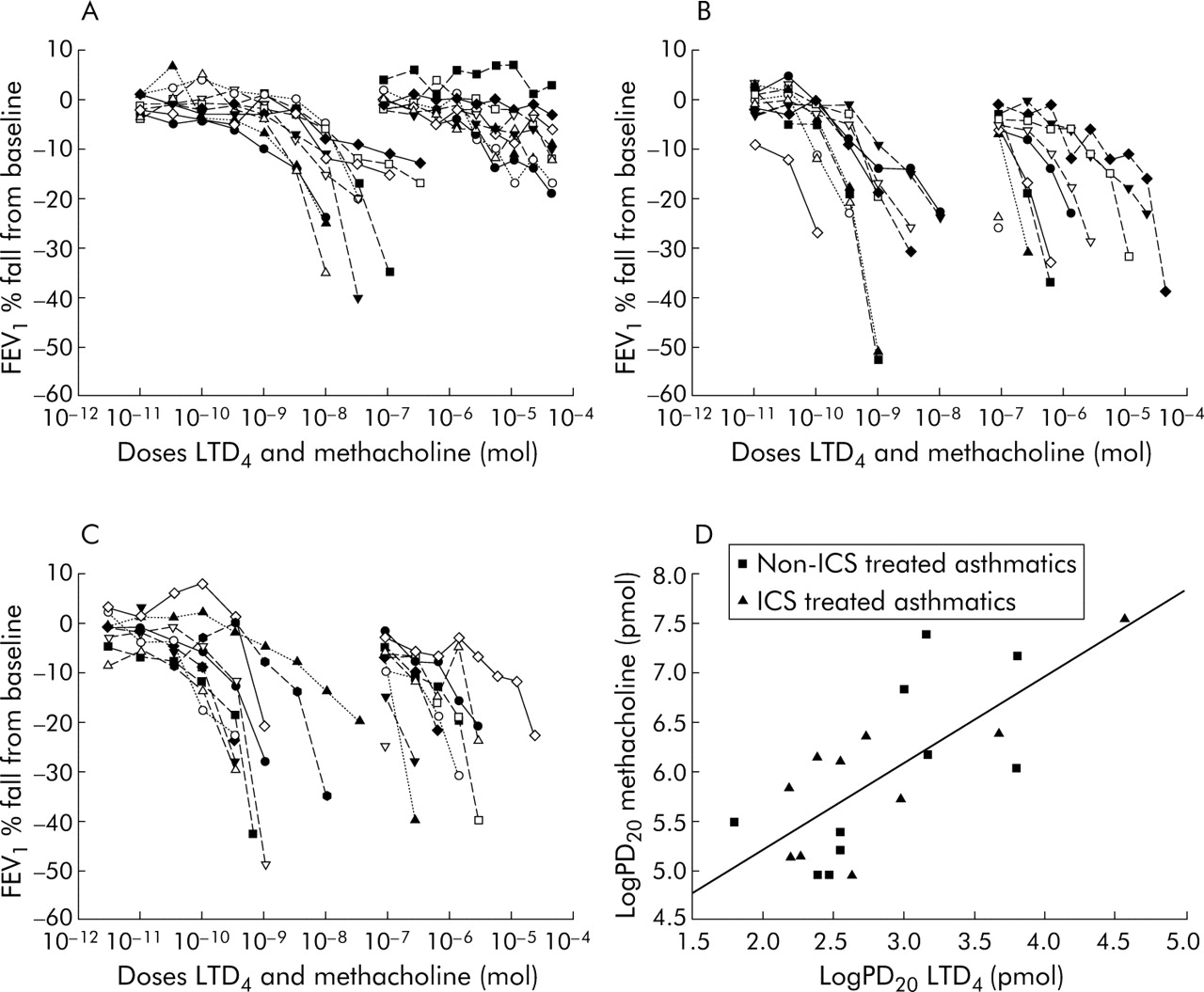
Individual dose-response curves for LTD4 (left) and methacholine (right) in (A) healthy subjects, (B) non-ICS treated asthmatics, and (C) ICS treated asthmatic subjects. (D) Comparison of airway responsiveness to inhaled LTD4 and methacholine indicated by the respective log PD20 values in the asthmatic subjects (r = 0.73, p<0.001, Pearson product moment correlation). ICS, inhaled corticosteroids.
All subjects with asthma produced PD20 values for LTD4 and MCh with no significant difference in responsiveness between the group taking ICS and the group that did not (table 2). The geometric mean (range) PD20LTD4 and PD20MCh for all subjects with asthma (n = 20) was 0.69 (0.062–37.05) nmol and 887 (89–37 188) nmol, respectively. Thus, on a molar basis, LTD4 was over a 1000 times more potent than MCh (PD20 ratio 877/0.69 = 1285; fig 1B and C). Very similar dose ratios between LTD4 and MCh were also obtained if PD15 or PD10 values were compared in the subjects with asthma (table 2).
