Article Text

Abstract
Background Evidence suggests that patients with COPD struggle to maintain improved physical activity (PA) after completing pulmonary rehabilitation (PR). Smartphone applications (apps) providing a comprehensive training programme have conferred healthy benefits. This study was conducted to determine whether regular usage of an app maintains PA following PR.
Methods Patients with stage II–IV COPD were enrolled in a 6-month trial following PR. After the screening period, participants were randomised into the Kaia COPD app group (intervention group (IG)) or the control group (CG). The primary outcome was PA (daily steps), measured using an activity tracker. Secondary outcomes included the COPD Assessment Test (CAT), the Chronic Respiratory Disease Questionnaire (CRQ) and the 1 min Sit-to-Stand Test (STST).
Results Sixty participants completed the study. The median steps from baseline to 6 months were significantly different between the groups, in favour of the IG (−105.3, IQR −1970.1 to 2105.8, vs CG −1173.0, IQR −3813.1 to –93.8; p=0.007). CAT was significantly decreased in the IG (15.1±8.6 vs 19.7±6.4, p=0.02), whereas the CRQ subdomains for dyspnoea (4.5±1.7 vs 3.7±1.3, p=0.033) and fatigue (4.5±1.4 vs 3.5±1.3, p=0.028) improved significantly in the IG. The STST at 6 months was not significant. Sleep duration and sleep efficiency showed no significant differences between the two groups at any time.
Conclusions A comprehensive program by using the Kaia app following PR maintained PA and improved symptoms in patients with COPD at 6 months. The app might be an important accessory tool for enhanced COPD care.
Trial registration number DRKS00017275.
- Pulmonary Rehabilitation
- Exercise
- COPD Pathology
Data availability statement
Deidentified and aggregated participant data are available from the corresponding author on reasonable request, subject to approval by an independent ethics committee.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
To date, no study has been able to demonstrate the benefits of eHealth in the postrehabilitation phase, especially in terms of maintaining physical activity (PA) in patients with COPD.
What this study adds
Regular use of the contents of the smartphone application (app) Kaia COPD app not only maintained PA in patients with COPD after rehabilitation but also improved symptoms.
How this study might affect research, practice or policy
Widespread use of eHealth has the potential to close the long-known gap in postrehabilitation.
Introduction
Pulmonary rehabilitation (PR) is defined as a multidisciplinary and comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies that include, but are not limited to, exercise training, education and behavioural changes designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote long-term adherence to health-enhancing behaviours.1 PR is considered an important modality for non-pharmacological management of COPD. Numerous trials have shown that participation in a PR programme improves health-related quality of life (HRQoL) and exercise capacity in patients with COPD.2 However, it is often challenging for patients with COPD who have completed a PR programme to maintain physical activity (PA) and to integrate regular exercise training into their daily lives. Consequently, many patients with COPD fail to adhere to exercise training after completing PR and receive insufficient instructions to continue their exercise training at home.3
A systematic review and meta-analysis of single-group and randomised trials evaluating the effect of exercise training (not necessarily PR) on PA concluded that this intervention conferred a small but significant increase in this outcome.4 Studies have highlighted the crucial importance of maintaining PA in COPD showing significantly higher survival rates correlated with increased PA.5 6 Several studies confirmed that a sustainable increase in PA following PR in patients with COPD with declining levels of PA is inconsistent following structured PR programmes.7 8
Digital therapeutics to promote behavioural change in chronic conditions have recently emerged with a growing body of evidence supporting their use across many indications.9 Of note, digital rehabilitation tools have been suggested as a means of increasing access to rehabilitation and structured exercise in different indications.10 11 Recent studies have investigated the effect of short-course digital interventions for PR in COPD, comparing them against face-to-face outpatient PR, which demonstrated comparable results in terms of HRQoL and exercise capacity as measured by the 6 min walk test.12 Further pilot studies have suggested the potential of digital applications (app) to also improve HRQoL and to reduce hospital readmissions in patients with severe symptoms when compared with standard care.13 Another pilot study suggested a moderate improvement in HRQoL in newly diagnosed COPD, regardless of disease severity.14 The effect of mobile health (mHealth) app use on PA was also investigated in an early feasibility mixed-methods study, but the effect of app usage on PA was not detected.15
The Kaia COPD app is available as a digital solution for PR and consists of an exercise training programme, breathing exercises and an educational programme.16 To the best of the authors’ knowledge, no current evidence supports the use of digital health interventions following structured PR programme PA. We hypothesised that the use of this smartphone app would maintain PA in patients with COPD following PR.
Methods
Participants and study centres
This trial was conducted as an international, bicentre, parallel-group randomised controlled trial (RCT). Study participants were in COPD Global Initiative for Obstructive Lung Disease (GOLD) stages II–IV who were randomised in a 1:1 ratio in parallel assignment to either the intervention group (IG), which was provided with the Kaia COPD app, or the control group (CG), which received standard care (accomplished by using a software randomiser, https://www.randomizer.org). Two centres specialised in inpatient PR for COPD (Schoen Klinik Berchtesgadener Land, Germany, and Zurich RehaCenter Clinic Wald, Switzerland) recruited participants. The trial was reported in line with the Consolidated Standards of Reporting Trials recommendations for the reporting of RCTs.17
The study was registered with the German Clinical Trials Register. A summary of the study protocol has been published.18
Objectives and outcomes
The primary objective was to assess the effectiveness of the newly developed COPD app as a maintenance programme after PR. The primary outcome was defined as a change in PA, measured in steps per day after 6 months. A commonly used activity tracker (POLAR A370 watch; Polar Electro Europe AG, Steinhausen, Switzerland) was used to measure the results of the primary endpoint. In a previous study, this activity tracker was also shown to be valid for daily life assessment of PA in patients with COPD.19
The secondary objectives were to evaluate the effects of the COPD app programme on functional exercise capacity (1 min Sit-to-Stand Test (STST)20), HRQoL and patient-reported health status (Chronic Respiratory Disease Questionnaire (CRQ)21 and COPD Assessment Test (CAT)22), number of exacerbations (defined as an increase in symptoms and an increase in dosage of or a new prescription of systemic corticosteroids and/or antibiotics), and depression and anxiety symptoms (Hospital Anxiety and Depression Scale23). Furthermore, we aimed to investigate patients’ compliance, adherence and safety; to identify factors that facilitate the implementation of the programme in the patient’s home setting; and to evaluate factors of the programme that are especially supportive of patient care. For additional information regarding materials and methods, see online supplemental material.
