Article Text

Abstract
Introduction and aim Exposure to some insecticides may cause airway obstruction, but existing evidence is limited by cross-sectional designs and inadequate confounder control. We investigated the relation between organophosphate and carbamate insecticides and pulmonary function in a prospective study accounting for important confounders.
Methods In a cohort of 364 smallholder farmers in Uganda (69% women), participants underwent pre-bronchodilator spirometry at baseline (September/October 2018) and at two follow-up visits (November/December 2018 and January/February 2019). Exposure to carbamate and organophosphate insecticides was assessed using haemoglobin-adjusted erythrocyte acetylcholinesterase (AChE/Hb). Less than 3% of participants were lost to follow-up. We calculated Z-scores for FEV1, FVC and FEV1/FVC using the Global Lung Function Initiative equations. Data were analysed in linear mixed and fixed effect models accounting for family relationships and repeated measures of exposure and outcome.
Results Low AChE/Hb was significantly associated with low FEV1 Z-score in both unadjusted and adjusted analyses. Compared with individuals with AChE/Hb 25.90 U/g (50th percentile, reference), those with lower AChE/Hb 24.50 U/g (35th percentile) had mean FEV1 Z-score 0.045 (0.003 to 0.087) lower, and persons with higher AChE/Hb 27.30 U/g (65th percentile) had a mean FEV1 Z-score 0.043 (−0.002 to 0.087) higher compared with the reference. Similar, but numerically smaller and statistically non-significant effects were seen for Z-scores of FVC and FEV1/FVC.
Conclusion Exposure to organophosphate and carbamate insecticides may lead to lung function decline. Our results add to the growing evidence of health effects in relation to exposure to organophosphate and carbamate insecticides, underlining the importance of minimising exposure.
- occupational lung disease
- asthma epidemiology
- COPD epidemiology
Data availability statement
Data are available upon reasonable request. Please contact the corresponding author for access to de-identified data from the subset of participants that consented to data sharing. Access requires approval from the MakSPH-HDREC and the Danish Data Protection Agency.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
Is exposure to cholinesterase-inhibiting insecticides associated with pulmonary function impairment?
What is the bottom line?
Low erythrocyte acetylcholinesterase was associated with low FEV1 among farmers, suggesting that subchronic exposure to cholinesterase inhibiting insecticides leads to impairment of lung function.
Why read on?
We improve on previous studies by using repeated measurements of both exposure and lung function and adjusting for important confounders, thereby reducing the risk of bias in our analyses.
Introduction
Asthma and chronic obstructive pulmonary disease are major public health challenges, with estimated global prevalence of 273 million and 299 million people, respectively.1 Some risk factors for these diseases are well-known, including tobacco smoking,2 3 genetic susceptibility and air pollution.2 4 It has also been suggested that exposure to some classes of pesticides can lead to lung function impairment, both in the general population5 6 and among occupationally exposed workers.7 Acute poisoning with acetylcholine-inhibiting insecticides (organophosphates and carbamates) can lead to respiratory failure,8 partly due to bronchoconstriction and increased mucus production in the airways.8 Exposure to organophosphates and carbamates at levels too low to cause acute intoxication might lead to airway obstruction. A recent systematic review and meta-analysis on pesticide exposure and lung function indicated that exposure to cholinesterase (ChE) inhibiting pesticides may reduce FEV1/FVC.9 However, the confidence in the findings was limited, as most studies were cross-sectional, had inadequate confounder control and did not investigate exposure–response relationships.9
Smallholder farmers in low- and middle-income countries can be heavily exposed to pesticides due to a lack of training, unsafe pesticide application practices and limited use of personal protective equipment.10–13 If pesticide exposure impairs pulmonary function, such farmers may therefore be some of the most affected persons, though few previous studies have focussed specifically on this group. Hence, the objective of this study was to investigate whether subchronic exposure to organophosphate and carbamate insecticides was associated with impaired lung function among smallholder farmers in Uganda, in a short-term follow-up study with abundant information on possible confounders.