Airway responsiveness to LTD4 was significantly correlated with responsiveness to MCh in the asthmatic subjects (r = 0.73, p<0.001; fig 1D). However, across the range of airway hyperresponsiveness to MCh, LTD4 was a relatively less potent bronchoconstrictor in the subjects with asthma most responsive to inhaled MCh and a more potent bronchoconstrictor in the subjects least responsive to inhaled MCh. There was a linear relation between airway responsiveness to MCh and the dose ratio of MCh to LTD4 (r = 0.6, p<0.01; fig 2).
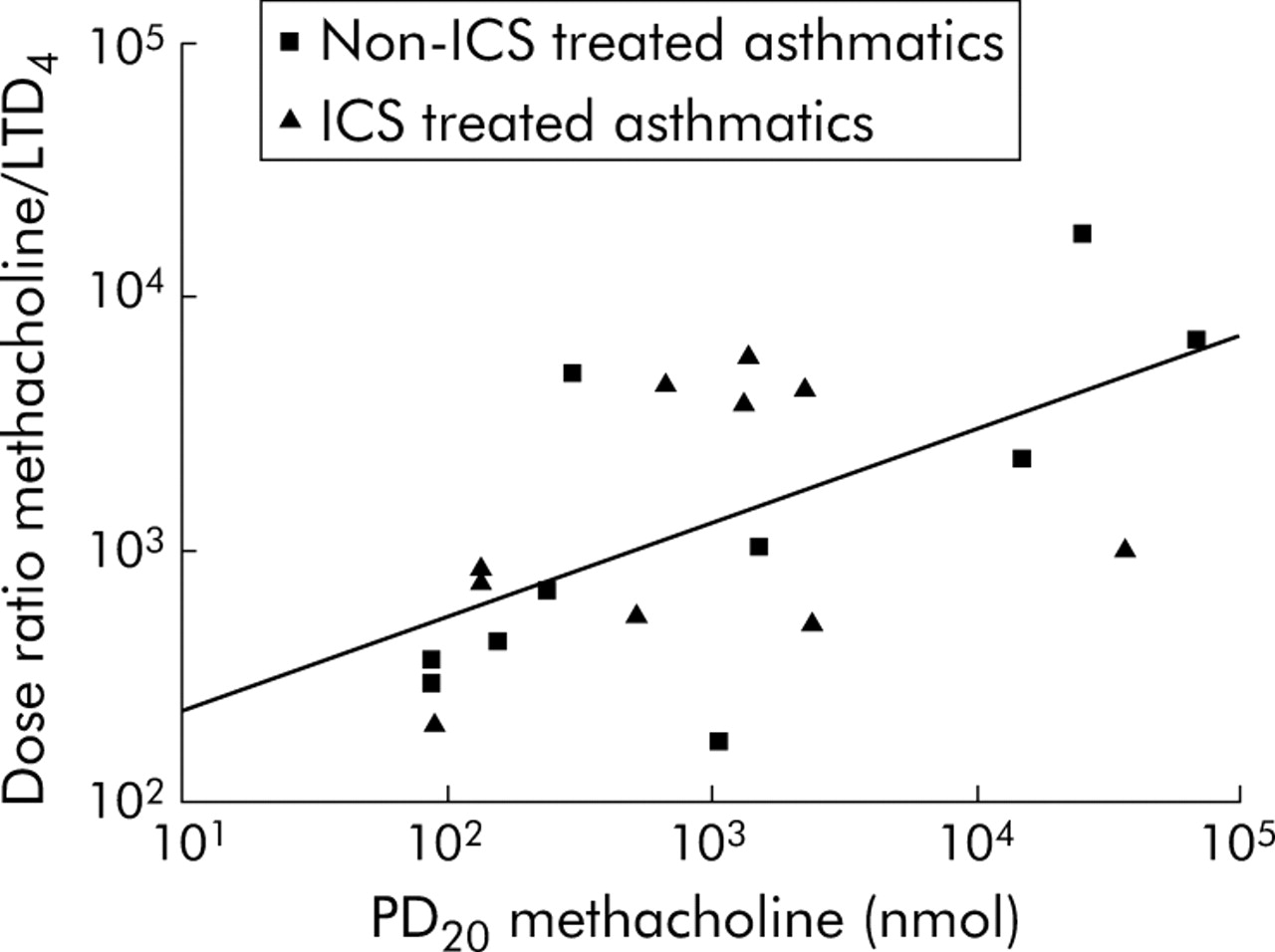
Relation between airway responsiveness to methacholine (PD20) and the relative potency of LTD4 compared with methacholine (dose ratio of MChPD20 to LTD4PD20). The linear relation between the two variables (r = 0.6, p<0.01, Pearson product moment correlation) indicates that the asthmatic subjects who were the most responsive to methacholine had the least relative airway responsiveness to LTD4.
