Article Text

Abstract
Background The COPD Best Practice Tariff (BPT) is a pay-for-performance scheme in England that incentivises review by a respiratory specialist within 24 hours of admission and completion of a list of key care components prior to discharge, known as a discharge bundle, for patients admitted with acute exacerbation of COPD (AECOPD). We investigated whether the two components of the COPD BPT were associated with lower 30-day mortality and readmission in people discharged following AECOPD.
Methods Longitudinal study of national audit data containing details of AECOPD admissions in England and Wales between 01 February 2017 and 13 September 2017. Data were linked with national admissions and mortality data. Mixed-effects logistic regression, using a random intercept for hospital to adjust for clustering of patients, was used to determine the relationship between the COPD BPT criteria (combined and separately) and 30-day mortality and readmission. Models were adjusted for age, sex, socioeconomic status, length of stay, smoking status, Charlson comorbidity index, mental illness and requirement for oxygen or noninvasive ventilation during admission.
Results 28 345 patients discharged from hospital following AECOPD were included. 37% of admissions conformed to the two COPD BPT criteria. No relationship was observed between BPT conforming admissions and 30-day mortality (OR: 1.09 (95% CI 0.92 to 1.29)) or readmissions (OR: 0.96 (95% CI 0.90 to 1.02)). No relationship was observed between either of the individual COPD BPT components and 30-day mortality or readmissions. However, a specialist review at any time during admission was associated with lower inpatient mortality (OR: 0.69 (95% CI 0.58 to 0.81)).
Conclusion Completion of the combined COPD BPT criteria does not appear associated with a reduction in 30-day mortality or readmission. However, specialist review was associated with reduced inpatient mortality. While it is difficult to argue that discharge bundles do not improve care, this analysis questions whether the pay-for-performance model improves mortality or readmissions.
- COPD exacerbations
Data availability statement
Data may be obtained from a third party and are not publicly available. Data collected on behalf of HQIP by all NCAPOP projects are routinely reported and these reports are available in the ‘Resources’ section of the HQIP website (https://www.hqip.org.uk/resources/). The reported data are also placed on the data.gov.uk website. Data are also placed upon MyNHS and NHS Choices. For details of how to apply for data that is not in the public domain, please see HQIP’s data access webpages (https://www.hqip.org.uk/national-programmes/accessing-ncapop-data/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Is the combination of specialist review within 24 hours and discharge care bundle incentivised by the English COPD Best Practice Tariff (BPT) pay-for-performance scheme associated with improved mortality and readmission in acute exacerbation of COPD (AECOPD) admissions?
What is the bottom line?
The combination of specialist review within 24 hours and a discharge care bundle as incentivised by the English COPD BPT pay-for-performance scheme did not appear associated with 30-day mortality or readmission in AECOPD admissions; however, respiratory specialist review was associated with decreased inpatient mortality.
Why read on?
This is the first study to use a large national audit to investigate the impact of the combination of specialist review and discharge care bundles as incentivised by the English COPD BPT pay-for-performance scheme on readmission and mortality in AECOPD admissions.
Background
COPD is the third leading cause of death worldwide1 and an estimated 1.2 million people in the UK have a diagnosis of COPD.2 Many patients with COPD experience episodes of worsening in their symptoms termed an acute exacerbation of COPD (AECOPD), which in the most severe cases require hospitalisation. COPD exacerbations account for approximately 3% of US hospital admissions per year,3 and in England, there are over 100 000 hospital admissions annually due to AECOPD,4 each one costing the National Health Service an average of £1868.5
Pay-for-performance incentives exist in several countries and for several diseases.6–8 In England, optimal care of AECOPD admissions has been incentivised since 2017 through the COPD Best Practice Tariff (BPT), which encourages best practice by paying care providers an additional amount for AECOPD admissions that are (1) reviewed by a respiratory specialist within 24 hours of the admission and (2) receive a discharge care bundle before the patient leaves hospital. A care bundle is a collection of evidence-based interventions.9 For example, the British Thoracic Society (BTS) COPD Discharge Care Bundle comprises: (1) review medication and check inhaler technique, (2) provide a self-management plan and emergency drug pack where appropriate, (3) offer support to achieve smoking cessation, (4) assess and refer for pulmonary rehabilitation and (5) arrange follow-up.10 The aim of the BTS COPD discharge bundle is to improve patient self-management and postdischarge care in order to reduce COPD readmissions.