Methods
Study design
The study was conducted as part of the ‘Pesticide Exposure, Asthma and Diabetes in Uganda’ (PEXADU) project,14 a short-term cohort study among members of two organisations of smallholder farmers from the Wakiso District in central Uganda—one for conventional farmers, and one for farmers working towards organic certification. We recruited participants from these two organisations to minimise confounding from sociodemographic variables while maximising insecticide exposure contrast. Participants were examined at baseline in September/October 2018 (phase 1) and at two follow-up visits in November/December 2018 (phase 2) and January/February 2019 (phase 3). The main insecticide application season in the study area is October/November (personal communication, Aggrey Atuhaire, Uganda National Association of Community and Occupational Health), and we selected the timing of the three rounds of examinations to also maximise contrast in insecticide exposure within the participants.
Study population
We attended the weekly meetings among small groups in each farmers’ organisation and invited all members 18 years or older to participate. Pregnant women were excluded. We compiled a list of 532 persons potentially eligible for participation, and used a pseudo-random number generator to randomise the sequence of persons on the list. Potential participants were invited in sequence by telephone. If a person could not be reached by telephone, or was unable to participate, we excluded that person and called the next person on the list. At baseline, 380 out of 532 individuals came to the examination centre, and after exclusion of ineligible persons, we included 364 participants. We re-examined 356 and 354 subjects in phase 2 and phase 3, respectively (see figure 1).
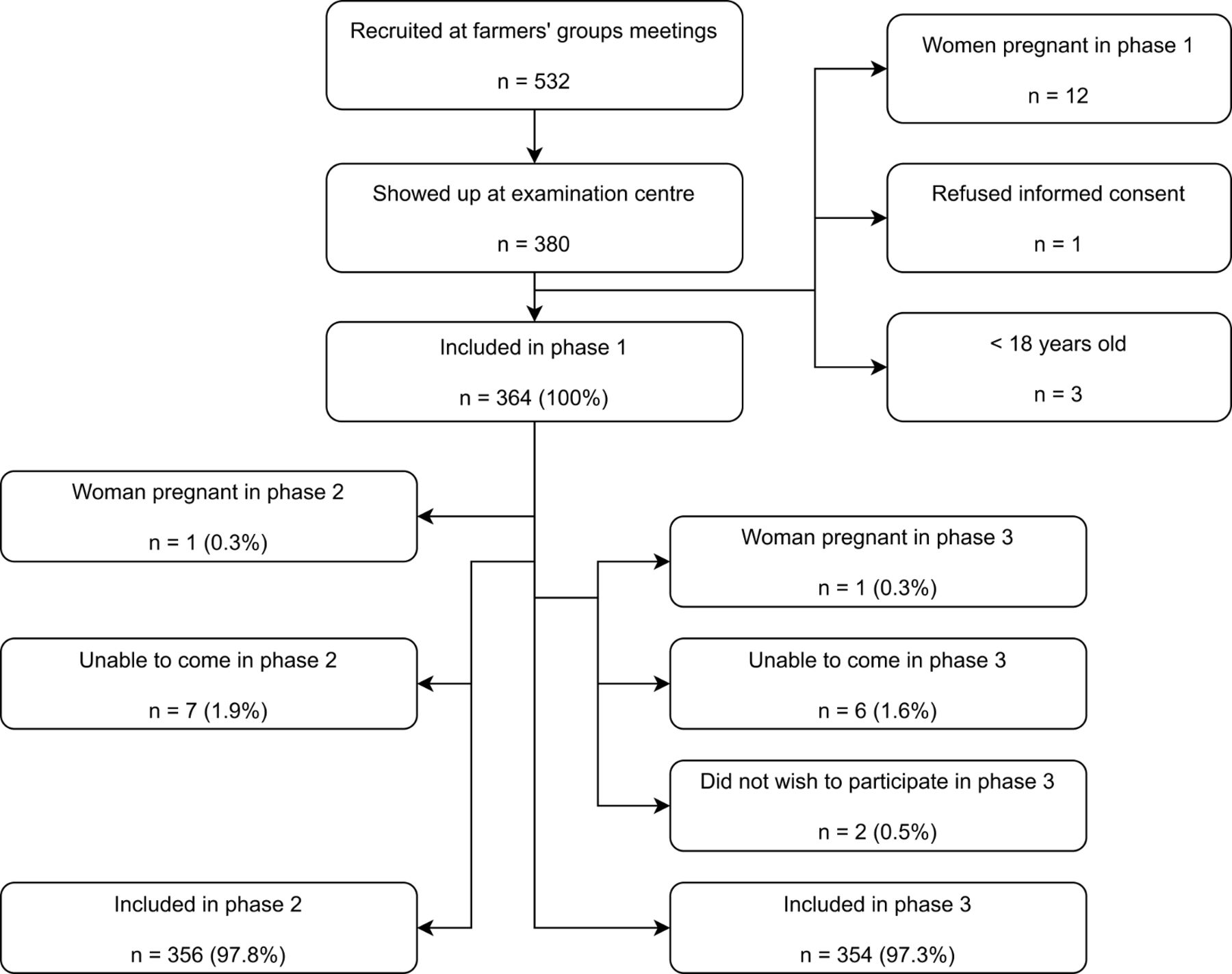
Flowchart of participant recruitment.
