Article Text

Abstract
Background The association of ACE inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) with disease severity of patients with COVID-19 is still unclear. We conducted a systematic review and meta-analysis to investigate if ACEI/ARB use is associated with the risk of mortality and severe disease in patients with COVID-19.
Methods We searched all available clinical studies that included patients with confirmed COVID-19 who could be classified into an ACEI/ARB group and a non-ACEI/ARB group up until 4 May 2020. A meta-analysis was performed, and primary outcomes were all-cause mortality and severe disease.
Results ACEI/ARB use did not increase the risk of all-cause mortality both in meta-analysis for 11 studies with 12 601 patients reporting ORs (OR=0.52 (95% CI=0.37 to 0.72), moderate certainty of evidence) and in 2 studies with 8577 patients presenting HRs. For 12 848 patients in 13 studies, ACEI/ARB use was not related to an increased risk of severe disease in COVID-19 (OR=0.68 (95% CI=0.44 to 1.07); I2=95%, low certainty of evidence).
Conclusions ACEI/ARB therapy was not associated with increased risk of all-cause mortality or severe manifestations in patients with COVID-19. ACEI/ARB therapy can be continued without concern of drug-related worsening in patients with COVID-19.
- viral infection
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data are available by accessing the published studies listed in table 1.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is the key question?
Is there a statistical significance in clinical outcomes, including all-cause mortality and severe disease between ACE inhibitors/angiotensin II receptor blocker (ACEI/ARB) group and non-ACEI/ARB group in patients with COVID-19?
What is the bottom line?
For 21 178 patients in 13 studies, ACEI/ARB use did not increase the risk of all-cause mortality of patients with COVID-19.
For 12 848 patients in 13 studies, ACEI/ARB use was not related to an increased risk of severe disease in those with COVID-19.
Why read on?
Our study supports the current recommendations favouring the continuation of ACEI/ARB use during the COVID-19 pandemic.
Introduction
As of 9 May 2020, SARS-CoV-2 has infected >3.7 million people and killed >259 000 patients worldwide.1 However, knowledge of this new virus remains sparse, which is a major hindrance to overcoming the current pandemic. One of the main issues to resolve is whether the use of the renin-angiotensin system blockers, including ACE inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs), may be associated with the severity of COVID-19 caused by SARS-CoV-2.
Preclinical studies demonstrated an increase in the expression level of ACE2 in the heart2 and kidney3 of rats treated with ARBs, as well as in human intestine biopsies treated with ACEIs.4 ACE2 was identified as a functional receptor through which SARS-CoV-2 enters host cells.5 6 Therefore, it is reasonable to be concerned that treatment with ACEI/ARB could facilitate virus entry due to increased ACE2 expression, leading to more severe disease. If this is the case, ACEI/ARB should be discontinued in patients who are being treated with these drugs on the confirmation of COVID-19 diagnosis.7 This issue is important, given that the duration of the SARS-CoV-2 pandemic remains unclear,8 and ACEI/ARBs are among the most commonly prescribed drugs.9 10 Although several professional societies have recommended the continuation of ACEI/ARBs in the current situation,11 uncertainty remains owing to a lack of supporting clinical data. Although several observational studies have been published recently,12–21 they reported somewhat different results. For example, Zhang et al showed that ACEI/ARB treatment was associated with a reduced risk of mortality in patients with COVID-19,21 but Mancia et al showed a higher proportion of ACEI/ARB use among critical patients than among those with mild-to-moderate infection.14
To help resolve this issue, we conducted a systematic review and meta-analysis on recently published studies to investigate the effects of ACEI/ARBs on the risk of mortality and severe disease in patients diagnosed with COVID-19.
Methods
Protocol and registration
This systematic review was reported according to the guidelines of the Meta‐analysis of Observational Studies in Epidemiology22 and Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement.23 The protocol of the systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO, CRD42020179780) on 17 April 2020.
Eligibility criteria
The eligibility criteria for studies included in the systematic review were as follows: (1) the study subjects were diagnosed with COVID-19 by high-throughput sequencing or real-time reverse transcription-PCR assay using upper or lower respiratory tract specimens, (2) the subjects could be classified into ACEI/ARB user and non-ACEI/ARB user groups, (3) the severity of disease or all-cause mortality was evaluated according to the use of ACEI/ARB and (4) any human clinical comparative study except for those with a cross-sectional design.