Achievement of the COPD BPT is assessed at the hospital level, based on admissions recorded in the UK National Asthma and COPD Audit Programme (NACAP), such that if 60% of audited patients with a primary diagnosis of AECOPD receive the two components of the COPD BPT (specialist review and discharge bundle), the hospital will receive an additional payment for all AECOPD admissions managed. If the 60% target is not met, the hospital will not receive the additional payment for any of the AECOPD admissions it managed and will instead be reimbursed at the standard rate.11–14 However, approximately 40% of hospitals in England have negotiated an alternative system of reimbursement for admissions meaning that the COPD BPT does not apply to them.
Review by a multidisciplinary respiratory specialist improves the quality of care received by patients15 and may lead to a reduction in mortality and length of hospital stay.14 16 There is also weak evidence that discharge bundles reduce readmissions.17 However, data suggest that discharge bundles are not always effectively implemented.18 Data from the 2014 COPD audit showed that only 57% of AECOPD admissions were reviewed by a respiratory specialist15 and only 69% of providers used discharge bundles.19 The COPD BPT aims to increase receipt of these two items of care for AECOPD admissions.13
There are few studies on the effectiveness of pay-for-performance in secondary care settings and no study to date has investigated whether implementing the two COPD BPT criteria together improves AECOPD admission outcomes. Therefore, in this analysis of national audit data, we aimed to determine whether people admitted with AECOPD who receive both COPD BPT criteria have fewer readmissions and lower mortality than those who do not receive the COPD BPT. Specifically, we want to determine whether the combination of specialist review and discharge bundle that the COPD BPT seeks to incentivise improves individual patient outcomes, rather than whether the 60% target used by the COPD BPT improves patient outcomes at the hospital level. Therefore, we examine outcomes at the patient level in all hospitals rather than comparing outcomes between eligible hospitals that met the 60% target versus those that did not. If we were instead to compare trusts that met and did not meet the 60% target in an ecological-type analysis, there would be admissions that both did and did not meet the BPT criteria in both the ≥60% and<60% groups. This would make it harder to determine whether the BPT criteria were truly having an impact on patient outcomes.
Methods
Database/population
The NACAP reports care received by patients admitted to hospitals in England and Wales with AECOPD. From 2017, audit data collection has been continual. All acute hospitals in England and Wales were eligible to participate (Scotland joined in 2018), and of 197 eligible hospitals, 182 (92%) participated in data collection. The first report on these prospective data was published in 2018 including analysis for patients admitted from 01 February 2017 and discharged by 13 September 2017. Further details of the audit methodology and results can be found in the published report20 and a paper describing the longitudinal evolution of national COPD audit in the UK.21
In 2019, a follow-up with longer term outcomes—30-day and 90-day mortality and readmission—of the admissions included in the original 2017 audit report was published. All included patients had details of their admission linked with mortality data from the UK Office for National Statistics (ONS)22 and admissions data from England’s Hospital Episode Statistics (HES) Admitted Patient Care (APC) database23 or Wales’ Patient Episode Database for Wales (PEDW).24 After data cleaning to remove patients aged <35 years and admissions with an impossible chronology, the data set was limited to the first admission for each patient in the audit period. This left a data set of 30 294 patients. This data set was used to conduct our analysis; further details are found in the audit outcomes report.25
Variables
The primary exposure in this study was conforming to the COPD BPT. An admission was considered to have conformed to the BPT if a patient received a respiratory specialist review ≤24 hours after admission and a COPD discharge bundle before discharge. The nature of discharge bundle was left to individual hospitals. Admissions where the patient was not reviewed by a respiratory specialist were included in the same category as admissions that received a respiratory specialist review >24 hours after admission. The two components of the COPD BPT (specialist review within 24 hours and discharge bundle) were also examined separately in secondary analyses.