Outcome assessment
Pulmonary function was quantified by pre-bronchodilator spirometry using a MicroDL spirometer and Spida 5 PC software (Micro Medical, Rochester, Kent, England). Exclusion criteria were myocardial infarction in the last 3 months, angina pectoris, haemoptysis, any surgery in the last 3 months, aortic aneurysm, history of pulmonary embolism, active tuberculosis, other current respiratory infection and severe hypertension (systolic >200 mm Hg or diastolic >120 mm Hg). If standard American Thoracic Society (ATS) criteria15 for quality of spirometry were not fulfilled after five blows, four additional attempts were provided. After the examination, quality and repeatability of all manoeuvres were assessed by a medical doctor with experience in pulmonary function testing, according to modified ATS criteria (online supplemental appendix 1). Reliable spirometry results were available for 290, 285 and 263 persons in phase 1, phase 2 and phase 3, respectively (see figure 2).
Supplemental material

Flowchart describing numbers of participants who performed spirometry.
The primary outcomes were Z-scores for forced expiratory volume in the first second (FEV1), forced vital capacity (FVC) and FEV1/FVC, calculated using the Global Lung Function Initiative (GLI-2012) equations,16 with ‘African-American’ ethnicity as the reference, while absolute values of FEV1, FVC and FEV1/FVC were secondary outcomes. Peak expiratory flow (PEF), instantaneous forced expiratory flow after exhalation of 25%, 50% and 75% of the FVC (FEF25, FEF50 and FEF75), mean forced expiratory flow between 25% and 75% of the FVC (FEF25-75) and FEF25-75 Z-score were also secondary outcomes.
Exposure assessment
To quantify exposure to organophosphate and carbamate insecticides, we used capillary blood erythrocyte acetylcholinesterase (AChE) analysed using a point-of-care device (Test-mate ChE Cholinesterase Test System Model 400, EQM Research Inc, Cincinnati, Ohio, USA). The analysis was performed immediately after blood sampling, and according to the manufacturer’s instructions.17 The primary toxicodynamic mode of action of organophosphate and carbamate insecticides is inhibition of nervous system acetylcholinesterase.18 The enzyme isoform in erythrocytes (AChE) is readily available for sampling, and can be measured as an expression of exposure in the short to medium term.19 Our primary exposure metric was AChE activity normalised by haemoglobin (Hb) concentration: AChE/Hb (U/g). Results from the Test-Mate system were recorded on paper and later double-entered using the Open Data Kit (ODK) Collect application.20
Confounder selection and assessment
Confounders were defined a priori using Directed Acyclic Graphs21 and the DAGitty software.22 The basic set of confounders included age, sex, cumulated lifetime tobacco smoking and cumulated lifetime hours of cooking as a proxy for exposure to biofuel smoke. The extended set of confounders also included body mass index and years of full-time education as a proxy for socioeconomic status. For analyses of absolute spirometric indices, all analyses included sex, age and height as covariates. Tobacco smoking was quantified as pack-years. Biofuel smoke exposure was expressed as ‘cooking years’, defined as the number of years with an average of 2.5 hours of cooking per day. We did not adjust analyses for the specific spirometer used during testing, as calibration check data showed that differences between spirometers were minor and did not explain the observed temporal trends in spirometric results.23
Height and weight was measured in a standardised manner24 using a stadiometer (SM-SZ-300, Sumbow Medical Instruments Co Ltd, Ningbo, China) and medical scale (seca robusta 813, seca GmbH & Co, Hamburg, Germany), respectively. Anthropometric data was recorded directly in ODK Collect.20
Subjective covariate information was collected in a structured, questionnaire-based interview. Questions on demographic data and tobacco smoking derived from the WHO STEPs questionnaire,25 while questions on exposure to biomass fuel smoke were adapted from the World Health Survey26 questionnaire. Finally, questions related to pesticide exposure were adapted from an existing questionnaire designed for use among smallholder farmers in low- and middle-income countries.13 27 We modified the existing pesticide questionnaire to make it simpler and faster to administer, while still collecting relatively detailed exposure information on, for example, duration and intensity of pesticide usage, and which specific pesticides were used. The interview was conducted in English or Luganda; the Luganda version of the questionnaire was back-translated to English before use. Interviewers entered answers directly into a database using ODK Collect.20
Statistical analyses
Data were managed using Python 3 (Python Software Foundation, https://www.python.org/) and Stata 15 (StataCorp, College Station, Texas, USA), and analysed using Stata 15. The analysis plan was specified a priori and published online.21 For an overview of all analyses performed (including sensitivity analyses), and any deviations from the protocol, see online supplemental appendix 2.
