Article Text

Statistics from Altmetric.com
Key messages
What is the key question?
To what extent is chronic pulmonary aspergillosis (CPA) both (a) mistaken for TB and (b) coexists with TB during the course of 6-month therapy?
What is the bottom line?
Features consistent with CPA were present in 6% of patients when starting TB therapy and 8% at the end of therapy, with some resolving and some developing CPA de novo during TB therapy. At the end of TB therapy symptoms, cavitations with Aspergillus-specific IgG detectable were the key features of CPA.
Why read on?
Coexistence of TB and CPA is present in a substantial minority of patients starting and ending TB therapy, and needs addressing in terms of diagnosis, dual therapy and follow-up.
Introduction
The link between pulmonary TB and the subsequent development of chronic pulmonary aspergillosis (CPA) is well established for those who have recovered from TB.1 2 Studies to date have addressed the relative rate of development of CPA with slightly different incidence rates depending on the modes of testing, timing, diagnostic criteria used and the patient population.3–5 No prospective studies have yet addressed the occurrence of both CPA and TB during anti-tuberculous therapy, although a few such cases are described.6 Misdiagnosis of CPA as pulmonary TB is relatively common in clinical practice, but hard to quantify as it is difficult to absolutely rule TB out as a diagnosis.5 No prospective studies of CPA have been done in Indonesia. In 2019, Indonesia reported 845 000 TB cases to the WHO, 87% pulmonary7 so the numerical impact of misdiagnosis could be large.
Once a diagnosis of pulmonary TB is considered based on clinical symptoms, disease duration and radiological appearance, the standard approach and general clinical recommendation is to commence anti-TB therapy. In a review of older studies before the HIV era and before effective therapy for pulmonary TB was available, Tiemersma et al 8 found that even in those with smear-positive TB, the spontaneous recovery was 30% (14%–47%) and in those with smear negative TB was ~80%. So the drive to immediately treat patients with suspected TB is driven by concern for transmissibility, rather than immediate death of the patient. In the era of coinfection of HIV and TB, the 1-year mortality is still excessively high, but this is not the predominant problem in Indonesia.9
This longitudinal study was designed to address the timing of the development of CPA during the course of treated TB. A very common feature of TB is pulmonary cavitation, and we know that this is an important precursor to CPA,2 10 and given that (a) Aspergillus inhalation is inevitable and daily and (b) that some genetic variants of humans are strongly associated with CPA, it would seem likely that some patients might develop CPA early in the course of TB.11 12 This early Aspergillus infection could be progressive, or it could be self-limited in those with adequate immune defences, and in both cases be marked by a raised Aspergillus antibody. This is not currently known.13–15
Furthermore, in those with a clinical presentation of TB, it may be that some patients do not have TB, but an alternative diagnosis. The differential diagnosis includes CPA, non-tuberculous mycobacterial infection, chronic cavitary pulmonary histoplasmosis, coccidioidomycosis or paracoccidioidomycosis, pulmonary cryptococcal infection, necrotising lung cancer, pulmonary hydatid disease, actinomycosis or a subacute bacterial infection on a background of bullous emphysema which appears radiologically similar to TB.16–19 Histoplasmosis is endemic in Indonesia, but coccidioidomycosis and paracoccidioidomycosis are not, so only international travel would allow these infections to manifest.20 We hypothesised that some smear-negative and TB PCR-negative patients might have CPA and not TB, as described in Nigeria by Oladele et al.5 By excluding patients with those previously treated for TB (based on the medical records and verbal confirmation from patients), we have taken out of consideration other populations of patients who might have CPA or a broader differential diagnosis.
Our primary objective was to determine the incidence of CPA during the course of and at the end of TB therapy, and to assess if the criteria for CPA diagnosis are suitable for this population of patients who are already ill with TB. A second objective was to assess how many patients who are thought to have TB, but lack microbiological evidence for this, actually have CPA and how many have dual infection. We also hoped to determine if any patients had ‘self-resolving CPA’, or ‘subclinical CPA’ which does not progress, entities not yet adequately described in the literature and which challenge the current general concept of CPA as a progressive disorder.21 Our hypotheses are that: CPA is common and underdiagnosed in patients with TB in Indonesia, there is dual infection between CPA and TB, CPA starts to develop during active infection of TB and the current diagnostic criteria for resource-constrained settings are applicable in Indonesia.