Patients who died during their admission or self-discharged were excluded from analyses as these patients are unlikely to have been able to receive a discharge bundle and it would be unfair to include these admissions in our assessment of conformation to the COPD BPT.
The outcomes examined in this study were 30-day mortality and readmissions. The patient was considered to have died within 30 days of admission if there was an ONS death record <30 days after their admission date (as inpatient deaths were excluded this means that our definition of 30-day mortality represents a variable period after discharge dependent on the length of stay). The data received by us only contained 30-day mortality in a binary format (yes/no patient died within 30 days of admission); therefore, we are unable to calculate 30-day postdischarge mortality. The patient was considered to have been readmitted within 30 days of discharge if there was a HES APC or PEDW admission record for any emergency hospital admission <30 days after discharge.
Potential confounders used in the analysis were age, sex, socioeconomic status, oxygen needed during admission, noninvasive ventilation (NIV) administered during admission, length of stay, smoking status, Charlson comorbidity index and a history of mental illness. Respiratory specialist review was included as an additional confounder in analyses of the COPD discharge bundle as we hypothesised that individuals who had received a specialist review were more likely to receive a discharge bundle. Detailed definitions of confounders are found in online supplemental methods and online supplemental tables S1 and S2.
Supplemental material
Statistical analysis
Data management and statistical analyses were performed using Stata V.15 (StataCorp, College Station, Texas). Data were first summarised using means and proportions where appropriate. In our primary analysis to investigate association between an admission conforming to the COPD BPT (receiving specialist review within 24 hours and receiving a discharge bundle) and 30-day mortality (from admission) and 30-day readmission (from discharge), we used mixed-effects logistic regression (xtlogit command, ‘re’ option) with a random intercept for hospital to account for clustering of patients within hospitals. ORs and 95% CIs were generated for each outcome. After univariate analysis, regression models were adjusted by including the potential confounders described above as covariates in the model.
Secondary analyses were performed using specialist review within 24 hours and receipt of a discharge bundle as the independent variables in place of conformation to the BPT to test the individual components of the BPT. Additionally, we further tested the components of the specialist review variable: patients who either did or did not have a specialist review, and for patients who did have a review, those who had one in ≤24 hours and those who had one in >24 hours.
Missing data were minimal for variables included in regression models and where data were missing, complete case analysis was used. OR graphs were generated using coefplot.26
Sensitivity analyses
We repeated the discharge bundle analysis excluding ‘not clear’ responses to the ‘Has a BTS, or equivalent, discharge bundle been completed for this admission?’ question to determine if there was a strengthening of the effect of a discharge bundle on the outcomes if it was known for certain whether a patient received a bundle or not. We repeated the specialist review analyses using the full audit cohort (including patients who died as an inpatient or self-discharged) to determine whether specialist review was associated with mortality in the full 30-day period from admission or inpatient mortality. Additionally, we repeated the analysis using 90-day mortality and 90-day readmissions as the outcomes to examine if the benefits of the COPD BPT were not detectable until sufficient time had passed for all elements of the discharge bundle to be completed (such as smoking cessation and pulmonary rehabilitation). We also ran the analysis without Welsh hospitals, as these are not eligible to participate in the BPT, to see if there was any change in outcomes. Finally, we examined if there was any difference in patient outcomes between hospitals that met the 60% target for BPT conforming admissions and hospitals that did not meet the target.
Results
After exclusion of patients who self-discharged (n=465 (0.5%)) died during admission (n=1213 (4.0%)) and had ‘other’ as the response for whether they received a discharge bundle (n=571 (1.9%)), the final analysed cohort in this study comprised 28 345 patients (first admission in audit period only) from 181 hospitals.
COPD BPT conforming admissions
Thirty-seven per cent of admissions conformed to the BPT (received specialist review within 24 hours and a discharge bundle) (table 1). BPT conforming admissions, compared with admissions not meeting BPT, were more frequently prescribed oxygen (60.9% vs 51.3%), had more NIV administered (11.4% vs 7.6%), had fewer hospital stays of 0–1 days (24.5% vs 27.4%), more patients with smoking status recorded (95.6% vs 87.7%), more patients with a Dyspnoea, Eosinopenia, Consolidation, Acidaemia and atrial Fibrillation (DECAF) score (measure of AECOPD severity27) recorded (26.5% vs 6.4%) and more patients with spirometry results available (46.0% vs 32.9%).