Supplemental material
All outcome variables were analysed on a continuous scale. To account for family relationships and repeated measurements of both exposure, outcome and covariates, data were analysed in a linear mixed effect model with random effects for family and participant, and fixed effects for the exposure and confounder variables. The regression coefficient for the exposure variable was allowed to vary between participants. A ‘family’ was defined as a group of participants where all members were genetically related to at least one other member of the group. The model can be described thus:

y is the outcome.  is the regression coefficient for the effect of the exposure variable b on the outcome;
is the regression coefficient for the effect of the exposure variable b on the outcome;  is normally distributed in the study population, and each person has his/her own level of
is normally distributed in the study population, and each person has his/her own level of  . The regression coefficient for the effect of the i
th confounder ci is called
. The regression coefficient for the effect of the i
th confounder ci is called  and all members of the population have the same
and all members of the population have the same  . Random effects for family and participant are called α and τ, respectively. ε is an error term.
. Random effects for family and participant are called α and τ, respectively. ε is an error term.
Apart from sex, all independent variables were continuous and were generally modelled using restricted cubic splines with four knots to take into account non-linear exposure–response relationships. However, tobacco smoking was modelled under the assumption of linearity, as the number of smokers was too low to use splines (table 1). We used the xblc28 Stata package to plot results for spline variables.
Demographics for the study population at baseline
Analyses only included participants with information on all covariates from at least one project phase. The number of observations in each model is available in online supplemental appendix 2. Due to a negligible loss to follow-up (see figure 1), we did not account for it statistically.
To remove the effect of unknown time-invariant confounders, we performed secondary fixed effect analyses focussing on the change in variables within each person between project phases. The model can be written as

 is the change in the outcome between two project phases.
is the change in the outcome between two project phases.  is the change in the ith independent variable xi, and
is the change in the ith independent variable xi, and  is the regression coefficient for the fixed effect of Δxi on Δy. All participants have the same
is the regression coefficient for the fixed effect of Δxi on Δy. All participants have the same  . α is a random effect for family, and ε is an error term. In our main fixed effect model, we compared phases 1+3. Sensitivity analyses compared phases 1+2 and 2+3, respectively.
. α is a random effect for family, and ε is an error term. In our main fixed effect model, we compared phases 1+3. Sensitivity analyses compared phases 1+2 and 2+3, respectively.
Results
Demographics of the study population are provided in table 1, both overall and stratified by AChE/Hb below or above the median at baseline. Two-thirds of participants were women, and most were middle-aged (median age 46.6 years). Few were ever-smokers, and the number of pack-years for ever-smokers was low. The vast majority of the participants used biomass fuels for cooking. Individuals above and below the median AChE/Hb were similar in terms of all included demographics, except for sex, where men had higher AChE/Hb than women. Self-reported use of pesticides, including cholinesterase-inhibiting insecticides, was similar in the two strata of AChE/Hb.
The mean pulmonary function (defined primarily by Z-scores of FEV1, FVC and FEV1/FVC) decreased across project phases, and so did AChE/Hb, table 2. The range of observed values showed considerable overlap between phases, and the changes in the means were numerically small, but most were statistically significant. Analyses of variance for both outcome and exposure variables are provided in online supplemental appendix 3. Most of the variance was between persons and between families, with less variation within persons. The ratio of within-person variance to the sum of between-person and between-family variance was 0.12 for FEV1 Z-score, 0.15 for FVC Z-score, 0.43 for FEV1/FVC Z-score and 0.22 for AChE/Hb.