Methods
Study population
This was a prospective, longitudinal study. Patients were enrolled at two tertiary care hospitals (National Referral Centre Persahabatan Hospital and National Referral Centre Cipto Mangunkusumo Hospital) and four district hospitals (Grha Permata Ibu Hospital, Universitas Kristen Indonesia Hospital, Cempaka Putih Jakarta Islamic Hospital and MH Thamrin Hospital), serving greater Jakarta (12 million). Patients were referred from primary care because of diagnostic uncertainty, patient request or comorbidity.
All consecutive consenting patients with newly diagnosed pulmonary TB were recruited into the study. The exclusion criteria were history of TB, multidrug-resistant TB, less than 16 years of age and non-consenting patients.
PulmonaryTB was diagnosed by the attending clinical team based on typical symptoms, positive TB PCR by GeneXpert MTB/RIF (Cepheid, California, USA) and/or acid fast bacilli (AFB) smear and/or radiology finding positive for TB, as per national guidelines.22 Culture for Mycobacterium spp was not done, except in exceptional circumstances. Many patients were treated empirically if the suspicion for pulmonary TB was high.
Data collection
Patients were assessed at the start of TB therapy (baseline, 0–8 weeks) and at the end of TB therapy (at 5–6 months). The main variables, collected at both time points, were serum Aspergillus-specific IgG levels, symptoms and quality of life scores.
A validated quality of life instrument used in respiratory disease—the St Georges Respiratory Questionnaire (SGRQ)—was used in addition to CPA-specific questions.23–25 This questionnaire consists of three domains (activity, impact and symptoms, each with range of 1–100) and high scores reflect worse quality of life.
Sample collection and processing
Blood samples (5–10 mL) and sputum (if produced) were collected from patients in the clinic at both time points. Aspergillus-specific IgG level was measured using the Immulite 2000 system (Siemens, Berlin, Germany) according to the manufacturer’s instructions using a cut-off of 11.5 mg/L.26 Prior to testing, serum was stored in −80°C. Sputum from patients with productive cough was tested for TB using GeneXpert MTB/RIF PCR. AFB smear results were collected from patients’ medical records. Any remaining sputum was cultured for fungi.
Radiological interpretation
All patients had a chest radiograph at baseline and end of TB therapy. CT scans were also done for patients who could afford them. All images were digitised and reviewed by an experienced radiologist (FN) who coded the appearances systematically and provided a narrative report. All radiographs were also reviewed by one of the authors (DWD) who specialises in aspergillosis. All radiographs were interpreted in the absence of data on symptoms or any laboratory findings or the interpretation of the other reviewer. The presence of pleural thickening adjacent to a cavity was required to suspect CPA, as opposed to anywhere on the radiograph—the only finding where there was some difference between the two reviewers who were in agreement for all other criteria.
Definitions
Proven CPA was diagnosed based on three criteria: (1) at least one of the following symptoms—cough, haemoptysis, chest pain, dyspnoea, fatigue, and/or weight loss ≥3 months, AND (2) radiological features indicative of CPA (cavitation, fungal ball or pleural thickening) and/or progressive cavitation on serial chest radiographs, AND (3) positive Aspergillus IgG and/or Aspergillus spp detected by culture. The diagnosis of probable CPA was made when criteria 1 and 2 but not 3 were met AND (4) the PCR for M. tuberculosis was negative. Possible CPA was diagnosed in those who met criteria 1 and 2 but not 3 or 4. Criteria for proven, probable and possible CPA were modified versions from Denning et al.15 ‘CPA’ in the tables and text refers to proven CPA, unless otherwise stated.
Data analysis
Statistical analysis was performed with the use of IBM SPSS V.25 statistic software. A p value of <0.05 was considered statistically significant. Data were presented using frequencies and percentages for binary and categorical variables, medians and range for non-normally distributed, continuous variables. The difference between non-parametric continuous variables was analysed using Mann-Whitney U test for CPA and non-CPA groups. Fisher’s exact tests or Χ2 tests were used for categorical variables for CPA and non-CPA groups. Comparisons of median results across different time points were assessed by Wilcoxon signed-rank test. In addition, post hoc analyses were carried out with McNemar’s test with adjusted Bonferroni corrections between two time point comparisons.