Information sources and search strategy
The Medline, Embase, Cochrane Central Register of Controlled Trials, MedRxiv, Social Science Research Network and Peer J databases were searched for potentially eligible published and unpublished studies up to 4 May 2020. The search strategy was designed by experienced researchers (HWL and C-HL) based on The Peer Review of Electronic Search Strategies checklist.24 Manual searches were conducted for references cited in recent articles, systematic reviews and meta-analyses to complement the search strategy. When unpublished or forthcoming papers were found, we contacted the authors to obtain all available data, but none replied. There was no restriction on study period, ethnicity or language in the search strategy. The details of the search strategy are outlined in online supplemental appendix 1. The searched references from retrieved articles were imported into a reference management software (Endnote X7, Thomson Reuters, Philadelphia, Pennsylvania, USA) and shared with the other authors.
Supplemental material
Study selection
The study selection was conducted by two individual reviewers (HWL and C-HL) based on the PRISMA flow diagram.25 Duplicated studies were censored based on the study title and name of the first author. The two independent reviewers (HWL and C-HL) individually screened the titles, abstracts and keywords to select potentially eligible studies. The independent reviewers (HWL and C-HL) then conducted a full-text review to check for conformance with the prespecified eligibility criteria. In case of any conflict or disagreement, eligibility was discussed by all authors until a consensus was reached.
Data extraction and quality assessment
Data were extracted using a standardised format.26 HWL and C-HL extracted data on the study characteristics (first author, published or preprinted year, region, eligibility criteria, exposure to intervention and definition of severe disease) and the baseline characteristics of the patients (number of analysed patients, age, sex and comorbidities, including hypertension, diabetes mellitus, cardiovascular disease, pulmonary disease, cerebrovascular disease, chronic liver disease, chronic kidney disease and cancer). Two dichotomous variables (number of patients who died during the observation period and number of patients with severe disease) were used as clinical outcomes. We extracted adjusted risk ratios, including the OR and HR, when data were available. If the use of ACEI/ARB was evaluated only in the subpopulation with hypertension, the extraction process was conducted with a focus on the subpopulation, along with the collection of data for the whole population to determine any relevant differences.
The risk of bias (ROB) of eligible studies was assessed using the Risk Of Bias In Non-randomised Studies of Interventions (ROBINS-I) tool,27 as recommended by the Cochrane Scientific Committee in 2017. If a study was assessed to have a critical level of ROB in any domain in ROBINS-I tool, a sensitivity analysis was planned after excluding the biassed study.
Outcomes
The primary outcomes were all-cause mortality and severe disease. The definition of severe disease was according to individual study definitions.
Data synthesis and analysis
The outcomes were conservatively analysed using a random-effects model because heterogeneity was detected among the included studies regarding the study method and patient characteristics. Risk of all-cause mortality or severe disease events was calculated as the OR with a 95% CI in terms of summary statistics. The overall results of the meta-analysis were visualised with forest plots. The I2 statistic and the Cochran’s Q test were used to evaluate statistical heterogeneity among the effect sizes of the included studies.
Meta-regression analysis was conducted by using different variables including baseline characteristics, whether confounders were adjusted or not, and the definition of outcome, as a covariate. Subgroup analysis was also performed according to categorical covariates.
Funnel plot asymmetry and Egger’s and Begg’s tests were used for qualitative and quantitative evaluation of publication bias, respectively.26 If publication bias was suspected, the trim-and-fill method was planned to calculate a corrected OR by estimating the number of missing studies.28 All the analyses were performed using Stata software V.14.2 (StataCorp, College Station, Texas, USA), using the commands named “metan”, “metafunnel”, “metabias” and “metareg” and using R V.3.4.0 statistical computing software (R Foundation for Statistical Computing, Vienna, Austria) with the metafor and meta packages.29 Two-tailed p<0.05 was considered to indicate statistical significance.