Supplemental material
Lung function measures and acetylcholinesterase in each project phase
In our main analysis, FEV1 Z-score was significantly lower among individuals with low AChE/Hb, compared with persons with higher AChE/Hb, both in unadjusted analyses and adjusted analyses including the basic and extended sets of confounders (figure 3 and table 3). FVC Z-score and FEV1/FVC Z-score showed similar patterns as FEV1 Z-score, but differences were numerically smaller and statistically non-significant.
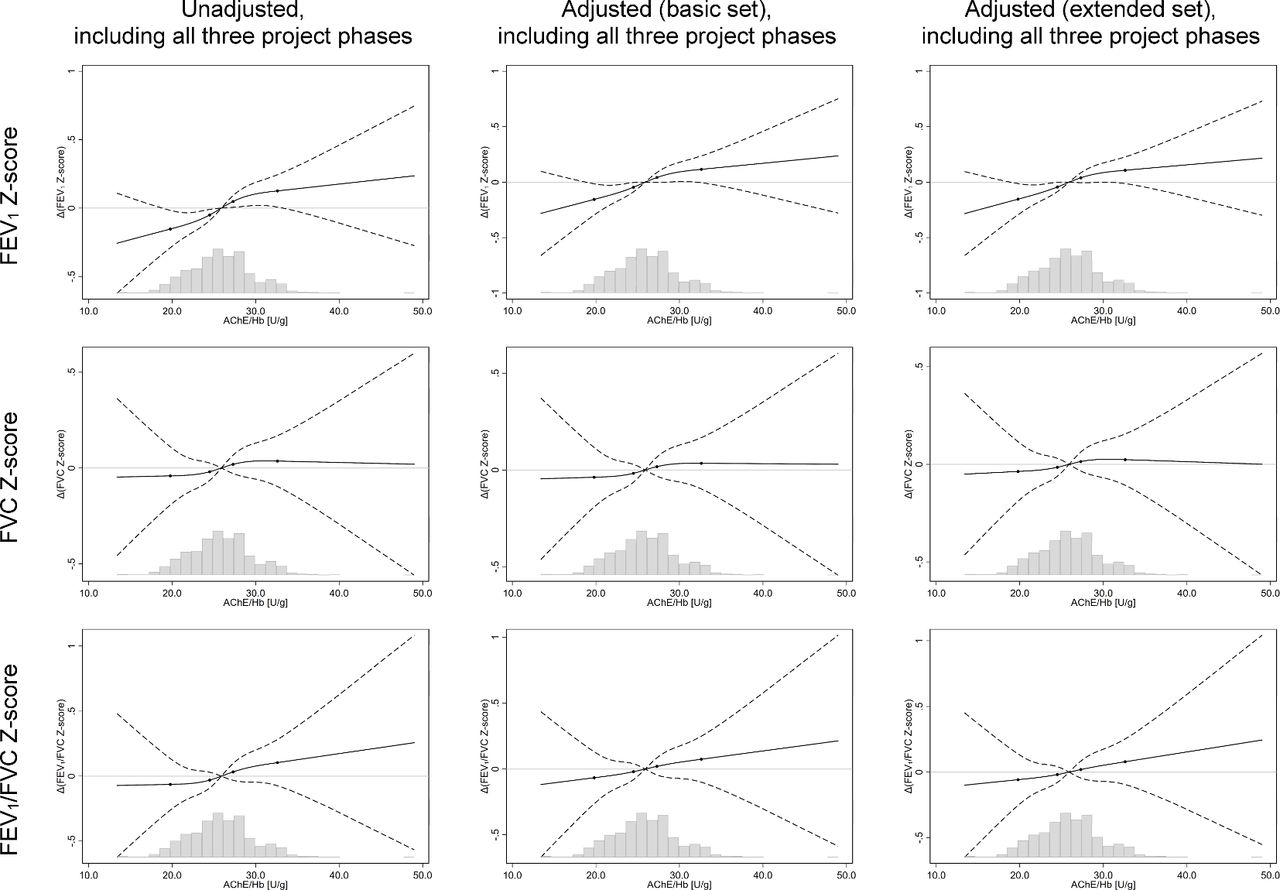
Results from random coefficient model of pulmonary function versus AChE/Hb. Solid line shows lung function parameter relative to value at the median AChE/Hb. Dashed lines show 95% CI. Spline knot location shown by black dots. Histograms show the distribution of AChE/Hb values for observations in the model. Basic covariate set=age, sex, pack-years of smoking, cumulated lifetime hours of cooking. Extended covariate set=basic set+BMI, years of full-time education. AChE/Hb, erythrocyte acetylcholinesterase normalised by haemoglobin concentration.