Results
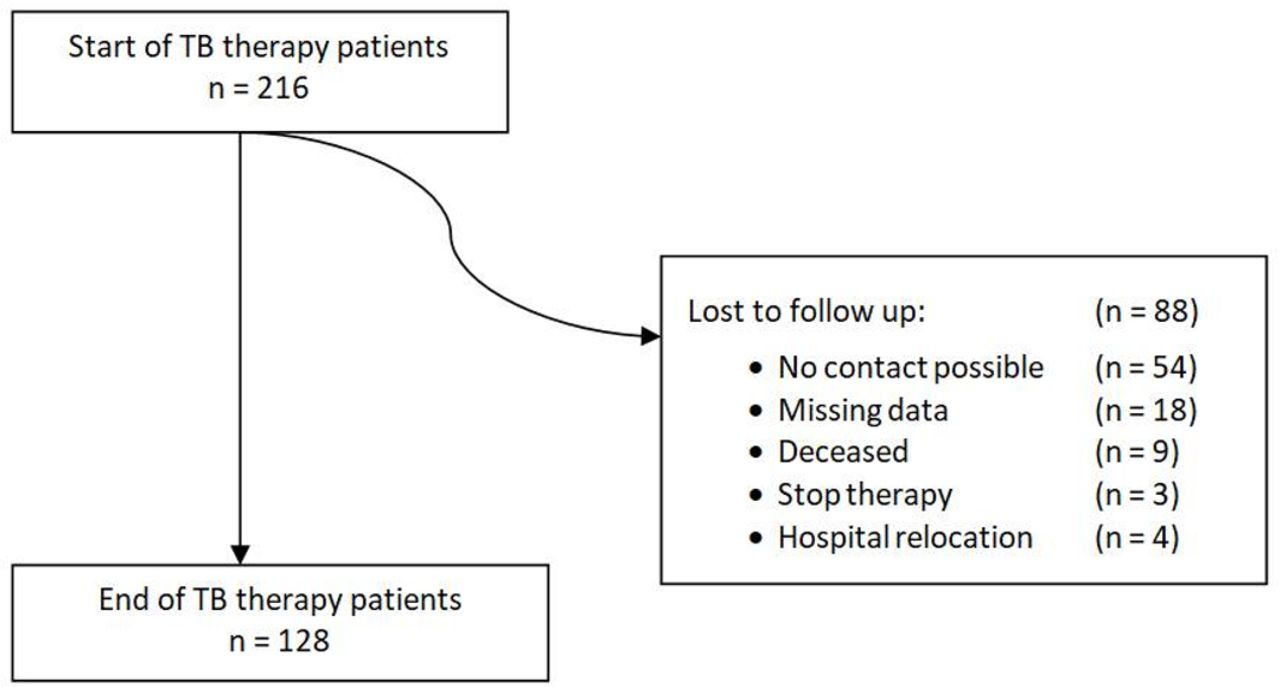
A total of 216 patients with pulmonary TB were recruited at the start of their TB therapy and 128 (59%) patients reattended the end of TB therapy follow-up appointment (figure 1). The recruitment phase for the baseline appointments is from February 2017 until April 2018. At baseline, 91 (42%) of 216 patients had microbiological evidence for TB (positive TB PCR and/or AFB smear), 91 (42%) patients were clinically diagnosed as TB but had no microbiological evidence of it (negative TB PCR and/or AFB), and 34 (16%) patients were clinically diagnosed as TB but microbiological diagnostics had not been performed. Additional two patients had a positive TB PCR result at the end of TB therapy. Twelve (6%) patients met the criteria of proven CPA, 5 (2%) patients as probable CPA and 15 (7%) patients as possible CPA, an incidence of 7.9% (95% CI: 4.7% to 12.3%) or 14.4% if possible cases are included. Six patients grew Aspergillus in sputum culture, two of whom met the criteria of possible CPA. None of the patients with proven CPA grew Aspergillus in their sputum.

Overview of the study population.