Supplemental material
Intervention
The study intervention consisted of physical exercise training sessions conducted daily by the patient via the Kaia COPD app. The app is available as a digital solution for PR in German-speaking countries. This COPD app consisted of an exercise training programme, breathing exercises and an educational programme, and was developed by healthcare professionals and PR experts. In a feasibility study for the Kaia app, promising results were obtained from a 20-day intervention on the CAT and HRQoL in patients with severely symptomatic COPD.16
Regular contacts via telephone calls were made by a trained healthcare professional to assess and discuss compliance with the study intervention. Additionally, patients were contacted by phone if they did not meet the predefined minimal adherence criteria (exercising with the app at least 4 out of 7 days a week).
Individualised strength training programme
The exercise training programme provided by the COPD app consisted of various daily whole-body exercises of 15–20 min. Most exercises included compound movements to train large muscle groups and improve upper and lower body strength and mobility. Each exercise day began with a whole-body warm-up and finished with two to three stretching exercises. During the programme, the intensity of the exercises was progressively increased dynamically based on patient feedback recorded through the application at the end of each exercise session. All exercises were explained in exercise videos, which included detailed instructions to ensure proper performance, training amount and intensity. Completed training sessions were recorded by the application, and aggregated data about training intensity and frequency were provided to the site staff to assess compliance with the study intervention. Within the exercise training programme, frequency of workouts, as well as exercise duration and intensity, were initially determined using a self-test assessing baseline exercise capacity. All exercises were performed without the need for specialised exercise equipment. Furthermore, the app promoted overall PA (eg, walking). The number of steps per day was collected by the activity tracker and reported to the app, and goals for activity were set weekly, depending on the updated individual fitness level. Users were reminded of their activity goals via push notifications provided by the app. The CG also wore the activity tracker every day and used a smartphone for the assessments but had no access to the COPD app. The IG and CG received a leaflet to encourage an active lifestyle (German version of ‘living well with COPD’) as well as individual exercise recommendations, as part of their discharge instructions to reflect the established standard of care. At the 6-month assessment, participants who were allocated to the CG were offered to use the Kaia COPD app free of charge.
Sample size calculation and statistics
Sample size calculation was based on expected changes in the primary endpoint and the average step difference between the groups from week 1 to the 6-month follow-up. The minimal clinically important difference in steps per day after PR is estimated between 350 and 1100 steps as measured with an activity tracker during an intervention.24 Assuming an SD of the outcome variable of 2500 steps/day, an expected effect size of 2000 steps/day could be assumed for programmes combining PA counselling with PR to increase activity. According to a current meta-analysis,25 to achieve 80% power and a significance level of 5% (one-sided), a sample size of 52 participants (26 participants in each group) was required. Assuming a drop-out rate of 50%, enrolment of up to 104 participants was expected. From our study group, two RCTs on outpatient training interventions were published in advance, each demonstrating high drop-out rates of 45% and 57%.26 27 The sample calculation and the primary outcome analysis were based on a two-tailed unpaired t-test comparing changes from baseline between the two groups at the final visit at the end of the follow-up period.
Discrete variables are presented as absolute and relative numbers. For continuous variables, the Shapiro-Wilk test was performed to determine the normality of distribution. Depending on the results of the Shapiro-Wilk test, mean and SD or median with IQR were reported. For discrete variables, group comparisons were performed using χ2 tests. Continuous variables were compared with either t-tests or Mann-Whitney U tests, according to the normal distribution assumption. Data are presented as boxplots or mean plots with error bars. A p value of 5% was determined as significant for all analyses. For the main analyses, we compared the CG with the IG using an intention-to-treat approach. The effect size for the Mann-Whitney U tests was calculated using rank–biserial correlation; for t-tests, Cohen’s d was calculated. This study was designed as a superiority study, and analyses were performed using the R V.4.1.1.
Results
Recruitment and baseline characteristics
Overall, 421 subjects were screened for eligibility. The trial was conducted from July 2019 to June 2021. Enrolment was terminated after the planned number of participants completed the study (n=52). Figure 1 shows the protocol for screening, randomisation and follow-up. Table 1 shows the baseline demographics of the 67 randomised patients. The 67 participants with COPD had a mean age of 64±8 years and, according to the pulmonary function testing, severe airflow obstruction with a mean FEV1% predicted of 44%±16%. Comorbidities are illustrated in table 2, showing no group differences according to distribution.
Demographic characteristics of the study population
Comorbidities of the study population

Consolidated Standards of Reporting Trials diagram. ITT, intention to treat.
Primary outcome
The main analysis showed a significant difference in the change in median steps from baseline to 6 months between the groups (IG −105.9, IQR −1970.1 to 2105.8, vs CG −1173.0, IQR −3813.1 to –93.8 steps per day; p=0.007) (figure 2). The effect size was 0.402 (IQR 0.131–0.617).