Demographics and outcomes for people discharged from hospital following acute exacerbation of COPD whose admissions did conform to the COPD Best Practice Tariff (BPT) (receipt of a respiratory specialist review within 24 hours of admission and a discharge bundle) and those whose admissions did not conform to the COPD BPT, N=28 345
In mixed-effects logistic regression analysis, no significant difference in 30-day mortality (OR: 1.09 (95% CI 0.92 to 1.29)) and 30-day readmission (OR: 0.96 (95% CI 0.90 to 1.02)) was found between admissions that conformed to the BPT and admissions that did not conform (figure 1 and online supplemental table S3).

Forest plot of adjusted ORs and 95% CIs for 30-day post-admission mortality and 30-day post-discharge readmission for people discharged from hospital following acute exacerbation of COPD whose admissions conformed to the COPD Best Practice Tariff (BPT) relative to those whose admissions did not conform to the COPD BPT. Values <1 favour conforming to the BPT; values >1 favour not conforming to the BPT.
The COPD BPT individual components
Respiratory specialist review
Fifty-three per cent of admissions were reviewed by a respiratory specialist within 24 hours (online supplemental table S4). Twenty-four per cent of patients did not receive a respiratory specialist review at all (online supplemental table S5). Of the 76% of patients who did receive a review, 69% were within 24 hours of admission, meaning that 31% of reviewed patients had to wait more than 24 hours for a review (online supplemental table S6). A detailed description of the differences between the exposure groups for each of the respiratory specialist review exposures is found in online supplemental results.
In mixed-effects logistic regression analysis, no significant difference in 30-day mortality or 30-day readmission was observed between admissions that were reviewed by a respiratory specialist within 24 hours and those that were not reviewed or reviewed in >24 hours (figure 2A and online supplemental table S7). No significant difference in 30-day mortality or 30-day readmission was observed between patients who did and patients who did not receive a specialist review (figure 2B and online supplemental table S8) and no significant difference was found in either outcome between patients who received a review within 24 hours and those who received a review in >24 hours (figure 2C and online supplemental table S9).
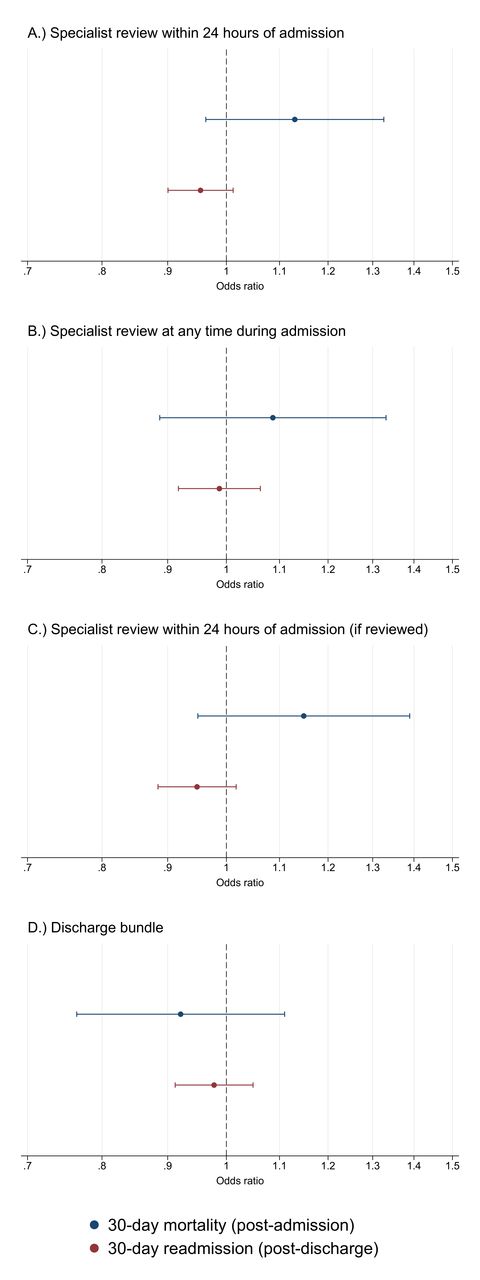
Forest plot of adjusted ORs and 95% CIs for 30-day post-admission mortality and 30-day post-discharge readmission for people discharged from hospital following acute exacerbation of COPD who: (A) received a respiratory specialist review within 24 hours of admission relative to those who did not receive a review or received a review in >24 hours of admission; (B) received a respiratory specialist review at any time during admission relative to those who did not receive a respiratory specialist review at any point during admission; (C) received a respiratory specialist review in ≤24 hours of admission relative to those who received a respiratory specialist review in >24 hours of admission; (D) received a discharge bundle relative to those who did not receive a discharge bundle. Values <1 favour the intervention; values >1 favour not receiving the intervention.
