Article Text

Abstract
Inorganic antigens may contribute to paediatric sarcoidosis. Thirty-six patients matched with 36 healthy controls as well as a group of 21 sickle-cell disease (SCD) controls answered an environmental questionnaire. Patients’ indirect exposure to inorganic particles, through coresidents’ occupations, was higher than in healthy and SCD controls (median score: 2.5 (0.5–7) vs 0.5 (0–2), p=0.003 and 1 (0–2), p=0.012, respectively), especially for construction, exposures to metal dust, talc, abrasive reagents and scouring products. Wood or fossil energies heating were also linked to paediatric sarcoidosis. This study supports a link between mineral environmental exposure due to adult coresident occupations and paediatric sarcoidosis.
- sarcoidosis
- paediatric interstitial lung disease
- occupational lung disease
- rare lung diseases
Statistics from Altmetric.com
Introduction
Paediatric sarcoidosis is extremely rare with only three reported cohorts1 : Danish (Caucasian), French (Afro-Caribbean) and Louisiana (Afro-American) patients. Most patients were aged 11–13 years. The disease seemed severe in children, involving multiple organs, and often persistent in adulthood.1 2
Granuloma formation in sarcoidosis might stem from an exaggerated inflammatory response to organic or inorganic environmental antigens in genetically predisposed patients.3 4 Beryllium or crystalline silica have been associated with ‘sarcoidosis-like’ diseases.5 This environmental factor is sustained by molecular studies involving foreign body reaction pathways such as autophagy in sarcoidosis.6 The PEDIASARC study aims at comparing the exposure to inorganic—mineral—particles in patients with paediatric-onset sarcoidosis to controls.
Methods
PEDIASARC was a retrospective, multicentric, case–control study from 2015 to 2019. Patients whose sarcoidosis began before the age of 16 were recruited in the French Reference network for rare lung diseases (RespiRare), without calculation of a suitable sample size. The diagnosis was confirmed by histology (91.7%) or multidisciplinary expert discussion. A control group of healthy children was matched by age ±2years and sex. In order to have a control population closer to the characteristics of the patients in terms of geographic origin, family migration experience, socioeconomic and genetic background, a second control group was recruited among patients with sickle-cell disease (SCD). Patients and controls and/or their adult representatives gave their consent and answered a detailed environmental questionnaire (online supplemental files 1,2) that evaluated inorganic exposures from birth to the age at sarcoidosis onset in both patients/controls and their coresidents. Questions targeted living habits, occupational and non-work-related environmental exposures (hobbies, housing), particularly crystalline silica, talcum, wood dust, mould, pollution or metal dust. Each phone or face-to-face interview lasted 45 min. The environmental exposure score combined a direct score measuring patients’ or controls’ exposures, an indirect score measuring occupational and non-work-related activities and a housing score related to in-house exposures (online supplemental figure S1). Each exposure scored 1 point. Each exposure was compared between the three groups (n, percentage). A median score and an interquartile range (IQR: 25–75) of each group were calculated for each global exposure (direct, indirect, housing) and they were compared using a Wilcoxon-Mann-Whitney test. The housing score was divided by the number of questions. The study was authorised by French legal authorities (CPP, comité de protection des personnes; CNIL, commission nationale de l'informatique et des libertés).
Supplemental material
Supplemental material
Results
Among the 53 patients with paediatric-onset sarcoidosis of the RespiRare network, 14 could not be reached, 3 refused to participate and 36 (68%) patients—mostly from Sub-Saharan and Afro-Caribbean origins—were included in the study (table 1 and online supplemental table S1). None of the patients had to be excluded because of an absence of understanding of the questionnaire. They were matched with 36 paired healthy controls—mostly from Caucasian origin. Twenty-one SCD controls could be included.