Changes in steps per day from baseline to 6 months. P value was obtained from the Mann-Whitney U test. CG, control group; IG, intervention group. **P<0.01.
The median number of daily steps at 6 months measured as an average value over 7 days was significantly higher in the IG (median steps and IQRs in the IG 5016.3 (2920.3–10 206.5) vs 3105.1 (606.4–4372.0), p=0.014) than in the CG (figure 3). The effect size was 0.370 (IQR 0.095–0.593).

Steps per day at baseline and 3 and 6 months for the IG and the CG. P value obtained from the Mann-Whitney U test. CG, control group; IG, intervention group. *P<0.05.
At baseline and 3 months, the differences were not significant between the groups (baseline, IG 6361.4 (IQR 3401.2–8304.3) vs CG 5052.21 (IQR 3531.9–8999.1) steps per day, p=0.760; effect size, 0.024 (IQR −0.264 to 0.309); 3 months, IG 4661.1 (IQR 2538.4–7829.0) vs CG 3728.0 (IQR 1889.3–5773.4) steps per day, p=0.199; effect size, 0.168 (IQR −0.125 to 0.433) (figure 3).
Secondary outcomes
COPD Assessment Test
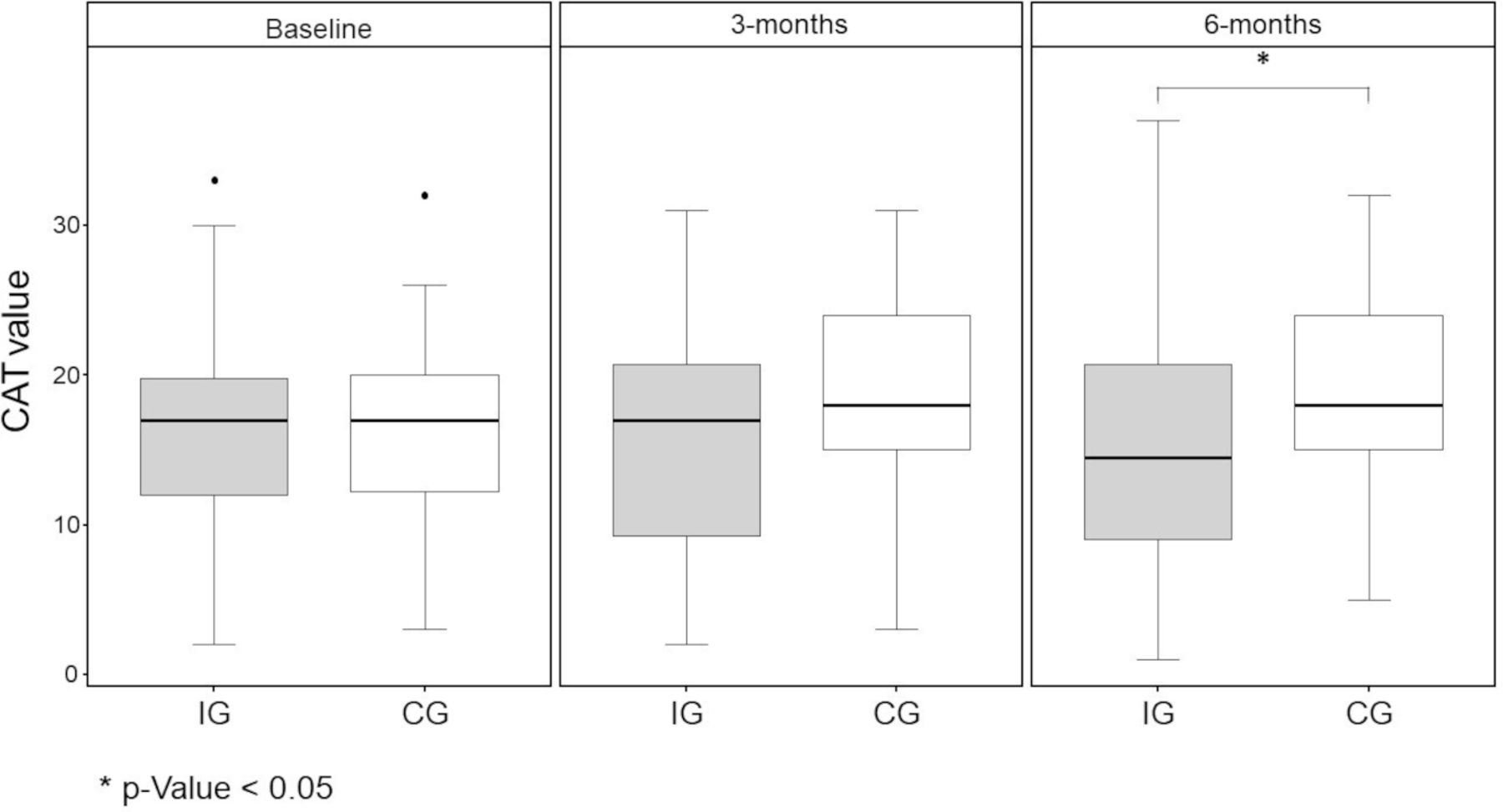
CAT scores decreased from baseline to 6 months in the IG (−1.4 point mean difference) but increased in the CG by 3.7 points (p=0.02) (figure 4 and table 3).