Certainty of evidence
The certainty of evidence was rated using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach.30
Results
Study selection
After removing duplicates, 404 studies were screened, and 35 potentially relevant articles were retrieved for full-text review (figure 1). Twenty studies met the eligibility criteria. The reasons for excluding 15 articles are described in online supplemental appendix 2. Three studies were excluded because the data could be overlapped with other included data sources.31 The details of data sources of included studies are described in online supplemental appendix 3. All 20 studies were observational studies, and there was no randomised controlled trial reporting relevant results. All-cause mortality was reported in 13 studies,13 15–17 19–21 32–37 and severe disease was reported in 13 studies.12–14 16–18 20 34 35 38–41 Mortality was evaluated during hospitalisation in nine studies,13 15–17 19 20 32 33 35 at 28 days during hospitalisation in two studies,21 34 during hospitalisation in about 87% of patients in one study,36 and at 60 days in one study.37 Severe disease was evaluated during hospitalisation in 12 studies,12 13 16–18 20 34 35 38–41 and during hospitalisation in severe cases in 1 study,14 where about half of mild-to-moderate cases were not hospitalised.
Supplemental material
Supplemental material

Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) flow diagram for the systematic review and meta-analysis. In PRISMA flow diagram, the information of different phases of a systematic review are summarised. PRISMA flow diagram maps out the number of records identified, included and excluded, and the reasons for exclusion.
Baseline characteristics of the included studies and patients
The baseline characteristics of the included studies and patients are summarised in table 1 and online supplemental appendix 4. All studies were conducted in 2020; nine in China, four in the USA, three in Italy, one in Iran, one in South Korea, one in the UK and one other study across multiple countries. All the 36 108 patients with a confirmed diagnosis of COVID-19 were hospitalised or isolated. Among these patients, data for 30 766 patients with information on the use or non-use of ACEI/ARB were included in the meta-analysis, 8066 of whom were classified in the ACEI/ARB group. The mean age was 54.4 years and 54.5% of the included patients were men. Several comorbidities were reported, including 41.9% patients with hypertension in all 20 studies, 15.3% with cardiovascular diseases in 18 studies, 17.9% with diabetes in 17 studies, 8.8% with chronic respiratory diseases in 14 studies, 3.9% with chronic kidney disease in 12 studies, 9.1% with malignancies in 10 studies, 3.7% with cerebrovascular diseases in 8 studies and 4.6% with chronic liver diseases in 7 studies. The ACEI/ARB group was defined as those with any medication history of treatment with ACEI or ARB based on the electric medical record in 12 studies, those who used ACEI or ARB during hospitalisation in 6 studies, those who used ACEI or ARB at the time of hospitalisation in 1 study and those who were treated with ACEI or ARB within the 7 days before symptoms or during inpatient treatment in 1 study. Definitions of severe disease followed the report of the WHO-China Joint Mission on COVID-1942 for (1) respiratory rate (RR) ≥30, (2) O2 saturation at rest ≤93% and (3) PaO2/FiO2 ratio ≤300 in seven studies12 13 16 17 20 38 41; the criteria for severe disease as intensive care, mechanical ventilation or death in four studies14 18 39 40; the criteria for severe disease as (1) reduced consciousness, (2) RR ≥30/min, (3) blood pressure <90/60, (4) multilobar infiltration and (5) hypoxaemia in one study35 and the severe community-acquired pneumonia definition in the clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America43 in one study.34
Supplemental material
Characteristics of 20 included observational studies
ROB assessment within studies
The ROB assessment is summarised in online supplemental appendix 5. In general, the studies had low ROB in patient selection, classification of interventions and deviations from intended interventions, but showed moderate ROB in missing data and selection bias. Many studies did not provide sufficient information on confounding variables. The majority of studies were assessed to be vulnerable to ROB in the measurement of outcomes, which was attributed to the innate nature of a retrospective study in that the outcome assessors were aware of the intervention status, rather than to a serious or critical defect in the study design.