Men outnumbered women in CPA cases with a 3:1 ratio (table 1). Diabetes mellitus appeared to be a significant risk factor for CPA at baseline assessment (p=0.040, relative risk=3.346, 42% in patients with CPA vs 16% in patients without CPA). There was a significant difference in the proportion of cough (93% in patients with CPA vs 13% in patients without CPA), fatigue (42% in patients with CPA vs 8% in patients without CPA), and weight loss (17% in patients with CPA vs 1% in patients without CPA) between CPA and non-CPA cases (p<0.05). Baseline quality of life SGRQ scores are shown in table 2. There was a significant difference between patients with CPA and patients without CPA in SGRQ in the symptoms domain (p=0.029, median 58 (CPA) vs 39 (non-CPA)). Cavitation (92% in patients with CPA vs 52% in patients without CPA), air fluid level in cavities (50% in patients with CPA vs 22% in patients without CPA) and pleural thickening (84% in patients with CPA vs 27% in patients without CPA), were all more common in CPA cases (p<0.05) (table 1).
Patients’ characteristics at baseline assessment
IgG tests and SGRQ results at baseline
The overall prevalence of Aspergillus-specific IgG positivity was 30% (64 of 216) at baseline. All (n=12) patients from the CPA group had positive levels of Aspergillus-specific IgG. In the non-CPA group, 52 (26%) patients showed positive Aspergillus-specific IgG. There was a statistical significance between positive Aspergillus-specific IgG across CPA and non-CPA groups (p<0.001, median 15.4 (CPA) vs 8.3 (non-CPA)) (table 2).
Nine (4%) patients died before the end of their TB therapy appointment. Eight of them (90%) had extensive infiltrates and/or cavitation in both lungs. Immulite Aspergillus-specific IgG level was positive in four (44%) of these patients. Chronic kidney diseases (n=3, 33%) and diabetes mellitus (n=1, 11%) were linked to mortality. One patient with possible CPA with multicavitary TB disease died with no other underlying disease. There were no deaths in patients with proven and probable CPA.
At the end of TB therapy, those assessed (n=128) had a similar spectrum and frequency of symptoms with the exception of fatigue (60% vs 13%, p=0.001) and cough (50% vs 11%, p=0.005) which were more common in CPA (table 3). The overall prevalence of Aspergillus-specific IgG positivity was 52% (66 of 128). Ten of 128 patients had CPA, an incidence of 7.8% (95% CI: 7.9% to 20.4%). All (n=10) patients from the CPA group had positive levels of Aspergillus-specific IgG. In the non-CPA group, 45 (42%) patients showed positive Aspergillus-specific IgG. Immulite Aspergillus-specific IgG level increased in patients with CPA compared with patients without CPA (p<0.001, median 24.2 (CPA) vs 9 (non-CPA)). Quality of life scores dropped dramatically during TB therapy, reflecting improved well-being, from a median of 35.9 to 4.8 for overall score (p<0.001) (table 4). However, this drop was smaller in those with proven CPA (62% decrease in SGRQ total score) than in those without CPA (91% decrease in SGRQ total score). Radiological findings improved during TB therapy with the exception of pleural thickening, and the interval development of one aspergilloma (table 3). There was also a slight increase in bronchiectasis (on plain radiography).