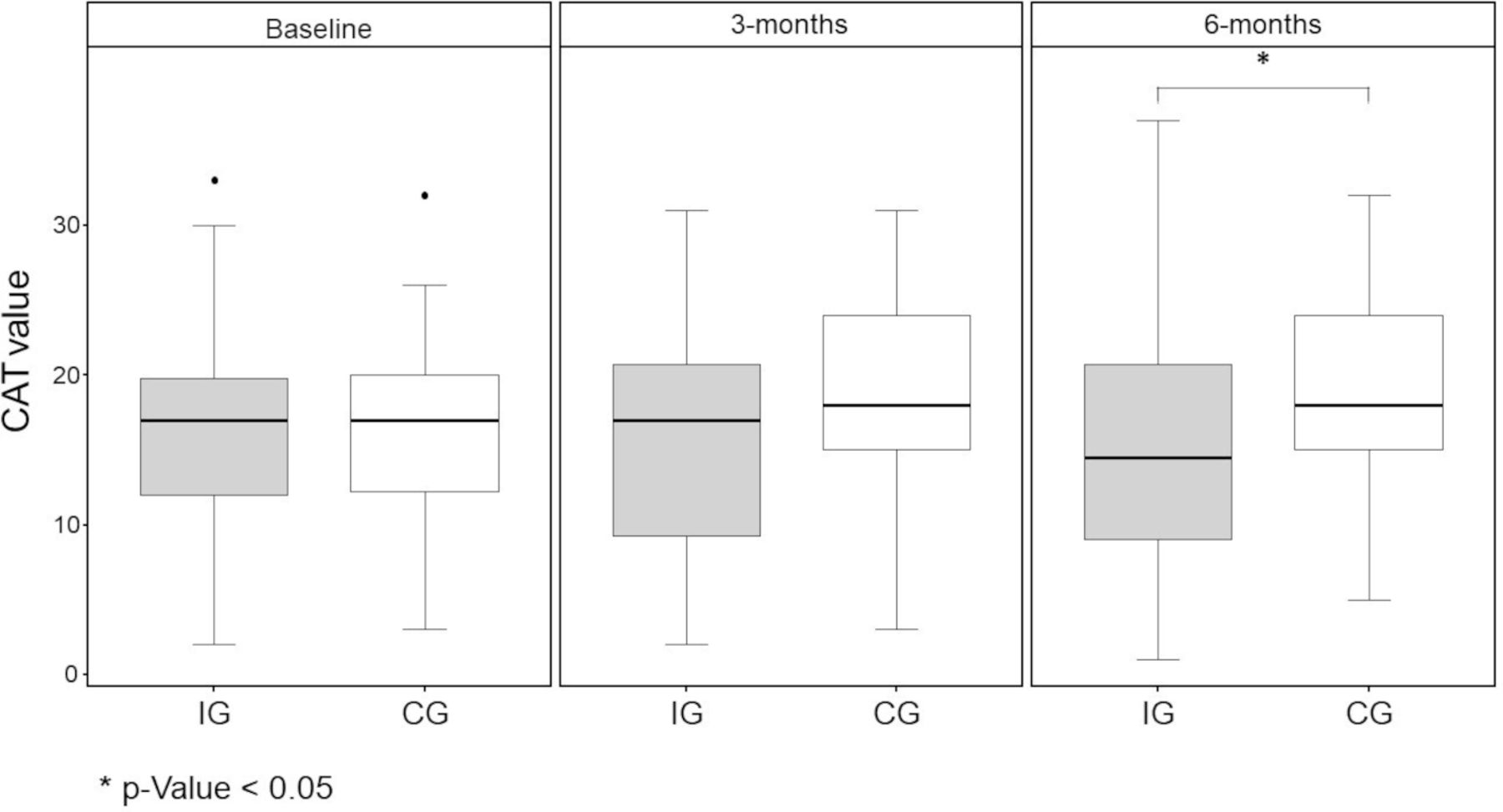
Results of the CAT for the IG and the CG. P value was obtained from the t-test. CAT, COPD Assessment Test; CG, control group; IG, intervention group. *P<0.05.
Results of secondary endpoints for the IG and CG
Chronic Respiratory Disease Questionnaire
Significant differences were found between the IG and CG for the CRQ domains of dyspnoea and fatigue. The domains of emotional function and mastery, as well as the CRQ total score, did not show significant differences between groups (table 3).