Supplemental material
All-cause mortality
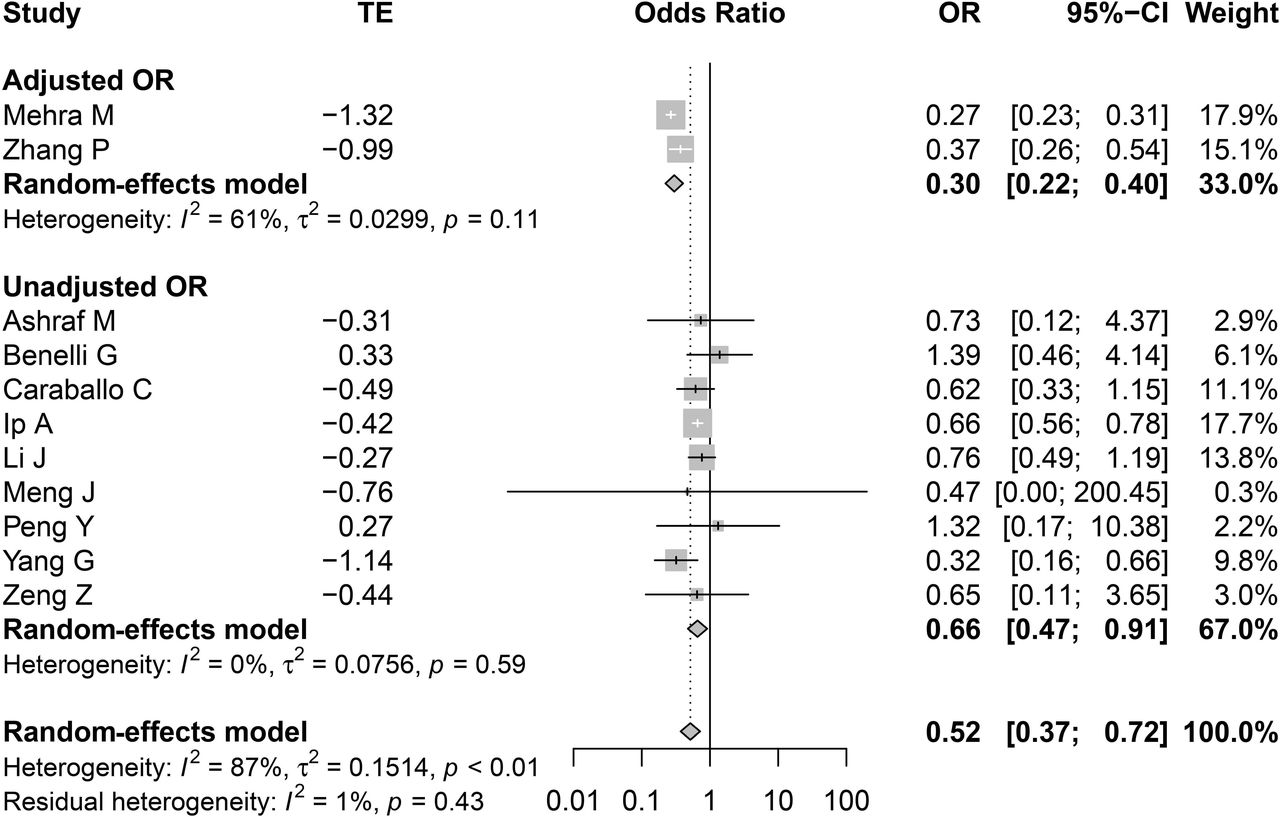
We found 21 178 patients in 11 studies reporting OR and 2 studies reporting HR. The risk of all-cause mortality was significantly decreased in the ACEI/ARB group compared with non-ACEI/ARB group with a heterogeneity (OR=0.52 (95% CI=0.37 to 0.72), I2=87%, p value for heterogeneity <0.01, figure 2) (moderate level of evidence, online supplemental appendix 6). To identify factors affecting the heterogeneity, we conducted meta-regression and subgroup analyses. A meta-regression analysis showed whether confounders were adjusted or not affected the effect size (test of moderator p<0.01). However, ACEI/ARB group had significantly lower risks of all-cause mortality than non-ACEI/ARB group in both subgroup analyses where confounders were adjusted (OR=0.30 (95% CI=0.22 to 0.40); I2=61%, p value for heterogeneity=0.11, figure 3) and where confounders were not adjusted (OR=0.52 (95% CI=0.37-0.72); I2=0%, p value for heterogeneity=0.59, figure 3). There were no other factors affecting the effect size in meta-regression analyses by using the following covariates: ‘including hypertensive patients only or not’ (test of moderator p=0.92), ‘the age of participants aged ≥60 or <60 years’ (test of moderator p=0.19) or ‘male proportion ≥50% or <50%’ (test of moderator p=0.89). ACEI/ARB group was associated with decreased risk of all-cause mortality in hypertensive patients-only subgroup (OR=0.53 (95% CI=0.39 to 0.73); I2=87%, p value for heterogeneity=0.04, online supplemental appendix 7). ACEI/ARB group was associated with decreased risk of all-cause mortality in both subgroups of age ≥60 and <60 years (online supplemental appendix 8) and was also associated with decreased risk of all-cause mortality in both subgroups of male proportion ≥50% and <50% (online supplemental appendix 9). The sensitivity analysis excluding three studies, in which the definition of mortality was not ‘in-hospital mortality’ but ’28 days mortality’21 34 or not all patients were hospitalised,36 showed a similar result (online supplemental appendix 10).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material

Forest plot of for all-cause mortality using OR. All-cause mortality data of OR and 95% CI from 11 studies were pooled in this meta-analysis using random-effects model and the result of meta-analysis was described as a forest plot. The square and horizontal line indicated the OR and 95% CI of individual study that was also described in the right side of the forest plot. The diamond on the bottom of this forest plot indicated a pooled OR and 95% CI. TE, treatment effect.