COPD discharge care bundle
Fifty-four per cent of admissions received a discharge bundle (online supplemental table S10). A detailed description of the differences between admissions that did and did not receive a discharge bundle is found in online supplemental results. In mixed-effects logistic regression analysis, no significant difference in 30-day mortality or 30-day readmission was observed between admissions that received a discharge bundle and those that did not receive a discharge bundle (figure 2D and online supplemental table S11).
Sensitivity analysis
Repeating the discharge bundle analysis without ‘not clear’ responses made no material difference to the odds of 30-day mortality and readmission (data available on request).
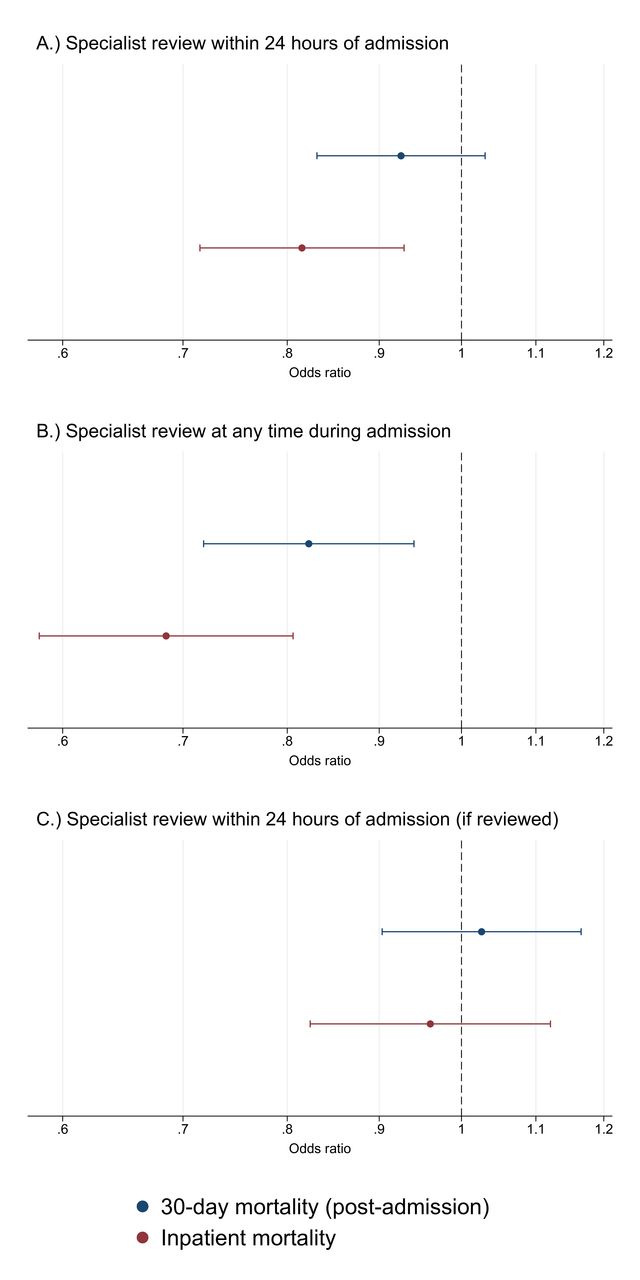
Repeating the specialist review analyses including patients who died during their admission (summary statistics by each specialist review exposure definition are shown in online supplemental tables S12-S14) and therefore, examining mortality in the full 30-day period following admission, did result in changes to the odds of 30-day mortality. However, the only statistically significant result was found for patients who received a specialist review at any time, who had 18% lower odds (OR: 0.82 (95% CI 0.72 to 0.94)) of 30-day death than patients who did not receive a specialist review (figure 3 and online supplemental table S15). Limiting mortality to inpatient mortality only, the effect of specialist review was even stronger with patients who received a specialist review at any time during admission having 31% lower odds (OR: 0.69 (95% CI 0.58 to 0.81)) of inpatient death (figure 3 and online supplemental table S15).