Hospital Anxiety and Depression Scale
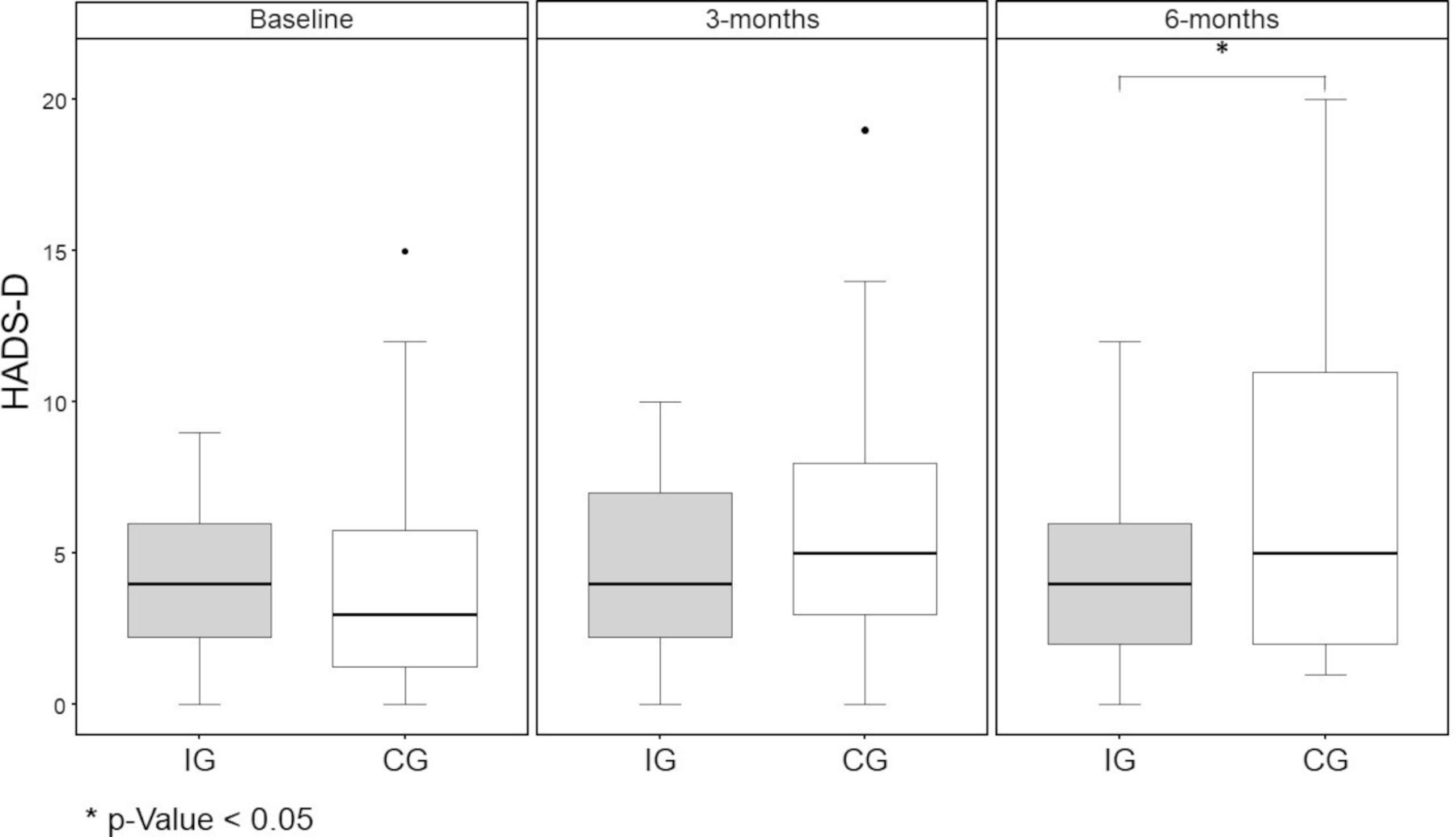
While Hospital Anxiety and Depression Scale–Depression Subscale (HADS-D) did not change significantly over the study period for the IG, the scores significantly increased for the CG (IG 4.20 (±2.95) vs CG 6.55 (±5.08), p=0.033) (figure 5). Group differences for the Hospital Anxiety and Depression Scale–Anxiety Subscale (HADS-A) and the total scores were not significant at 6 months (table 3).

Results of the HADS-D for the IG and the CG. P value was obtained from the t-test. CG, control group; HADS-D, Hospital Anxiety and Depression Scale–Depression Subscale; IG, intervention group. *P<0.05.
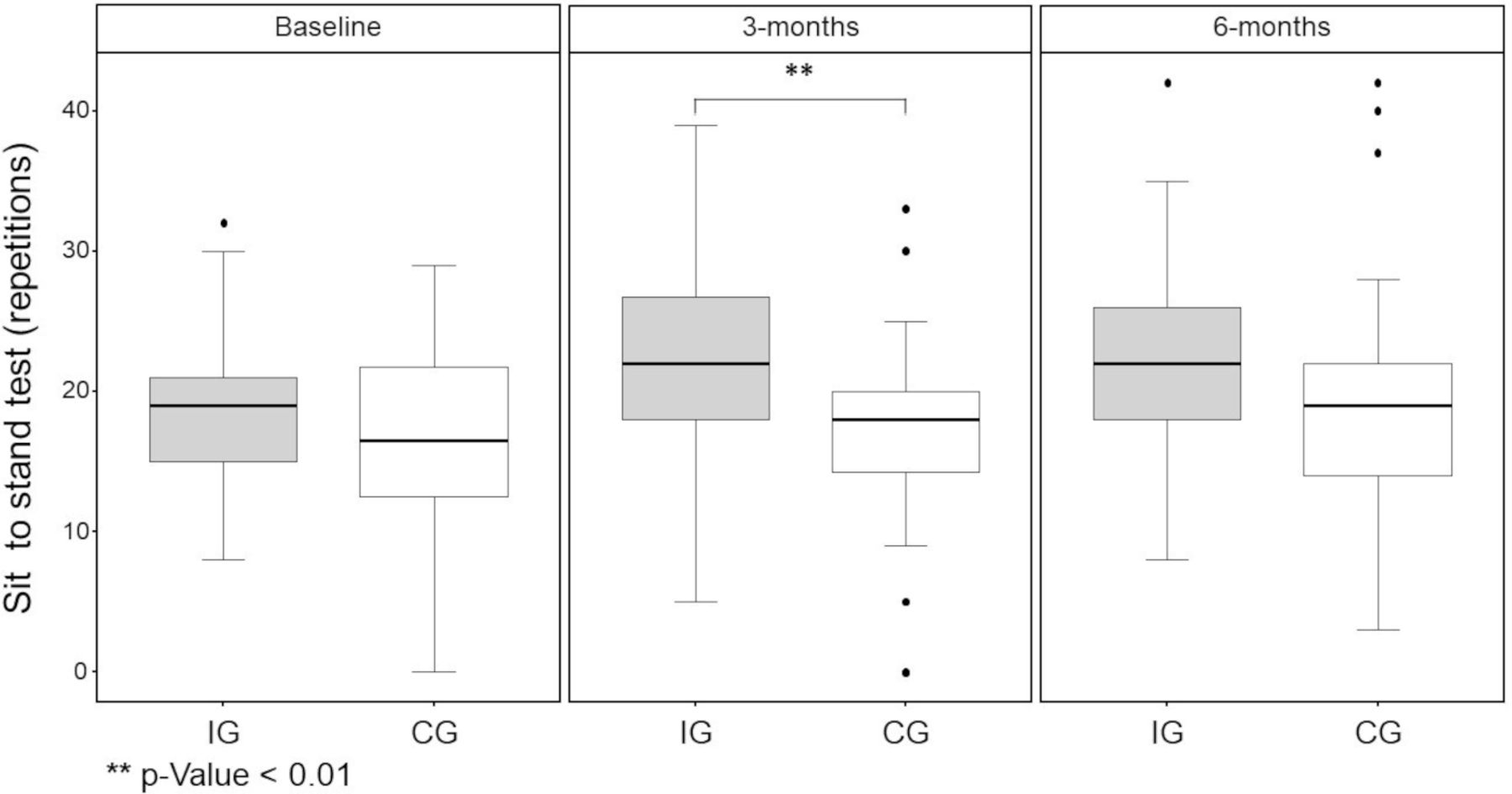
Sit-to-Stand Test
At baseline, no significant difference in the number of STST repetitions was observed. After 3 months, participants in the IG performed a significantly higher number of repetitions, and after 6 months, no significant difference was noted in the number of STST repetitions (figure 6 and table 3).