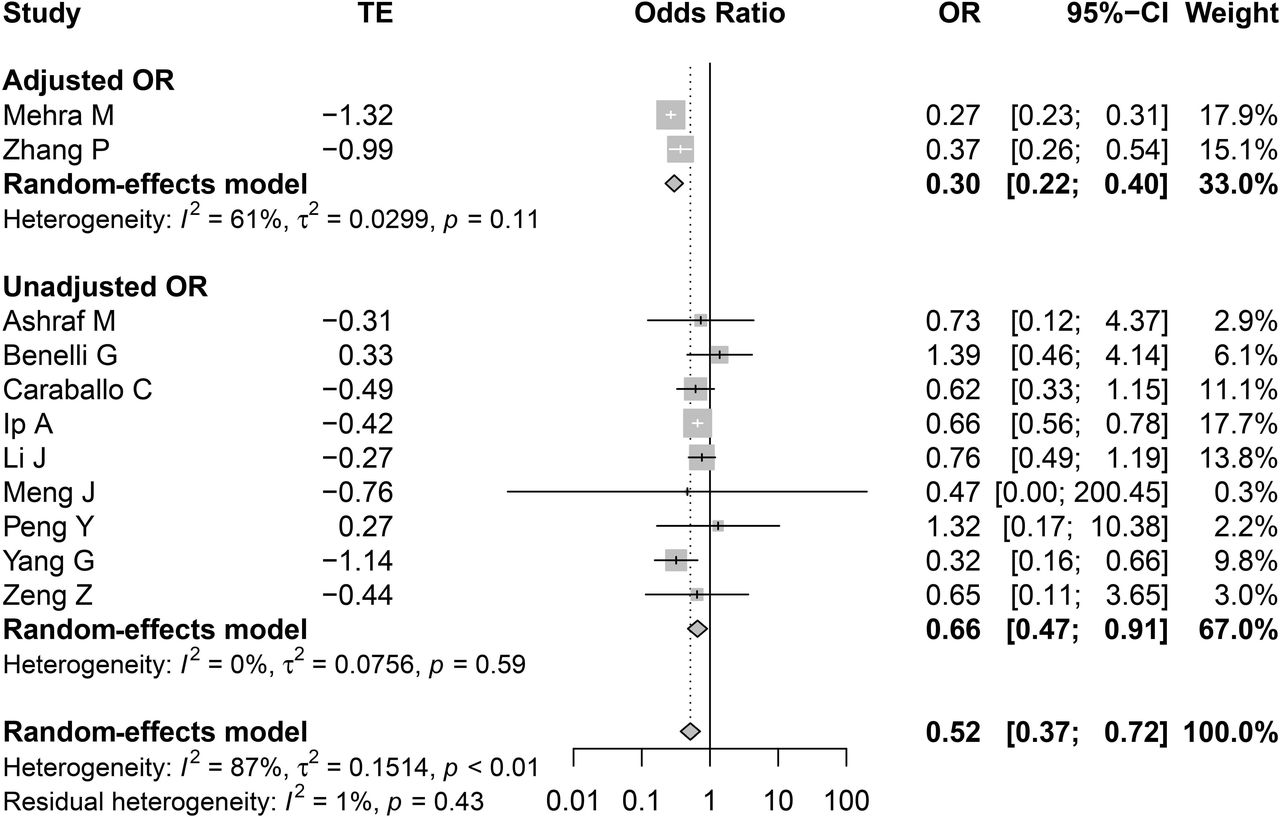
Forest plot for all-cause mortality in adjusted OR and unadjusted OR. Subgroup analysis for all-cause mortality was conducted according to adjusted or unadjusted OR. The square and horizontal line indicated the OR and 95% CI of individual study that was also described in the right side of the forest plot. The diamond of this forest plot indicated a pooled OR and 95% CI in each subgroup analysis and in overall population. Meta-regression analysis performed using ‘unadjusted versus adjusted’ as the covariate affected the effect size (test of moderator, p<0.001). TE, treatment effect.