Summary table of results from random coefficient model
Analyses of absolute lung function measures generally confirmed the results for Z- scores, but were only statistically significant in unadjusted analyses for FEV1 (table 3 and online supplemental appendix 2). Analyses of the remaining secondary outcomes (such as PEF and FEF25) were less consistent (online supplemental appendix 2).
A number of preplanned sensitivity analyses conducted to check the robustness of the main findings generally gave similar results as the main analyses (online supplemental appendix 2). However, in an adjusted post-hoc sensitivity analysis that included project phase as a categorical variable, no clear relationships were seen between AChE/Hb and spirometry Z-scores (see online supplemental appendix 2), probably due to the association between phase and exposure seen in table 2. In post-hoc analyses stratified by sex, associations between AChE/Hb and spirometry Z-scores were only evident for women (online supplemental appendix 2).
In the fixed effect model, we did not demonstrate any clear association between change in AChE/Hb between phase 1 and phase 3, and the change in Z-scores of FEV1 and FVC, figure 4. We did see a statistically non-significant association between decreases in AChE/Hb between phases (corresponding to increased exposure) and decreases in FEV1/FVC Z-score, but this result should be interpreted with caution due to the unclear pattern for Z-scores of FEV1 and FVC. Sensitivity analyses comparing phase 1/2 and phase 2/3 provided inconsistent results, online supplemental appendix 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results from fixed effect model of change in pulmonary function and AChE/Hb from phase 1 to phase 3. Solid line shows lung function parameter relative to value at the median Δ(AChE/Hb). Dashed lines show 95% CI. Spline knot location shown by black dots. Histograms show the distribution of Δ(AChE/Hb) values for observations in the model. Basic covariate set=Δage, Δpack-years, Δ(hours of cooking in the last week). Extended covariate set=basic set+ΔBMI. AChE/Hb,erythrocyte acetylcholinesterase normalised by haemoglobin concentration.
Discussion
In our analyses, low AChE/Hb (indicating high exposure to organophosphate and carbamate insecticides) was associated with low values of most spirometric indices. The relationship was numerically largest and statistically significant for FEV1 Z-score, but similar trends were seen for FVC Z-score and FEV1/FVC Z-score. This indicates that exposure to organophosphate and carbamate insecticides might impair pulmonary function. Our confidence in the findings are somewhat tempered by the lack of clear exposure-response patterns in the fixed effect model, but the latter model may have been statistically underpowered due to a lower-than expected within-person exposure variability.
Exposure to cholinesterase inhibitor insecticides is the most obvious explanation for depression of AChE/Hb in this population of smallholder farmers. However, we did not see any clear differences in self-reported use of insecticides between persons with AChE/Hb below or above the median at baseline (table 2). The farmers might mainly be exposed in ways on which we do not have information, such as re-entry exposure during work in previously sprayed fields, or through diet. Of note, insecticide exposure is not the only factor that can influence AChE/Hb.29 Our results could therefore be confounded, but the problem is likely limited, as demographics between the low and high AChE/Hb groups at baseline were generally similar, and results from unadjusted and adjusted analyses of Z-scores for FEV1, FVC and FEV1/FVC were nearly identical. Because of the lack of association between subjective exposure to cholinesterase inhibitor insecticides and AChE/Hb, we did not adjust our analyses for use of other pesticides (such as pyrethroid insecticides, glyphosate and dithiocarbamate fungicides), for which we currently only have subjective exposure information and no biomarkers. Depressed AChE/Hb could therefore be a proxy for exposure to other agrochemicals.