Results of the 1 min Sit-to-Stand Test for the IG and the CG. P value was obtained from the t-test. CG, control group; IG, intervention group. **P<0.01.
Sleep parameters
Regarding sleep duration and sleep efficiency, no differences were found for both the CG and IG at any time (table 3).
App usage and adherence
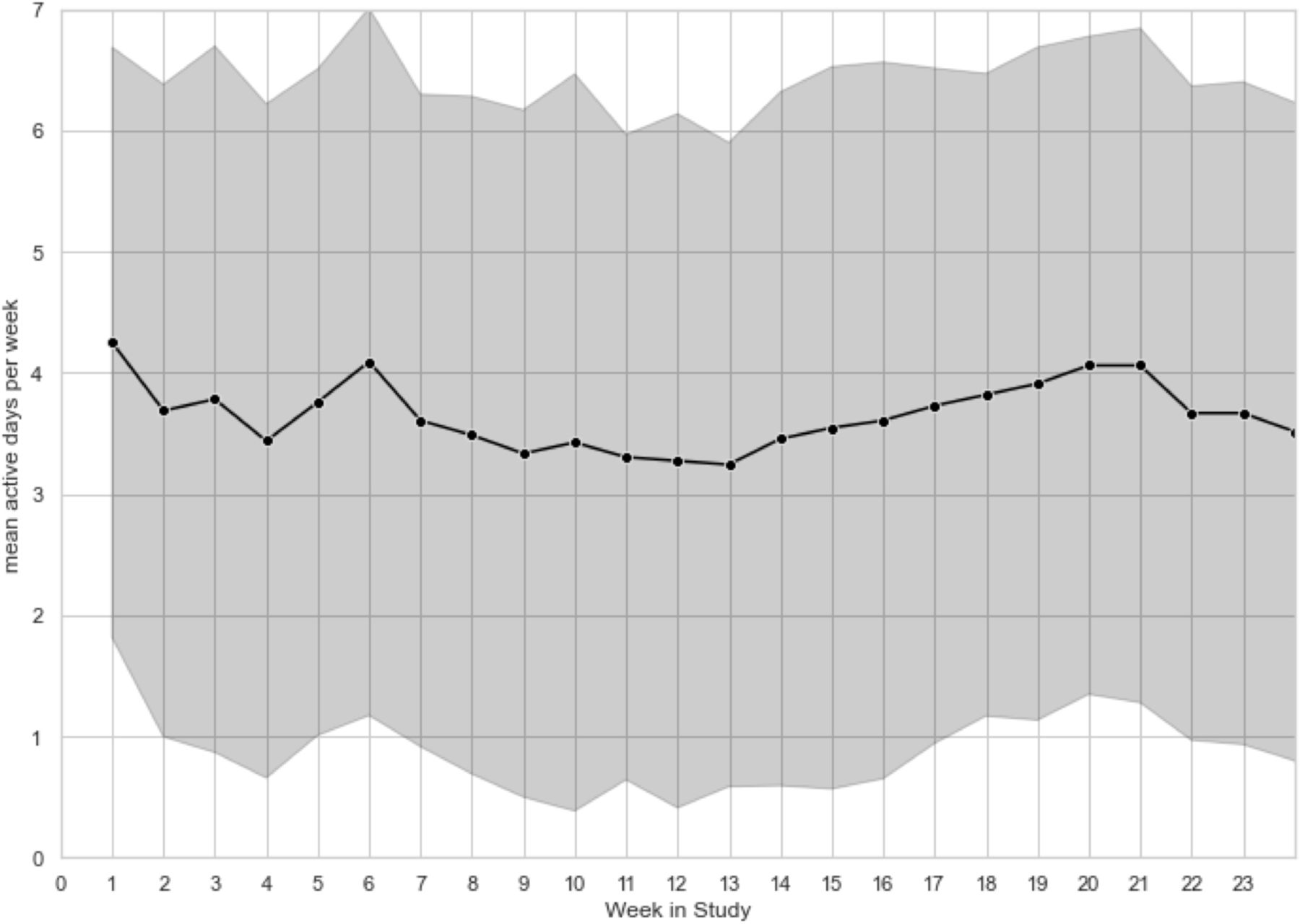
The app usage for the IG is reported in line with adherence to definitions previously reported and listed in table 4.14 A prespecified optimal usage rate of four different types of content, on four different days per week, was achieved by 36% of the participants. Using the prespecified adherence definition (use of the application at least four times a week for at least 70% of the weeks during the study), 13 participants (43%) in the IG complied fully with the app usage suggestions (‘frequent app user’). As a sensitivity analysis, we reanalysed this subgroup of patients and found an even greater difference when compared with controls regarding the primary outcome (change in steps from baseline in the IG 1092.1 (−1036.3 to 2317.9) and in the CG −1173.0 (−3813.1 to −93.8), p=0.006). The results of the subgroup frequent app user are provided in online supplemental table S7). A visual representation of the participants’ app usage is shown in figure 7.