There were two studies applying HR to compare the risk of all-cause mortality between ACEI/ARB group and non-ACEI/ARB group. Because those studies included patients with largely different characteristics such as age (44.437 vs 76.0 years19), male proportion (38.5%37 vs 72.3%19) and the proportion of hypertensive patients (19.0%37 vs 100%),19 we did not perform a meta-analysis. Both the study by Lee et al (HR=1.07 (95% CI=0.66 to 1.74))37 and the study by Tedeschi et al (HR=0.97 (95% CI=0.68 to 1.38))19 showed that ACEI/ARB use did not increase the risk of all-cause mortality compared with non-ACEI/ARB group.
Severe disease in COVID-19
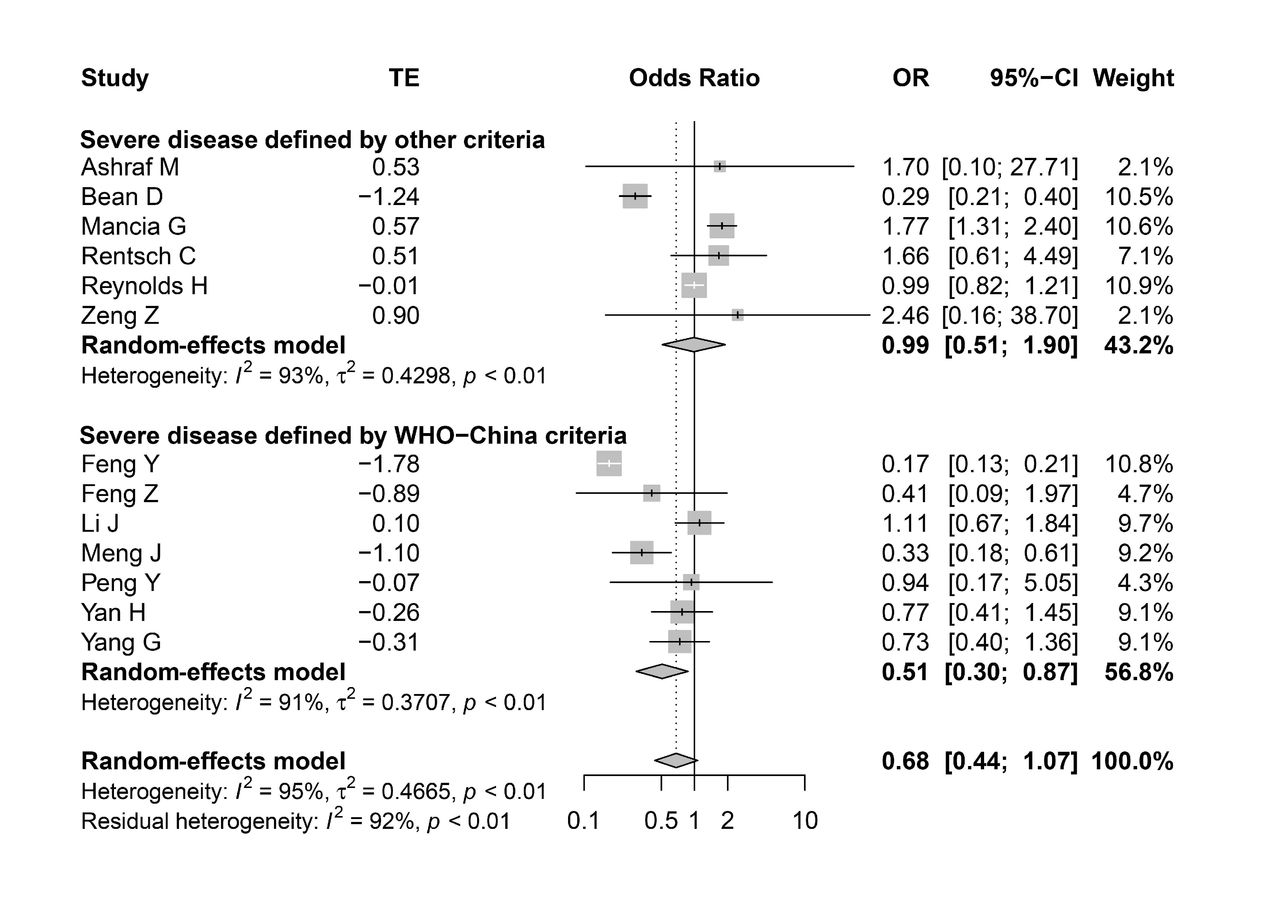
For 12 848 patients in 13 studies, ACEI/ARB use was not associated with an increased risk of severe disease manifestation in a meta-analysis using a random-effects model, although there was a significant heterogeneity (OR=0.68 (95% CI=0.44 to 1.07); I2=95%, p value for heterogeneity <0.01, figure 4) (low level of evidence, online supplemental appendix 6). We conducted a various meta-regression, but did not identify a contributor of heterogeneity among the following covariates: ‘confounders were adjusted or not’ (test of moderator p=0.99), ‘including hypertensive patients only or not’ (test of moderator p=0.35), ‘the age of participants ≥60 or <60 years’ (test of moderator p=0.21) or ‘male proportion ≥50% or <50%’ (test of moderator p=0.58). Whether the definition for severe disease followed the WHO-China criteria or not also did not affect the effect size (test of moderator p=0.17). ACEI/ARB group did not have a higher risk of severe disease than ACEI/ARB group both in subgroup of studies defining severe disease according to WHO-China criteria (OR=0.51 (95% CI=0.30 to 0.87)) and in subgroup of studies defining severe disease according to other criteria (OR=0.99 (95% CI=0.51 to 1.90)) (figure 5). ACEI/ARB was not associated with increased risk of severe disease in all other subgroup analyses, although there were statistical heterogeneities in majority of subgroup analysis (online supplemental appendices 11–14. The sensitivity analysis excluding one study,14 in which not all patients were hospitalised, showed a similar result (online supplemental appendix 15).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material

Forest plot for severe disease using OR. Severe disease data of OR and 95% CI from 13 studies were pooled in this meta-analysis using random-effects model and the result of meta-analysis was described as a forest plot. The square and horizontal line indicated the OR and 95% CI of individual study that was also described in the right side of the forest plot. The diamond on the bottom of this forest plot indicated a pooled OR and 95% CI. TE, treatment effect.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for severe disease according to the definition of severe disease. Subgroup analysis for severe disease was conducted according to whether the definition of severe disease followed WHO-China criteria or not. The square and horizontal line indicated the OR and 95% CI of individual study that was also described in the right side of the forest plot. The diamond of this forest plot indicated a pooled OR and 95% CI in each subgroup analysis and in overall population. Meta-regression analysis performed using ‘defined by WHO-China criteria versus other criteria’ as the covariate did not affect the effect size (test of moderator, p=0.1657). TE, treatment effect.
Publication bias