Results for end of TB therapy assessment compared with baseline for all those assessed at both time points, using the CPA categorisation at the second time point
IgG tests and SGRQ comparisons for all patients assessed at baseline and at end of TB therapy, using the CPA categorisation at the second time point
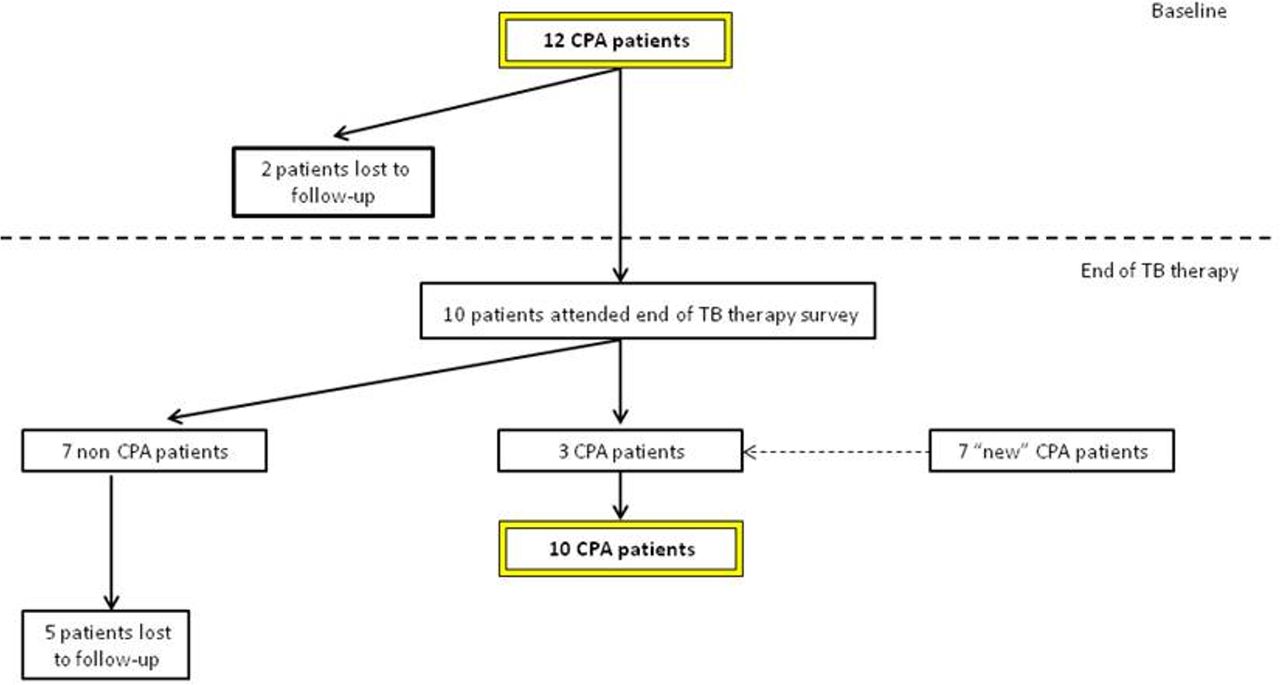
Of the 12 patients with features of CPA at baseline, 7 (58%) were categorised as non-CPA cases at the end of TB therapy without any antifungal therapy or surgery. This was mainly due to decrease in symptoms and in infiltrates seen in chest X-rays (figure 2). Two (17%) were lost to follow-up and not assessed. The remaining three patients continued to have CPA features at the end of TB therapy. An additional seven patients developed CPA during their TB therapy, resulting in a total of 10 (8%) CPA cases at the end of TB therapy. The risk of developing CPA during TB therapy appears to increase with age (p=0.004, mean 52 years (CPA) vs 37.1 years (non-CPA)) (table 3).

{kind=link}
{kind=link}
Patients with CPA during two time point assessments. CPA, chronic pulmonary aspergillosis.
Of five probable CPA cases at baseline, two improved clinically (resolution of symptoms) and one patient became a possible CPA with decreased persistent symptoms but stable pleural thickening by the end of TB therapy. Two patients were lost to follow-up. Of 15 possible CPA at the baseline, 1 patient improved clinically, another met the criteria for probable CPA and 3 patients did not have features of CPA cases at the end of TB therapy assessment; 10 patients were lost to follow-up. At the end of TB therapy, probable CPA and possible CPA were detected in seven (5%) patients and four (3%) patients, respectively. The clinical and radiology profiles of patients at both time points are compared in tables 3 and 4.
Discussion
The incidence of proven and probable CPA was 7.9% (95% CI: 4.7% to 12.3%) at baseline and increased to 13.3% (95% CI: 7.9% to 20.4%) at the end of TB therapy, although the latter figure is marred by substantial loss of follow-up, including some deaths, probably of CPA, between these two time points. There are three confounding factors that need to be considered when interpreting this finding. First, different patients met the criteria for CPA diagnoses at baseline and end of TB therapy. Second, a notable number of patients were lost to follow-up. Third, the accuracy of the CPA diagnosis is a challenge with 5 patients with probable CPA and 15 patients with possible CPA at baseline and 7 probable and 4 possible at the end of TB therapy. Furthermore, some patients had aspergillomas visible on their chest radiograph without clinical or serological features of CPA; five at baseline and one at the end of TB therapy. If all these patients are assumed to have CPA (which is unlikely for the possible group), the incidence of CPA was 17% both at baseline and at the end of TB therapy. Nevertheless, it is likely that the true prevalence of CPA during the course of treatment of TB is somewhere between 6% and 17% at baseline and 8% and 17% at the end of therapy, in Indonesia. These are the first estimates of CPA incidence during anti-TB therapy made globally.