Usage of the COPD app in the intervention group
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Usage rates per week during the observational period. Mean values are indicated by the black line and dots; SDs are indicated by grey bars.
Of the 30 participants, 29 (96.6%) completed the study, indicating that they were satisfied with the study app after using it. Ten (34.5%) participants rated it as ‘okay’, and 18 (62.1 %) rated it as ‘very satisfactory’. All participants would recommend the app to other patients with COPD. There were no differences in safety endpoints. More detailed information regarding safety endpoints is provided in the online supplemental material.
Discussion
The study investigated the effects of a digital-based post-PR programme provided via a smartphone app to maintain the positive results of PR as long as possible and to encourage patients to adopt a more active lifestyle. The results demonstrate that the maintenance of PA and a significant increase in HRQoL, up to 6 months after completing PR, were possible by using a mobile app for self-management of COPD. To our knowledge, this study is the first RCT to demonstrate the maintenance of PA after inpatient PR using a digital structured programme. In addition, differences in favour of the IG could be found in all observed endpoints of the study (except HADS-A) after 6 months, exceeding the minimal clinically important differences (online supplemental material). These positive app results are particularly impressive because the CG received the usual postrehabilitation recommendations rather than no intervention. In addition to the application providing potential benefit of maintenance after participating in PR, it may provide benefit of increasing the uptake of digital delivery of PR overall.
PR has been demonstrated to significantly and reliably improve HRQoL and exercise capacity. However, the long-term effects on PA are moderate. Given its resource-intensive and costly nature, consolidation and maintenance of PR-induced benefits, especially in maintaining PA, remain a challenge across modes of delivery and healthcare systems. Structured exercise programmes aimed to improve the maintenance of benefits after PR showed mixed results when assessing exercise tolerance, HRQoL and PA.28
Additionally, the findings of the current study are of relevance because PA is an important outcome. Previous studies on this topic have shown ambivalent results, and most studies have focused on physical performance as the primary endpoint.7 8 Since a higher exercise capacity does not necessarily lead to higher PA,7 29 it is of particular interest to evaluate the effects of a postrehabilitation programme on PA. Physical inactivity is a potential modifiable risk factor and should be clinically assessed as a vital sign of a patients’ general physical condition prior to any exercise-based intervention.30
In this study, training on the use of the study equipment occurred during rehabilitation (four sessions, each of 20 min duration). When reduced to pure training with the app, the effort would be significantly lower, and a cost-effective and feasible application would be conceivable in the outpatient area. However, the extent to which a reduction in training times has an influence on adherence to the training app cannot be estimated.
Barriers to referral, uptake and completion of PR are well documented and linked with organisational, practitioner and patient-related factors.31 However, the extent to which the use of a training app can close a gap here must certainly be evaluated in further studies. Findings from studies of maintenance programmes following PR are heterogeneous, especially regarding supervision frequency. A recently published Cochrane review including 21 studies with 1799 patients with COPD suggested that supervised maintenance programmes for patients with COPD after PR may improve HRQoL and could possibly improve exercise capacity at 6–12 months. The strength of the evidence was assessed as limited. The authors concluded that the optimal frequency of supervision and mode for supervised maintenance programmes are still unclear.32 However, these studies also predominantly examined only the effects on the participants’ physical performance and not the consequences in terms of PA. Interestingly, no significant changes between CG and IG were seen in the 3-month assessment. We suppose this to be the usual duration that PR effects are measurable. By the extended observation period of 6 months, significant differences between the groups could be seen. Our results confirm the experience of the ATS guidelines, stating that the benefits of PR in the absence of any maintenance strategy appeared to diminish over 6–12 months.3 Another study tried to demonstrate the effects of an mHealth intervention to improve or maintain PA in patients with COPD after PR. However, no differences were observed in PA, functional exercise capacity, HRQoL outcomes or body mass index in patients with COPD using a consumer smartphone-based mHealth intervention.33 The discrepancies between outcomes of the previous study and the current study might be caused by the different settings, as patients in the previous study were enrolled until half a year after outpatient PR, and the different inclusion and exclusion criteria. In addition, differences between study interventions might have played a role.
Other disease-relevant outcomes such as the CAT, HRQoL measured by the dyspnoea and fatigue domains of the CRQ, and data on the mood of the patients assessed with the HADS-D showed a significant improvement in the IG compared with CG. Regarding the STST, a clinically and statistically significant difference was observed at 3 months, while no significant difference was noted at 6 months, which may be caused by the fact that the study was not sufficiently powered to detect such a change in the STST. These findings are in line with the effects observed in a retrospective pilot study of the same application, showing at least a significant improvement in the CAT score and the identical CRQ domains from baseline to the end of the observational period.16 Our results support the findings of North et al, who had previously reported non-inferiority of a mHealth intervention to outpatient face-to-face PR on changes in functional exercise capacity and HrQoL in patients with COPD meeting referral criteria to PR.13 In a recent study among patients with severe COPD, telerehabilitation (delivered though providers instead of an app) also yielded equal results to face-to-face PR.34 Of note, all participants in our study were included following a comprehensive rehabilitation, assuming that the patients were in their best possible condition with little potential for further improvements.