{kind=link}
{kind=link}
{kind=link}
Forest plot of adjusted ORs and 95% CIs for 30-day post-admission mortality and inpatient mortality for patients admitted to hospital with acute exacerbation of COPD (ie, the full audit cohort including patients who died as an inpatient or self-discharged) who: (A) received a respiratory specialist review within 24 hours of admission relative to those who did not receive a review or received a review in >24 hours of admission; (B) received a respiratory specialist review at any time during admission relative to those who did not receive a respiratory specialist review at any point during admission; (C) received a respiratory specialist review in ≤24 hours of admission relative to those who received a respiratory specialist review in >24 hours of admission. Values <1 favour the intervention; values >1 favour not receiving the intervention.
When using 90-day mortality and 90-day readmission as study outcomes, review within 24 hours of admission was significantly associated with 90-day mortality, with patients reviewed within 24 hours having 16% greater odds of dying within 90 days (OR: 1.16 (95% CI 1.05 to 1.28)) (online supplemental table S7). Patients who were reviewed by a respiratory specialist also had 20% higher odds (OR: 1.20 (95% CI 1.06 to 1.36)) of dying within 90 days than patients who were not reviewed by a respiratory specialist (online supplemental table S8), and patients who were reviewed within 24 hours had 13% higher odds (OR: 1.13 (95% CI 1.01 to 1.26)) of dying within 90 days than patients who were reviewed in >24 hours (online supplemental table S9). There was no material difference in mortality or readmissions at 90 days compared with 30 days for patients who received a discharge bundle (online supplemental table S11).
In the analysis using only English hospitals, there was no material difference in 30-day outcome results; however, there were some changes in significance for 90-day outcome results. Patients had 12% lower odds (OR: 0.88 (95% CI 0.79 to 0.98)) of death within 90 days if they received a discharge bundle and patients who received a specialist review within 24 hours (relative to those who received a review in >24 hours) were no longer significantly likely (OR: 1.11 (95% CI 0.99 to 1.24)) to die within 90 days of admission (online supplemental table S16).
In the analysis comparing hospitals where ≥60% of admissions conformed to the COPD BPT and hospitals where <60% of admissions conformed, we did not find a significant difference in outcomes between the two groups (online supplemental table S17).
Discussion
In this study, we did not find an association between the combination of the two criteria (specialist review within 24 hours and receipt of a discharge bundle) of the English COPD BPT pay-for-performance scheme and a reduction in 30-day (postadmission) mortality or 30-day (postdischarge) readmissions among people discharged from hospital following AECOPD. While the BPT was not designed to reduce mortality or readmission rates specifically, rather the intention was to promote better quality patient care, it might be anticipated that better patient care should in turn lead to better outcomes of readmission and mortality. In further analysis, when individually examining the two COPD BPT components, we also did not find an association between being reviewed by a respiratory specialist within 24 hours or receiving a discharge bundle and 30-day mortality or readmissions. However, when we included patients who died as an inpatient, we found that having a specialist review at any time during the admission was associated with 18% lower odds of 30-day mortality and 31% lower odds of inpatient mortality. This suggests that specialist review at any point during an admission is beneficial for inpatient mortality but does not improve mortality after discharge. When repeating the analysis using 90-day outcomes, patients who were reviewed by a specialist within 24 hours of admission had greater odds of dying within 90 days than those who were not reviewed or were reviewed after 24 hours. The most likely explanation for this is that there is important confounding from admission severity that we have not been able to adjust for and that, appropriately, the sicker patients are being reviewed in priority to those who are less unwell. In fact, given that patients seen by a respiratory specialist were more frequently prescribed oxygen and required NIV, respiratory specialist review may simply be a proxy for admission severity.