Clinical features of the included patients and controls
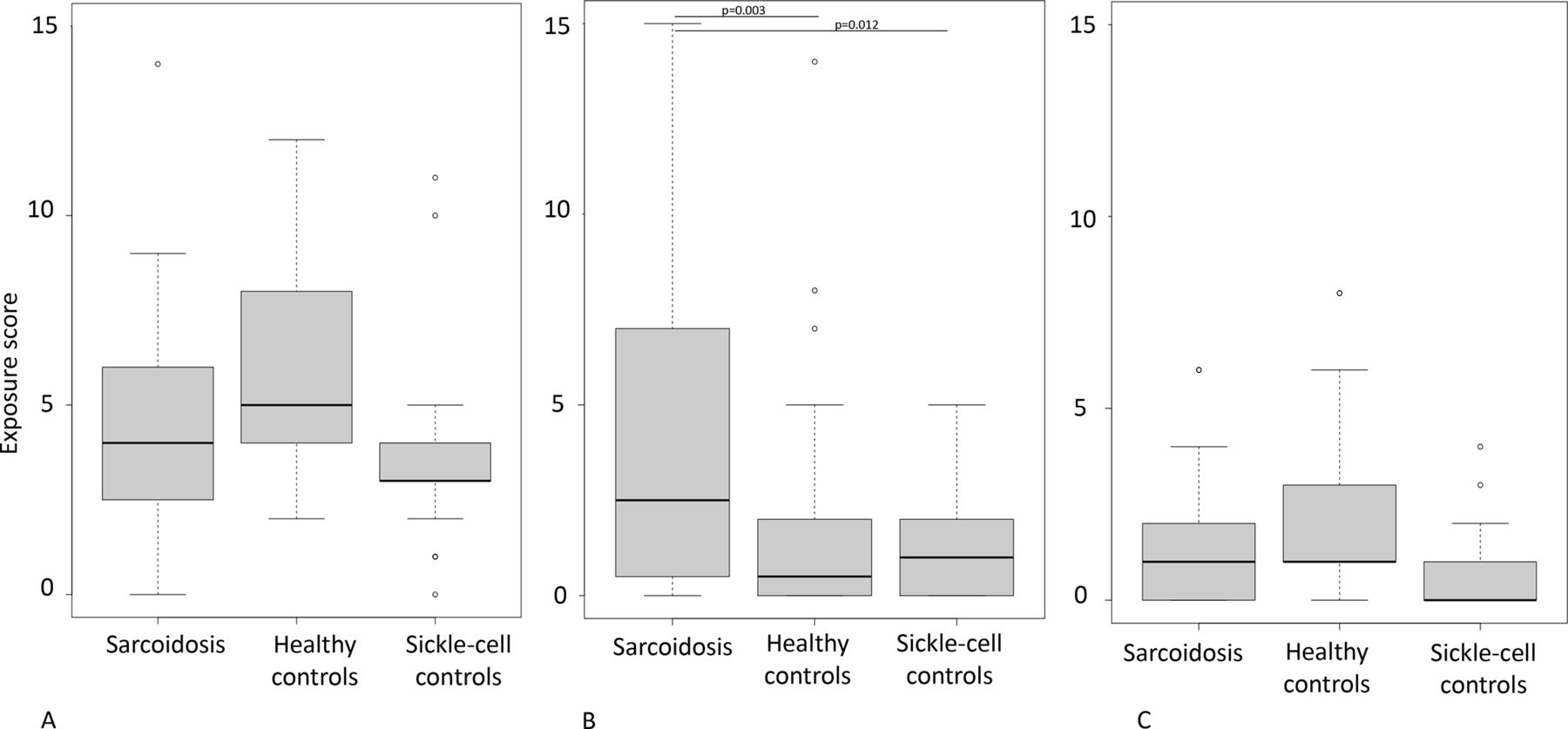
Direct exposure scores did not differ between the three groups (figure 1). Exposure to scouring powder was the only one to be higher in patients’ environment as compared with healthy controls (p=0.037) (online supplemental table S2). The global indirect exposure score was significantly higher in the sarcoidosis group than in the SCD group (5.5 (1.75–9), 2.5 (1–5.25) (p=0.09), 1 (1–3) (p=0.009)), respectively for the sarcoidosis, healthy controls and SCD controls. The occupational exposure score of the patients’ coresidents (whose number was similar among the three groups (table 1)), was higher than in both control groups (median scores 2.5 (0.5–7)) versus (0.5 (0–2), p=0.003 for healthy controls and 1 (0–2), p=0.012 for SCD controls), particularly exposure to abrasive material (silica), talcum, combustion or welding fumes in metal working industry. The coresidents were exposed to mineral dusts via construction works and cleaning with scouring reagents. Only the frequency of occasional do-it-yourself was found different between patients and controls regarding coresidents’ non-work-related activities (online supplemental table S3) and figure 1.