In the healthy subjects the fall in FEV1 in response to the highest cumulative dose of MCh (45 282 nmol) was less than 15% for eight of the 10 subjects (fig 1A). In contrast, LTD4 produced a PD20 in seven of the healthy subjects and PD15 could be determined for nine (fig 1A and table 2). Compared with the asthmatic subjects, the healthy subjects were about 40 times less sensitive to either LTD4 or MCh when PD15 values for LTD4 or PD10 values for both compounds were compared (table 2). As in the asthmatic subjects, LTD4 was more than 1000 times more potent than MCh when PD10 values for LTD4 and MCh were compared in the seven healthy individuals who responded to MCh (fig 1A and table 2).
There was no correlation between the responsiveness to inhaled LTD4 and Feno in subjects with asthma or in healthy individuals at the PD15 level (data not shown).
Blood ex vivo LTB4 production and urinary excretion of LTE4
Urinary LTE4 excretion and ex vivo LTB4 production were consistent within each study group with no significant differences between the three visit days (table 3), nor were there differences in baseline U-LTE4 excretion between the three study groups (p>0.05, table 3). However, asthmatic subjects taking ICS had higher ex vivo LTB4 production than those with asthma not taking ICS (median (range) 10.7 (4.3–21.5) v 7.0 (2.5–18.1) ng/106 WBC, p<0.05). There was no correlation between ex vivo LTB4 production and U-LTE4 in either the asthmatic subjects (p>0.05) or in the healthy individuals (p>0.05, data not shown).
Median (range) leukotriene levels on the three visit days
Furthermore, there was no correlation between airway responsiveness to LTD4 and ex vivo LTB4 generation on the day of provocation in subjects with asthma (n = 20, r = 0.36, p = 0.12) or in the healthy individuals (n = 7, r = −0.12, p = 0.80; fig 3A). Likewise, there was no correlation between responsiveness to inhaled LTD4 and baseline U-LTE4 concentrations in subjects with asthma (n = 20, r = −0.22, p = 0.36) or in healthy individuals (n = 7, r = −0.17, p = 0.71; fig 3B).

{kind=link}
{kind=link}
{kind=link}
No relation was seen between airway responsiveness to inhaled LTD4 and two general markers of leukotriene production in subjects with asthma or in healthy individuals (Spearman rank order correlation): (A) blood ex vivo LTB4 production; (B) baseline U-LTE4 concentration.
DISCUSSION
No relationship was found between two global measures of leukotriene biosynthesis and bronchial responsiveness to inhaled LTD4. Although baseline data (including asthma specific quality of life) indicated that the subjects with asthma had relatively similar disease severity, their responsiveness to LTD4 varied by almost 1000 times (PD20 from 60 pmol to 40 nmol (30 ng to 20 μg). There was also no relation between LTD4PD20 and exhaled NO, although the latter displayed the expected difference between healthy subjects and asthmatics (table 1).
In the search for factors that determine leukotriene responsiveness in the airways, the effects of inhaled LTD4 were examined in one of the largest bronchoprovocation studies (n = 30) completed with this agent. Subjects with mild asthma, half of whom were receiving treatment with ICS, were chosen because they represent the vast majority (approximately 70%) of all asthma patients. Thus, in subjects with asthma, LTD4 was (on a molar basis) more than 1000 times (1285) more potent than MCh (geometric mean PD20 values obtained after inhalation: 650 pmol LTD4 (325 ng) v >900 nmol MCh (270 μg)). This potency ratio compares well with other bronchoprovocation studies and with investigations in isolated human airways.17,23 In the asthmatic subjects there was, however, no difference in absolute or relative responsiveness to LTD4 or MCh between subjects on ICS and those not on ICS.