One of the study objectives was to determine how many patients have dual infection. Coinfection of active pulmonary TB and CPA is reported in previous studies.6 27–29 Our data indicate more frequent dual infection than previously thought. However, many of these patients appear to resolve their Aspergillus infection and had ‘self-resolving CPA’. Several other patients failed to attend the second assessment, so their fate is uncertain. The cause of death in those lost to follow-up in our study was uncertain, including determining whether any patients with dual infection died before assessment. In Japan, the term chronic progressive pulmonary aspergillosis was coined to separate those who deteriorated from those who remained clinically and radiologically stable.21 We have clear-cut evidence of this divergence of disease behaviour in this study.
Male sex was an independent risk factor for CPA in this study. Earlier studies also showed male predominance in CPA compared with Aspergillus colonisation in Japan,30 and in a large CPA cohort in Manchester.25 It can be speculated that this is due to a higher prevalence of other risk factors such as smoking, but supportive data are lacking.
Prior studies have demonstrated that the rate of CPA in post-TB therapy populations varies between 4.9% and 14.3%.2 10 In Nigeria, the CPA rate was reported to be 8.7% at the end of TB therapy5 and in Uganda, 9% of HIV-infected patients had Aspergillus-specific IgG detectable at the end of TB therapy.31 A cross-sectional study from Iran reported 13.7% of 124 HIV-negative TB patients developed CPA (76% patients were on active TB treatment).4 All of these CPA rates are within the ranges of our study. However, these studies provide no or minimal information about the status of the patients at baseline and reflect pooled patient populations assessed at varied time points after TB therapy.2 10
One element of the diagnosis of CPA is symptoms for ≥3 months (weight loss and/or cough and/or haemoptysis).15 But as can be seen, this definition component is challenged by our data. TB gives rise to weight loss and cough and many patients have some degree of haemoptysis. We found the relative frequency for CPA and TB to be: cough 93% vs 13%, fatigue 42% vs 8% and weight loss 17% vs 1%, respectively (table 1). Three months of cough is more discriminatory than any cough. Fatigue has been studied and a score devised for patients with COPD applied to patients with CPA appears to be useful, but has yet to be translated into routine clinical practice.32 Chest pain appeared to be a useful discriminator in Nigeria but was only present in 25% of patients with CPA.5 Three months of haemoptysis was found in only 8% of patients with CPA, compared with 1% with TB, but shorter periods of haemoptysis were common and not very discriminatory (table 1).
In addition to specific symptoms, the SGRQ quality of life score was recorded at baseline. Unremarkably for patients with TB, scores were moderately high (table 2), but not at all discriminatory between those with only TB and those with CPA and TB, at baseline. However at 4–6 months after starting anti-tuberculous therapy, those with CPA had persistently raised SGRQ scores in all domains, and there was almost complete resolution of all symptoms in those without (table 4). Therefore, this score might be very useful in Indonesia for identifying CPA at the end of anti-TB therapy. It is worth noting that the SGRQ scores in this study are remarkably low compared with other patients who have recovered from TB in the USA,33 but not Papua, Indonesia.34
The radiological appearances of CPA and TB partially overlap, with upper lobe predominance and cavitation. While TB does not usually cause pleural thickening in the apices, consolidation can occur which can appear like pleural thickening. Likewise pericavitary infiltrates are very typical of CPA, but local consolidation can mimic these findings too. The first description of an aspergilloma by Deve in 1938 described a huge cavity with a fungal ball, which is unmistakable, but more subtle findings are now understood to be typical of CPA.35 The typical appearance of a fungal ball or aspergilloma includes the air crescent or air meniscus sign, first described in the context of pulmonary hydatid disease.36 37 Our study lacks confirmation from CT of the findings seen on chest radiographs in 97.7% of patients. This is a clear-cut study weakness and arises primarily from a lack of funds to afford CT scanning for most patients and an inability to identify in real time those whose disease required better anatomical definition with CT, as serology was done in batches months after the patients were seen.
There is intrinsic uncertainty in the interpretation of chest radiographs. Concordance between readers is far from 100%, both in ascertaining cavitation in TB (50%–70%) and in aspergillosis.38 39 Our radiographs were read by an experienced radiologist in Indonesia (where the only aspergillosis radiological diagnosis made currently is an aspergilloma) with confirmation by a highly experienced clinician focused on pulmonary aspergillosis. Separating CPA from TB with a chest radiograph alone with any certainty is not possible.