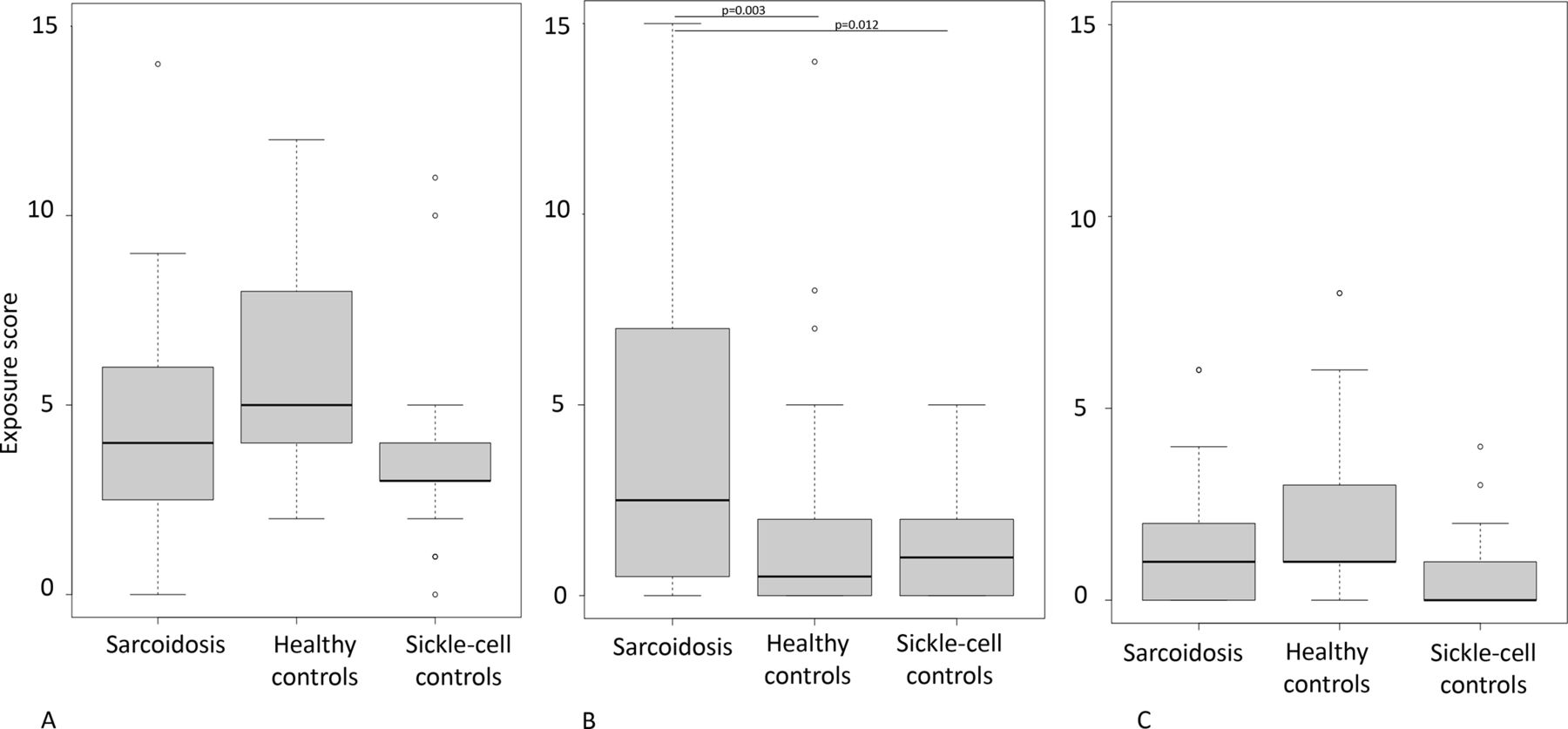
Exposure scores of the patients and the controls. (A) Direct exposure score, (B) indirect exposure score due to occupational activities and (C) indirect exposure score due to non-work-related activities of the patients and controls. The box represents the interquartile range (the lower line of the box represents the 1st quartile, the horizontal line within the box is the median and the upper line is the 3rd quartile), the horizontal bars at the ends are the minimum and maximum values and the isolated points represent are the extreme (exceptional) values. The theoretical maximal scores are as follows: direct exposure score = 26, indirect exposure score = 27, indirect extraprofessional exposure score = 15. The indirect exposure score due to occupational activities was higher in patients than in both control groups. No difference was found for the direct exposure score and the indirect exposure score due to non-work-related activities of the patients and controls. *p<0.05.