On the other hand, the asthmatic subjects who were the most responsive to MCh had the lowest relative airway responsiveness to LTD4 compared with MCh. The relation between responsiveness to LTD4 and standard direct bronchoconstrictors has been debated.24–26 The relationship we found between responsiveness to MCh and LTD4 supports previous findings.27,28 Ädelroth et al hypothesised that asthmatic subjects with more severe airway inflammation and greater MCh responsiveness somehow had developed a specific tachyphylaxis to inhaled CysLTs, possibly as a result of increased local biosynthesis of CysLTs. Interestingly, Ketchell et al found that bronchial responsiveness to MCh but not to LTD4 was increased after allergen challenge, findings that indirectly are in line with Ädelroth’s hypothesis and our findings.29 Thus, although MCh and LTD4 are both direct bronchoconstrictors, the difference in relative potency for the two classes of bronchoconstrictors in asthmatics with varying degree of hyperresponsiveness indicates that each bronchoconstrictor has unique effects on the airways in asthma. Our findings support the hypothesis27 that subjects with asthma and a high degree of airway reactivity have developed tachyphylaxis to LTD4, presumably because of high exposure to endogenous LTD4 in their inflamed airways. Another explanation for the findings in fig 2 might be that LTD4 in subjects with more inflamed airways stimulates the release of bronchoprotective factors such as nitric oxide or prostaglandin E2. The conclusion that LTD4 has a very specific mode of action on the airways is also supported by the current observation that there was no relation between LTD4PD20 and exhaled NO, whereas MCh responsiveness has been reported to be correlated with exhaled NO levels.30
It was confirmed that LTD4 is also a potent bronchoconstrictor in subjects without asthma.24–26 Interestingly, a PD20 value for LTD4 could be obtained in seven out of 10 healthy individuals whereas only two subjects had a fall in FEV1 of more than 12% after inhalation of the highest dose of MCh used in this protocol. The latter observation is in line with the established plateau to MCh in healthy subjects.31 The less apparent plateau to LTD4 might relate to its longer duration of action in airway smooth muscle compared with agonists such as histamine or MCh.23 Bel et al found that the maximal airway narrowing to LTD4 was much greater than that produced by MCh.32 In agreement with these fundamental differences in action on the airways, the potency ratio between LTD4 and MCh (1827) could only be determined on a PD10 level in the healthy controls. However, when LTD4 responsiveness was compared for the groups, the healthy controls were about 40 times less responsive than the subjects with asthma.
Baseline urinary excretion of LTE4 was the same in all three groups studied, and there was no relation between baseline U-LTE4 and PD20 for inhaled LTD4 in subjects with asthma and healthy controls. Measurements of ex vivo LTB4 formation in whole blood also failed to establish a relation between this measure and airway responsiveness to LTD4 for asthmatics or healthy controls. Taken together, the study therefore refuted the hypothesis that there is a relation between airway responsiveness to LTD4 and the global propensity of individuals to generate leukotrienes measured either as U-LTE4 or blood ex vivo LTB4 production. It is likely that the expression of CysLT1 receptors in the airways is the primary determinant of responsiveness to inhaled LTD4. CysLT1 receptor expression and hence airway responsiveness to the inhaled agonist may, however, still be regulated by the local biosynthesis of leukotrienes in the airways measured, for example, in sputum, bronchoalveolar lavage (BAL) fluid or cells recovered from BAL fluid. Mechanistic studies to address these possibilities are ongoing.
Interestingly, we found that asthmatic patients who were receiving ICS produced somewhat higher levels of LTB4, whereas their urinary excretion of LTE4 was the same as in asthmatic patients not treated with ICS. The finding with LTB4 is new and, together with the confirmatory data on urinary LTE4, adds to the knowledge that ICS have complex effects on the leukotriene pathway with no or minimal effects on leukotriene biosynthesis generally observed in vivo.33–35 The increased levels of steroid treatment might relate to the previous finding that 5-lipoxygenase and FLAP expression in cells may be upregulated by ICS.36 As there was no correlation between ex vivo generation of LTB4 and U-LTE4 for the individual subjects, the study also confirms the hypothesis that these two measures represent two different ways to assess the leukotriene pathway.
In conclusion, the lack of relationship between global markers of biosynthesis of leukotrienes and responsiveness to LTD4 is noteworthy in view of the limited usefulness of these markers to predict the response to antileukotriene drugs. Since subjects with asthma in the current study displayed a wide three log order of magnitude variability in responsiveness to inhaled LTD4, variability in the sensitivity of the target tissue to the effects of CysLTs may perhaps be a more decisive determinant of the treatment response to antileukotriene drugs. We therefore propose that future trials aimed at the establishment of responders to antileukotriene treatment should include PD20FEV1 for LTD4. We hypothesise that such a direct measure of airway responsiveness may be more predictive than the markers of biosynthesis currently investigated. Alternatively, a composite measurement integrating both airway responsiveness and an appropriate end point for leukotriene biosynthesis may be required to define leukotriene dependent asthma.
Acknowledgments
The authors acknowledge the assistance from Ingrid Delin, Margaretha Andersson, Margitha Dahl, Gunnel de Forest, Heléne Blomqvist, and Elisabeth Henriksson.
REFERENCES
Footnotes
-
Supported by Karolinska Institutet, Centre for Allergy Research and the Stockholm County Council (ALF), and the following Swedish foundations: Heart Lung Foundation, Association Against Asthma and Allergy, Consul Bergh’s Foundation, Medical Research Council (projects 14X-9071 and 74X-15067), and the Foundation for Health Care Sciences and Allergy Research (Vårdal). This study received no support from the pharmaceutical industry.
-
Competing interests: none declared
-
Published Online First 29 July 2005