Observation of funnel plots supported by Egger’s and Begg’s tests indicated no significant publication bias for the associations with mortality and severe disease (online supplemental appendix 16).
Supplemental material
Discussion
To our knowledge, this is the systematic review and meta-analysis investigating the association between ACEI/ARB treatment and the risk of mortality and severe disease in patients with COVID-19 first registered in PROSPERO. ACEI/ARB use was significantly associated with a decreased risk of all-cause mortality in meta-analysis for studies using ORs. Two studies using HR did not show an increased risk of all-cause mortality in ACEI/ARB group compared with non-ACEI/ARB group. Thus, we concluded that ACEI/ARB did not increase the risk of all-cause mortality in patients infected with SARS-CoV-2. ACEI/ARB use was not associated with an increased risk of severe disease, although there was a significant heterogeneity. We rated moderate certainty of evidence for all-cause mortality and low certainty of evidence for severe disease, mainly rated down due to the limitation of retrospective study design. Overall, the continuation of ACEI/ARB use during the COVID-19 pandemic can be a suitable strategy as current guidance suggested.11
Hypertension, cardiovascular diseases and diabetes are the most common comorbidities of patients with severe disease in COVID-19,44 which are commonly treated with ACEI/ARBs. Researchers have postulated that ACEI/ARB use could be a link between more frequent cases of severe disease symptoms in patients with comorbidities.44–47 This is based on the fact that ACEI/ARBs were found to upregulate ACE2 expression in rats and human intestinal cells.2–4 Since ACE2 is the receptor for SARS-CoV-2 entry in the host cell,5 6 ACEI/ARB use could facilitate worse symptoms in patients with COVID-19.44–47
However, our study does not support this speculation; it even suggests a potential benefit of ACEI/ARB for some COVD-19 patients given that a decreased risk of all-cause mortality was observed in the meta-analysis for studies using ORs. The biological mechanism of these beneficial effects with ACEI/ARB could be explained from two perspectives.48 First, ACEI/ARBs inhibit the activity of angiotensin II, which increases blood pressure, retention of sodium and water,49 inflammation50 and tissue injury.51 Thus, these drugs attenuate lung and cardiovascular insults, which could prevent severe disease and death.52 In fact, serum angiotensin II levels were found to be markedly elevated and linearly associated with viral load and lung injury in patients with COVID-19.53 Second, ACEI/ARBs upregulate ACE2, which is expressed in the heart, lung, intestine and kidneys.54 Human coronaviruses downregulate ACE2 expression on cell membranes after invading cells,55 56 thereby enhancing neutrophil infiltration in the lungs.57 Since angiotensin II is the main substrate of ACE2, the increase in ACE2 levels by ACEI/ARBs could mitigate the harmful effects of angiotensin II. ACE2 also degrades angiotensin I to angiotensin-(1-9), inducing anti-inflammatory, anti-oxidative and vasodilating effects through binding to the Mas receptor.11 In fact, some previous studies suggested that ACEI/ARBs may have a beneficial effect in preventing pneumonia58 59 and in improving the outcomes of patients with acute respiratory distress syndrome.60 The study of Meng et al,16 which was included in our meta-analysis, demonstrated no difference in viral load at baseline, although the peak viral load was significantly lower in the ACEI/ARB group than in the non-ACEI/ARB group (p=0.03).