Partly using this dataset (end of TB therapy only), and a separate cross-sectional study population (n=71) and both normal and disease controls (n=190), we derived the optimum cut-off for Aspergillus-specific IgG (11.5 mg/L) in Indonesia for the Immulite assay.26 The antibody titres varied substantially between both time points, indicative of a complex interaction between Aspergillus and the immune system during the months of anti-TB therapy.
The presence of an aspergilloma is highly indicative of CPA, with echinococcus and necrotising lung tumours really the only differential diagnoses. An aspergilloma may represent a single aspergilloma, without symptoms or be a feature of chronic cavitary pulmonary aspergillosis. In this study, aspergillomas were detected in 11 patients, with 8 (72.7%) patients having positive PCR TB and/or AFB smears at baseline, indicating coinfection of Aspergillus in patients with active TB. Five (45.5%) patients had positive Aspergillus-specific IgG by Immulite, four (36.4%) patients in the end and/or post TB therapy and one (9.1%) patient showed persistent positive Aspergillus-specific IgG by Immulite but with no accompanying symptoms. Two patients had CT scan-confirmed aspergilloma, both with bacteriologically confirmed TB.
In most patients with aspergillomas, Aspergillus IgG was negative when first seen and most were therefore classified as non-CPA. Seroconversion of Immulite from negative to positive Aspergillus-specific IgG occurred in all five patients with persistent aspergilloma. Aspergillomas with negative A. fumigatus IgG antibody have been observed in Africa and may relate to non-fumigatus infections or a muted antibody response.2 5
The other study objective was to determine how many patients are misdiagnosed as TB when in fact they have CPA. Ruling out TB can be difficult, so complete confidence in this assertion for individual patients is usually difficult. Community-acquired Aspergillus community-acquired pneumonia (CAP) without any evidence of immunocompromise can occur,40 41 often following significant environmental exposures such as bark chippings, compost and gardening.42 43 Some of these patients fail to completely resolve their Aspergillus infection, and if they do not die develop CPA. It is highly likely that some of the clinically diagnosed cases of TB in this study with positive Aspergillus IgG had community-acquired Aspergillus CAP and some went on to develop CPA.
We therefore propose that CPA should be included as an alternative diagnosis of pulmonary TB, especially if there is no clinical and radiological improvement after starting TB therapy. Pulmonary TB and CPA may coexist and both diseases require their own management plan. In the context of non-tuberculous mycobacterial infection and CPA, the outcomes of those with dual infection were much worse (11.5-fold increased mortality);19 this has yet to be ascertained for those with TB. The availability of Aspergillus antibody testing and CT scanning is an important component of optimal CPA diagnosis. This study is important for the future study of CPA in Indonesia. As an alternative or coexisting disease in patients with TB in Indonesia, CPA is important for clinicians and also to galvanise social and political will of multiple stakeholders to support improvement of diagnostic capacity of fungal disease in Indonesia.
Data availability statement
Data are available upon reasonable request. All data are available if requested.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Research Ethics Committee of the University of Manchester (approval number 16416) and from the Ethics Committee of the Faculty of Medicine, Universitas Indonesia (approval number 672/UN2.F1/ETIK/2016).
Acknowledgments
We would like to thank all the staff at the Department of Parasitology, Faculty of Medicine University of Indonesia for their help in sample storage and testing of sputum samples. We gratefully acknowledge Dr John Belcher of the Department of Medical Statistics for statistical support. We would also like to acknowledge support from the staff at the Mycology Reference Centre Manchester for providing training of manual Aspergillus-specific IgG ELISA tests and support throughout the project.
References
Footnotes
FS and AR are joint first authors.
Twitter @dwdenning
Contributors The study was coordinated and analysed, and the first draft written by FS. RR-R, AR, RW and DWD contributed to study design. AR, RA, RS, MT, CS, FN, JR, ARA, DH, EB, MR and RW all contributed to patient recruitment, data acquisition, sample analysis and radiological interpretation. DWD conceived the study, analysed all the radiographs, contributed to data analysis and paper drafting, and acts, with FS and AR, as guarantor of the study's integrity.
Funding The scholarship to support the studies of the first author was provided by Lembaga Pengelola Dana Pendidikan (20160222045506), Republik Indonesia. DWD is partly supported by the NIHR Manchester Biomedical Research Centre.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.