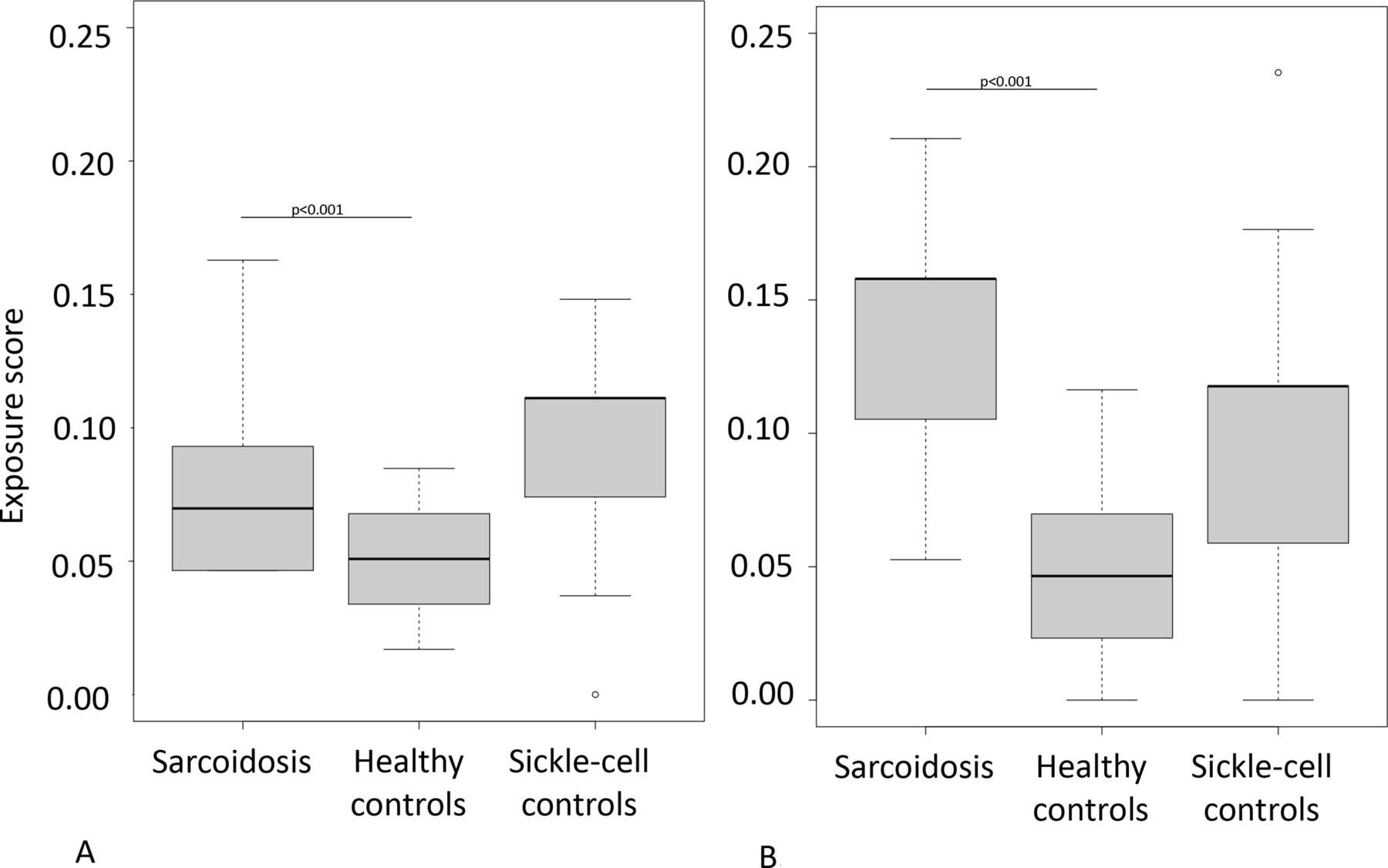
The exposure score related to the current and previous housings was significantly higher for patients as compared with healthy controls (median scores: 0.069 (0.05–0.1) vs 0.05 (0.04–0.07), and 0.16 (0.11–0.16) vs 0.04 (0.025–0.065), p<0.001 for both current and previous housings) but not with SCD controls (median scores: 0.11 (0.08–0.11), p=0.3 and 0.118 (0.06–0.12), p=0.13, respectively) (figure 2 and online supplemental table S4). Wood, gas, butane, coal and fuel oil heating were more frequently reported by patients than healthy controls and SCD controls. In patients’ previous housings, mould was more frequently present than in healthy controls but not in SCD controls (online supplemental table S5).