Our study has limitations. First, the interpretation of the results from our systematic review and meta-analysis should be careful because of high ROB from observational studies. According to GRADE approach, we attenuated the certainty of our conclusions. Second, the definition of severe disease was heterogeneous among studies. Seven studies defined severe disease based on the WHO-China criteria, and six studies used other different criteria. The heterogenous definition for severe disease may have led to a significant statistical heterogeneity in the meta-analysis (I2=91%, p value for heterogeneity <0.01). Although ACEI/ARB group did not increase the risk of severe disease both in subgroup of studies defining severe disease according to WHO-China criteria and in subgroup of those using other criteria, the results should be cautiously interpreted considering the heterogeneity of outcome definition and the statistical heterogeneity. Third, there were a little bit different time points when the outcomes were evaluated. Most studies evaluated severe disease and mortality during hospitalisation. However, in the study by Mancia et al, half of patients with non-severe disease were not hospitalised, although all patients with severe disease were hospitalised. In the study by Caraballo et al, about 87% of patients with COVID-19 were hospitalised and in-hospital mortality was evaluated. We postulated the patients with COVID-19 who were not hospitalised as those with mild disease who recovered spontaneously without hospitalisation. The studies by Zeng et al and Zhang et al used 28 days mortality. However, we performed sensitivity analysis, excluding those studies, which showed similar results. Fourth, we found significant interstudy heterogeneities in meta-analyses for all-cause mortality and severe disease. To identify factors contributing on interstudy heterogeneity, we conducted meta-regression analysis and subgroup analysis. We identified whether confounders were adjusted or not significantly affect the effect size for all-cause mortality and conducted subgroup analysis according to confounders were adjusted or not. However, both subgroup analysis showed that ACEI/ARB group did not have a higher risk of all-cause mortality than non-ACEI/ARB group as described above. Fifth, although all the included studies fulfil the eligibility criteria stipulated in the present systematic review, there were several inconsistent participant criteria because of eligible age (all adults vs ≥40 years old), comorbidities (general population vs specific disease cohort) and indications to exclude specific comorbid diseases.
Conclusions
The ACEI/ARB treatment does not increase the risk of all-cause mortality in patients with COVID-19. ACEI/ARB use does not increase the risk of severe disease, although the heterogeneous outcome definition and the statistical heterogeneity should be considered. Physicians can prescribe ACEI/ARB without concern of drug-related worsening in patients with COVID-19.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data are available by accessing the published studies listed in table 1.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study concept and design: HWL and C-HL. Acquisition of data: HWL and C-HL. Analysis and interpretation of data: HWL and C-HL. Manuscript drafting: HWL and C-HL. Critical revision of the manuscript and important intellectual content: EJJ and C-HY. Study supervision: C-HL.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Linked Articles
- Airwaves