Our findings support previous mainly cross-sectional studies showing associations between decreased pulmonary function and exposure to cholinesterase-inhibiting insecticides, expressed as either urinary metabolites of organophosphates,5 6 30 or depressed cholinesterase activity.31–35 Most previous studies were conducted among occupationally exposed workers and farmers, the majority of whom were men.30–35 Two studies showed associations in general populations with more balanced gender distributions.5 6 Thus, our study differs somewhat from previous studies, as our study population was occupationally exposed and most participants were women, and caution is warranted before directly comparing numerical estimates from the current and previous studies.
A link between exposure and lung function impairment is biologically plausible, as acute intoxication with cholinesterase inhibitor insecticides leads to bronchoconstriction.8 Support is also provided by a double-blind, randomised, placebo-controlled human trial on the pulmonary effects of the cholinesterase inhibitor medicine pyridostigmine in healthy volunteers. After administration of 60 mg of pyridostigmine, FEV1 decreased on average 130 mL, strongly correlated with the degree of acetylcholinesterase inhibition that ranged from ~20% to ~40%.36 In the present study, median AChE/Hb was 26.3 U/g at baseline. While AChE/Hb has a wide normal range,17 26.3 U/g is only 84% of the reference value (31.4 U/g) stated by the manufacturer of the device that we used to measure AChE/Hb.17 Hence, the degrees of cholinesterase inhibition in our study population and in the previous experimental study are of the same order of magnitude.
The effect sizes demonstrated in the study were modest, but non-negligible. In the analysis of the influence of AChE/Hb on the absolute value of FEV1, there was an estimated difference of 78 (9 to 148) mL in FEV1 between the 5th and 95th percentiles of AChE/Hb, after adjustment for the basic set of confounders. While this is below the Minimal Clinically Important Difference in FEV1 of 100 mL in pharmacological trials,37 it is a relevant difference at population level. In comparison, a systematic review on the pulmonary effects of outdoor air pollution found that each 10 µg/m3 increase in short-term exposure to PM2.5 was associated with a −7.02 (−11.75 to –2.29) mL change in FEV1.38
The strength of this study is the relatively large study population, all recruited from farmers’ organisations, and followed over time to account for both interindividual and intraindividual variability in pesticide exposure. We had low losses to follow-up. Exposure and outcome were objectively determined following established standards, and we accounted for confounders defined a priori based on Directed Acyclic Graphs.21
Our study also has clear limitations. Foremost, our sampling strategy was convenience-based, that is, participants were recruited from farmers’ organisations that we presumed a priori to have different mean exposure levels, but similar demographics. Limited information from each recruitment meeting was available regarding the number and characteristics of farmers who did not wish to participate in our study, and selection bias before baseline is theoretically possible. The proportion of female participants was high (69%), but this does not necessarily reflect imbalanced selection by sex, as the overall proportion of women among individuals economically active in agriculture in Uganda is 50%,39 and 56% of the labour time in Ugandan agriculture is provided by women.40 Loss to follow-up between phases was negligible and unlikely to introduce any considerable bias. However, some selection bias could have been introduced by (un)availability of spirometry data for included participants. We conducted a post-hoc analysis limited to spirometric results from phase 1, as Directed Acyclic Graphs showed that in this phase, the potential for selection bias was lower than in the study overall (see figure 2 and online supplemental appendix 2). The association between low AChE/Hb and low FEV1 Z-score disappeared in this cross-sectional analysis (online supplemental appendix 2). This could indicate that our main analyses are biassed by selection processes, but on the other hand, the cross-sectional analysis did not account for the considerable physiological variation in AChE/Hb.17
Pulmonary function was only assessed by pre-bronchodilator spirometry, as we did not have ethical clearance to administer bronchodilator medicine to participants. Hence, we cannot tell if airway obstruction was reversible.
We could confirm relationships between spirometric results and well-known determinants of pulmonary function, for example, age, sex and height (online supplemental appendix 2), strengthening our confidence in results related to AChE/Hb. Unexpectedly, we found no consistent associations between biomass smoke exposure or tobacco consumption with pulmonary function. The latter is probably due to power issues, as few of the participants had ever smoked, and our metric for biomass smoke was crude, meaning there is likely bias toward the null. Residual confounding due to the crude exposure metric for biomass smoke is likely limited, as biomass exposure is probably determined by a combination of sex, age and socioeconomic status—variables that we have adjusted for.