{kind=link}
{kind=link}
Housing exposure score. Exposure scores of the current (A) and previous (B) housing of the patients and controls. The housing scores were divided by the number of questions. The box represents the interquartile range (the lower line of the box represents the 1st quartile, the horizontal line within the box is the median and the upper line is the 3rd quartile), the horizontal bars at the ends are the minimum and maximum values and the isolated points represent the extreme (exceptional) values. The exposure scores were significantly higher for patients as compared with healthy controls but not with sickle-cell disease controls. *p<0.001.
Discussion
Our study is the first one supporting the fact that the adult coresidents’ occupational exposure (especially crystalline silica, metal and talcum—the toxicity of which has already been put forward) could play a promoting role in the pathophysiology of paediatrics sarcoidosis, whereas direct exposures at a paediatric age would not. We found that hazardous occupations were those releasing a lot of dust, especially in construction.7 These results are consistent with those produced in adults in the ACCESS study and the French pilot MINASARC study using also bronchoalveolar lavage (BAL) analysis of mineral dusts.4 8 More recently, a Dutch study highlighted an increased exposure but also an increased immunoreactivity to metal and silica in adult sarcoidosis patients.9
As in the USA, paediatric sarcoidosis in France affects mostly black children.1 The patients’ histories often highlighted chaotic migratory trajectories, successive insalubrious homes, and parents having numerous short-contract occupations, few exposing hobbies and other extraprofessional social activities. Thus, our results could be only a characterisation of the patients’ socioeconomic status, without this being an aetiological determinant for paediatric sarcoidosis. Since (1) the SCD control group allows checking social characteristics and (2) the housing score is not significantly different in patients and in the SCD control group, we consider that our results uncover findings specifically linked rather to paediatric sarcoidosis, than to socio-economic status.
Several studies have suggested that a genetic susceptibility could promote sarcoidosis. Moreover, Sub-Saharan Africa populations are more often affected.3 Despite probable similar exposures within families, only 3 (8.3%) kin-related sarcoidosis were reported. This observation questions the way how environmental exposure and genetic combine. The expansion of ongoing genetic family and trio studies may undoubtedly help to answer this question.6 10
Despite several limitations (small population size—as in all rare diseases, retrospective design that can induce recall bias and selection bias, potential uncontrolled confounding, absence of perfect match between the SCD group and the patients regarding their number, gender and geographic origin, and the absence of testing the immunoreactivity to suspected exposure), this study supports the hypothesis that mineral environmental risk factors, through occupational exposure to inorganic particles of the patients’ co-residents are linked to paediatric granulomatous disorders with sarcoidosis presentation.
Ethics statements
Patient consent for publication
Acknowledgments
We wish to thank the patients and their families for their participation in the study. We thank the French sarcoidosis group (GSF) (https://splf.fr/groupes-de-travail/sarcoidose-francophone-gsf/le-gsf/), the Société de Pneumologie de langue française (SPLF) and the Silicosis research team (http://www.sciencespo.fr/silicosis/fr). We thank the Assistance Publique-Hôpitaux de Paris and Sorbonne Université Paris, France, and the national networks for rare lung diseases: Centre de référence des maladies respiratoires rares (RespiRare), Centre de référence des maladies pulmonaires rares (OrphaLung) and Filière de soins pour les maladies respiratoires rares (RespiFIL). The RespiRare cohort is developed in collaboration with the Rare Cohort Disease (RaDiCo)-ILD project (ANR-10-COHO-0003), the FP7-305653-child-EU project, the COST Action European network for translational research in children’s and adult interstitial lung disease (COST-ILD) project (CA16125) and the ERS Clinical Research Collaboration for chILD.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
NN and M-EM contributed equally.
Collaborators The French Sarcoidosis Group, The Silicosis Research Group.
Contributors NN and CC designed the study. CC, OM, P-AR and MV designed the questionnaires. M-EM, CC, NN, MB, LS and FJ analysed and interpreted the data. M-EM, NN, P-AR, DV and CC wrote the manuscript.
NN, M-EM, SC, FJ, LS, RA-T, JB, CC-A, FC-A, MC, ChD, CeD, ADe, ADo, RE, JH, VH, DI-B, KJ, SL-J, FL, UM, MM, HN, SM, J-MN, M-HO, AC, DV provided the patients’ clinical data and facilitated the contacts to make the interviews with patients and SCD controls. All authors reviewed and approved the manuscript.
Funding Contract grant sponsor: European Research Council (ERC) / SILICOSIS project / Principal investigator: Paul-André Rosental; Contract grant number: ERC-2011-ADG_20110406ˆProject ID: 295817. Statistical analysis: RespiFIL funds.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.