Another pilot study investigated the same intervention as Crooks et al in inpatients with COPD following an exacerbation and found clinically relevant effects on HRQoL and the incidence of exacerbations.14 This study also reported an effect of a digital health intervention on PA, HRQoL and functional exercise capacity. The findings suggest that inpatient populations either are especially prone to profit from these interventions or reflect the well-documented effect of PR following exacerbations, as the majority of the participants of this study also had a history of a recent exacerbation.35
Notably, no significant difference was found between the groups with respect to the number of recorded exacerbations or adverse events (AEs). The intervention had a positive safety profile with a comparable incidence and distribution of AEs across the groups. These results are in line with the findings of the aforementioned Cochrane review showing that supervised maintenance programmes for patients with COPD after PR are not associated with increased AEs.33
However, it is still unknown which patients, in terms of disease progression or demographic properties, benefit the most from digital health apps for PR. Another recent pilot study investigated the use of an mHealth app in a collective of newly diagnosed, mild and moderately affected patients with COPD, but observed no clinically or statistically relevant effect on HRQoL, even if the study was powered comparably to the current study.14 However, in both studies, the patient’s baseline symptoms and demographics were comparable. Crooks et al showed that changes in CAT during the study period were more favourable with higher app usage. In the current study, results of the frequent app user subgroup indicated that increased usage creates greater advantages. Furthermore, this subgroup even increased their PA rather than just maintained it. Hence, it seems that increasing adherence motivation might be a key to achieving favourable results in mHealth app usage by patients with COPD. The finding that uptake of and adherence to digital health intervention is indeed a challenge in patients with COPD was also confirmed.36 It is quite conceivable that the use of the app can be beneficial even without prior rehabilitation. This is the subject of the current study and will be reported in the future.
App usage in the current study was sustained over the observational period in most participants in the IG. In this context, previous trials of digital health interventions for PR have repeatedly shown that adherence to the intervention is crucial for favourable outcomes, but adherence is difficult. Previous studies have reported that 28% of patients do not use an app after 1 month (40% at 3 months).12 13 Long-term adherence of >3 months for digital interventions has only been assessed by a few trials but seems to be a remarkable challenge in those studies with below 20% of participants completing the 6-month programme.37 The long-term usage rates in the current study suggest acceptable patient engagement throughout the observational period.
The observational period of our study suggests that using a digital health tool maintains PA after PR during an observational period of 6 months. This exceeds the observational periods of previous studies that have investigated the effect of digital tools on self-management in patients with COPD, which ranges mostly from 6 to 12 weeks.2 Implementing a long observational period is important since continued use and sustained demonstration of positive clinical outcomes of digital health tools have been described as a problem that needs to be addressed.36
This study has some limitations. First, the sample size was small. However, the statistical considerations according to the primary endpoint assumed a total sample size of 52 patients. In this study, the results of 60 patients were finally analysed, allowing for appropriate interpretation of the primary endpoint. However, in consequence, additional studies with larger sample sizes will help elucidate the effects of the intervention in broader settings. Second, more than three other sites were asked to participate; however, due to several reasons (eg, no sufficient inpatient PR case load in COPD and no adequate research infrastructure), only two sites were eligible. Third, the results of this study may not be generalisable to a broader population of patients with COPD. According to the aim and the defined inclusion criteria of the study, a preselection of patients in the COPD rehabilitation population was necessary, showing sufficient verification in mobile technology. Hence, even though the authors tried to mitigate this by offering smartphones and a corresponding education as part of the intervention, the study was mainly limited to smartphone users.
Fourth, the nature of the intervention made blinding of the study participants and study staff impossible. Although this problem is commonplace in rehabilitation trials, the lack of blinding is a limitation. To reduce the risk of bias, other procedures such as proper allocation concealment were implemented to ensure rigour and reproducibility. Selection bias may have been introduced in the study through the screening criteria which might select for participants compliant with the study intervention; this may have an effect on adherence and patient engagement. Fifth, while the study showed significant benefits of the intervention over an observational period of 6 months, the effects during a longer observational period like 12 months have not been assessed.
Conclusions
Digital interventions are an interesting option to support the management of chronic conditions such as COPD. For these digital interventions to be meaningful, integration into the existing healthcare landscape is paramount, and it may provide benefit of increasing the uptake of digital delivery of PR overall. This study reveals how a digital intervention can be used to supplement existing care by closing gaps in the existing healthcare landscape. However, to make a general recommendation on the benefit of an app as a maintenance programme after PR in patients with COPD, further studies are required.
Data availability statement
Deidentified and aggregated participant data are available from the corresponding author on reasonable request, subject to approval by an independent ethics committee.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Swiss Ethics Committee (BASEC 2019–00766) and the German Ethics Committee of the University of Marburg (number 96/19). The participants gave informed consent to participate in the study before taking part. The investigation conformed to the principles outlined in the Declaration of Helsinki.
Acknowledgments
We thank Editage (www.editage.com) for English language editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MS was the principal investigator for Switzerland and supervised the study, PR programme and data collection; ARK was the principal investigator for Germany. MS, TB, SH, PK-B, A-MP, SS, RG, IJ, TS, DL and ARK contributed to the study concept and design, as well as in the data collection. MS and SH wrote the first draft of the manuscript, which was critically reviewed by RG, PK-B, SS, ARK, WW, IJ, and TS. BU contributed for the statistical analysis. All authors participated in various steps in the study, edited the manuscript and gave their approval for submission. MS is the guarantor of the article.
Funding The clinical study was sponsored by Kaia Health software GmbH.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.