The median Z-scores for FEV1, FVC and FEF25-75 in the study population were <0 in all phases, while the Z-score for FEV1/FVC was >0. This could be a result of the harmful influence of various exposures on pulmonary function, or because the GLI-2012 equations16 do not include data from Uganda. Due to a lack of normal values for the Ugandan population, we used normal values for African-Americans. We analysed the Z-scores as continuous variables, and adjusted analyses of the raw metrics FEV1, FVC, FEV1/FVC and FEF25-75 gave similar results to the analyses based on the corresponding Z-scores. Therefore, the use of African-Americans as reference population is unlikely to pose a threat to the internal validity of our findings.
A considerable number of statistical analyses were conducted. Nevertheless, we do not think that multiple comparisons pose a substantial problem for the study validity, as we decided a priori which covariates to adjust for, which outcomes were primary and secondary, and which analyses were primary, secondary and sensitivity analyses. Furthermore, we see clear and consistent patterns for each exposure–outcome pair in the random coefficient models. We prepublished the analysis protocol in an online repository,21 and all deviations from protocol are listed in online supplemental appendix 2.
While we believe that our findings are generalisable to smallholder farmers using organophosphate and carbamate insecticides in Eastern Africa, care should be taken before extrapolating the findings to other populations with lower exposure levels, for example, farmers applying pesticides in high-income countries or consumers eating fruits and vegetables with pesticide residues. The PEXADU project population has a relatively high exposure to pesticides due to a lack of training on proper handling of pesticides and poor use of personal protective equipment.14 Further studies are needed to investigate whether similar effects can be demonstrated in lower-exposed populations.
Conclusion
Our main analyses indicate that occupational exposure to organophosphate and carbamate insecticides may lead to lung function impairment, though diverging results from some sensitivity and secondary analyses mean that caution is warranted when interpreting the findings. Nevertheless, our results add to the growing evidence of health effects in relation to exposure to organophosphate and carbamate insecticides, underlining the importance of preventive measures to avoid or minimise exposure.
Data availability statement
Data are available upon reasonable request. Please contact the corresponding author for access to de-identified data from the subset of participants that consented to data sharing. Access requires approval from the MakSPH-HDREC and the Danish Data Protection Agency.
Ethics statements
Ethics approval
The study was carried out in accordance with the Declaration of Helsinki. Participants gave informed consent before inclusion and were financially compensated for lost earnings on examination days. The project was approved by the Higher Degrees Research and Ethics Committee at Makerere University School of Public Health (MakSPH-HDREC, registration number 577) and the Uganda National Council for Science and Technology (registration number HS234ES).
Acknowledgments
We wish to thank the participants, as well as our collaborators from the Uganda National Association of Community and Occupational Health, Caritas Uganda, Wakiso District Farmers Association, the Agency for Integrated Rural Development and the Diálogos Foundation. We are thankful for the efforts of the field team: Amusa Wamawobe, Betty Kateregga, Brenda Wagaba, Evans Twin, Grace Lubega, Jonathan Mugweri, Imelda Namatovu, Joviah Gonza, Lydia Yariwo and Timothy Masaba. Finally, we are grateful to Dr Wajd Abbas Hassan Hansen for her assistance with spirometry quality control.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MRHH: conceptualisation; methodology; formal analysis; investigation; data curation; writing—original draft; project administration; funding acquisition. EJ: conceptualisation; methodology; writing—review and editing; supervision. AS: conceptualisation; methodology; writing—review and editing; supervision. DS: conceptualisation; methodology; resources; writing—review and editing. JCS: conceptualisation; methodology; writing—review and editing. RM: conceptualisation; methodology; writing—review and editing. PS: conceptualisation; methodology; writing—review and editing. SF: conceptualisation; methodology; writing—review and editing. TS: methodology; writing—review and editing. AB: methodology; writing—review and editing. BMB: methodology; writing—review and editing. VS: conceptualisation; methodology; writing—review and editing; supervision; funding acquisition. All authors have reviewed and approved the final manuscript.
Funding This project was supported by grants from Aarhus University Research Foundation (project number 81231) and the National Research Centre for the Working Environment (project number 10322). Neither of the funders played any role in study design, data collection/analysis, drafting of the manuscript or the decision to publish.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.