While it is difficult to argue that discharge bundles do not increase best-practice care, this analysis raises concern that while the right boxes are being ticked in the audit, there is not always effective intervention. We can measure conformance to the BPT, but we cannot measure the quality of the delivery of its components. For example, the bundle component of inhaler technique check will not provide any benefit if the inhaler is used poorly by the patient and optimal use is not then demonstrated and confirmed by the medical team, with a switch to an alternative device as appropriate. It is possible that some hospitals or members of the multiprofessional team may consider a bundle complete if just a few of the items have been completed, while others may complete all bundle items without realising and state that a bundle has not been completed. For example, results from the most recent COPD audit28 show that 74% of admissions were described as having received a discharge bundle, yet the patient was assessed for suitability for pulmonary rehabilitation in only 56% of admissions. We performed a sensitivity analysis, limiting our analysis to just English hospitals to exclude hospitals ineligible to participate in the BPT in case recording of data was better in those participating in the BPT. However, other than a possible suggestion that a discharge bundle was beneficial for 90-day mortality, no material difference was found. One possible reason for not seeing a benefit from the COPD BPT could be that benefits from some of the bundle items, such as smoking cessation and pulmonary rehabilitation, are not seen until after a longer period than 30 days, or the benefits are manifest in other ways (such as improved quality of life) that are not captured by readmission or mortality outcomes. It may also be possible that there is an indirect beneficial effect of the COPD BPT in the form of increased financial investment in respiratory teams as part of the focus to meet the BPT requirements. This may have helped to improve quality of care in COPD admissions. These are important aspects that this analysis cannot address and deserve further study.
While there have not been any previous studies of the COPD BPT pay-for-performance scheme, studies of the COPD BPT components have been completed. A systematic review17 of COPD discharge bundles found that they did not significantly improve mortality or quality of life and only weak evidence for a reduction in readmissions. A more recent literature review29 concluded that it was inconclusive if COPD admission or discharge care bundles reduced readmissions, and that further study was required. A recent UK study18 found no evidence that COPD care bundles reduced 28-day readmission, although emergency department attendances did reduce after care bundles were implemented in hospitals. It was also found that not all items of the admission and discharge bundles were reliably completed. A recent French study30 also concluded that a COPD discharge care bundle had no impact on 28-day AECOPD readmission or mortality. However, one recent US study31 found that all-cause readmissions reduced after implementing a COPD care bundle. It is worth noting that all these bundle studies have comparatively small numbers of included patients and generally compare outcomes at a population-level rather than the patient-level as we have done in this study. No formal assessment of publication bias was conducted in the literature reviews17 29 due to the limited number of published randomised controlled trials and it is possible there is resultant publication bias.
Timely receipt of respiratory specialist input in AECOPD admissions has not been as extensively studied as COPD discharge bundles; however, a study in North East England32 found that after implementing a model that ensured respiratory specialists were available 24 hours a day, 7 days a week, 30-day mortality decreased. An increase in 90-day (but not 30-day) readmissions was also observed. Again, this study compared population-level figures at two time points, which could explain differences from our study.
Although there are no prior studies of the COPD BPT, studies have examined the impact of the hip fracture BPT on patient outcomes. The hip fracture BPT is another pay-for-performance scheme in England, similar to the COPD BPT, that aims to improve care quality for hip fractures. Oakley et al 33 compared admissions before and after the introduction of the hip fracture BPT, BPT compliant and BPT noncompliant admissions. They found that the hip fracture BPT did not lead to any improvements at the organisational level (pre-BPT vs post-BPT), however, at the patient-level, mortality was significantly reduced (BPT vs non-BPT admissions). Survival analysis also found a significant long-term survival benefit for BPT conforming admissions. Whitaker et al 34 similarly found that 1-year survival was significantly better in BPT conforming admissions. Metcalfe et al 35 compared admissions in England and Scotland following the introduction of the BPT (which only applies to England) and found that there was a greater reduction in mortality, readmissions and length of hospital stay during the BPT period in England than in Scotland. It should be noted that the hip fracture BPT has the definitive intervention of surgery that is not present in the COPD BPT, so the two may not necessarily be comparable.
The value of pay-for-performance schemes has been investigated in other healthcare settings;6–8 however, it is difficult to draw direct comparisons given differences in healthcare delivery and pay-for-performance models that exist. While financial incentives are often seen as being a key element in changing clinical practice, pay-for-performance does not always lead to better easily measurable outcomes. For example, financial incentives may lead to better overall investment, with effective implementation of components of pay-for-performance schemes themselves difficult to measure.
The primary strength of this analysis comes from the number of patients included. However, this study does have limitations. We have used adjustment to attempt to control for differences between BPT admissions and non-BPT admissions. However, our results suggest that there is unmeasured confounding from admission severity. It may also be that there is confounding from other factors related to the admission such as COPD disease severity, exacerbation frequency and patient frailty. These are all possible confounders that we unfortunately do not have available data on to be able to adjust for and could possibly explain why we have not been able to find an association between the COPD BPT and mortality or readmission. Another possible limitation is that we have used all-cause readmissions as our outcome rather than just AECOPD admissions. It is not clear whether the BPT or discharge bundle aims to reduce just AECOPD readmissions or any readmissions. However, over 50% of the readmissions in our study were for either AECOPD or pneumonia and some of the other studies discussed used all-cause readmission as an outcome too.18 31 A limitation of the data set that we used is that it is not clear which specific elements of the discharge bundle have been completed, we are simply provided with a binary ‘yes, bundle completed’ response and as Morton et al 18 noted, certain elements of the discharge bundle are not always well completed.
In conclusion, we found that documentation of conforming to the COPD BPT pay-for-performance scheme criteria or receipt of a discharge care bundle alone does not appear to be associated with a reduction in mortality or readmission. However, receiving a respiratory specialist review at any point during an admission was associated with lower inpatient mortality. Further thought and work is needed to better understand the benefits of pay-for-performance models. The COPD BPT and other financial incentive schemes should be specific in the outcomes they want to improve, so that interventions with the strongest evidence base can be financially incentivised. If the COPD BPT is failing to have the desired improvement to patient outcomes because of failure to adequately complete all COPD discharge bundle components, it may be sensible to add each bundle item to the COPD BPT separately rather than including them under the single requirement of ‘COPD discharge bundle’.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data collected on behalf of HQIP by all NCAPOP projects are routinely reported and these reports are available in the ‘Resources’ section of the HQIP website (https://www.hqip.org.uk/resources/). The reported data are also placed on the data.gov.uk website. Data are also placed upon MyNHS and NHS Choices. For details of how to apply for data that is not in the public domain, please see HQIP’s data access webpages (https://www.hqip.org.uk/national-programmes/accessing-ncapop-data/).
Ethics statements
Patient consent for publication
Ethics approval
The audit operates under Section 251 approval from the Confidentiality Advisory Group of the Health Research Authority. The reference number is CAG-8-06(b)/2013. Further details are in online supplemental methods.
Acknowledgments
Preliminary work from this study has previously been presented at the 2019 European Respiratory Society International Congress (https://doi.org/10.1183/13993003.congress-2019.PA3326).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PWS ran the analyses and produced the first draft of the manuscript. PWS, AA, JRH, CMR, JKQ made substantial contributions to conception and design of the study, acquisition and interpretation of data; took part in revising the article critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PWS reports grants from Royal College of Physicians, during the conduct of the study. AA reports grants from Royal College of Physicians, during the conduct of the study. JRH reports grants, personal fees and non-financial support from pharmaceutical companies that make medicines to treat COPD, outside the submitted work. CMR reports personal fees from Astra Zeneca, personal fees from Pfizer, outside the submitted work. JKQ reports grants from Royal College of Physicians, during the conduct of the study; grants and personal fees from AZ, grants and personal fees from Bayer, grants and personal fees from BI, grants and personal fees from Chiesi, grants and personal fees from GSK, grants from MRC, grants from The Health Foundation, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Airwaves