Article Text

Abstract
SARS-CoV-2 infection is a multisystem disease with post-discharge sequelae. We report early follow-up data from one UK hospital of the initial 200 hospital inpatients with slow recovery from the condition. At 4 weeks post-discharge, 321/957 survivors (34%) had persistent symptoms. A structured outpatient clinical assessment protocol was designed, and outcomes from the first 200 patients seen 4–6 weeks post-discharge are presented here. In 80/200 (40%), we identified at follow-up a cardiorespiratory cause of breathlessness, including persistent parenchymal abnormality (64 patients), pulmonary embolism (four patients) and cardiac complications (eight patients). These findings occurred both in patients who had intensive care unit (ICU) admissions and those who had been managed on the ward, although patients requiring ICU admissions were more likely to have a significant cardiorespiratory cause found for their breathlessness, risk ratio 2.8 (95% CI 1.5 to 5.1).
- viral infection
- respiratory infection
- systemic disease and lungs
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Background
On 11 March 2020, WHO declared SARS-CoV-2 or COVID-19 a global pandemic. As of late December 2020, 2 149 551 cases had been recorded in the UK.1 The long-term outcome for these patients is unknown. However, recent studies indicate potential long-term complications ranging from disturbance of taste/smell,2 cough,3 fatigue and dyspnoea2–5 to more pronounced cardiac,6 respiratory3 4 7 and cognitive dysfunction.3 7
Method
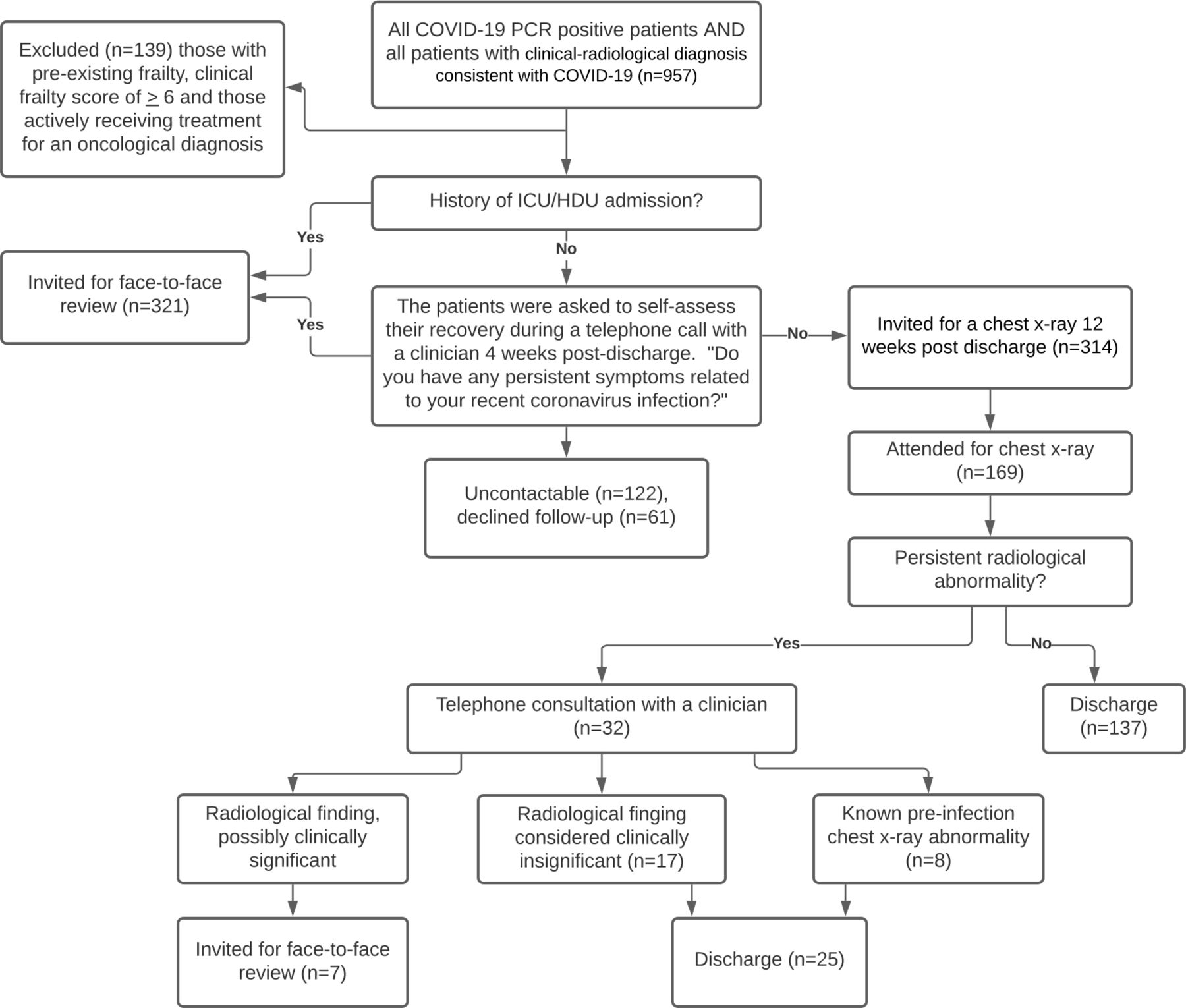
As the early Guy’s and St Thomas’ Hospital patients diagnosed with COVID-19 were being discharged, a post-COVID clinic was established to address the unmet needs of those with persistent symptoms. All patients attending the Hospital with either a positive PCR for COVID-19 or a negative PCR but a clinical-radiological diagnosis were telephoned 4 weeks after discharge. Those with persistent symptoms and those who had required intensive care unit (ICU) admission were invited for review. Those reporting a return to baseline were offered a chest radiograph at 12 weeks, consistent with national guidance.8
Patients attending the clinic were evaluated 4–6 weeks post-discharge by Respiratory or Infectious Disease Specialists. Further details of the follow-up pathway are found in figure 1. History and physical examination were undertaken; data collected on baseline characteristics and function; chest radiograph and blood tests performed; and health status questionnaires completed. Patients completed a 6 min walk test (6MWT) where physically able.
{kind=link}
Post-discharge follow-up pathway outcomes. ICU, intensive care unit; HDU, high dependency unit.
Further assessment was based on physiological impairment and patient-reported symptoms. Available investigations included: dual energy CT or high-resolution CT, ventilation-perfusion scanning, spirometry with gas transfer (limited due to the aerosol-generating nature of the procedure), echocardiography and ECG. Onward referral to other specialist teams for early assessment was effected.
Data collected was analysed using SPSS V.27 (IBM). Variables are expressed as mean±SD for parametrc data or median ±IQR for non-parametric data. ICU versus non-ICU values are compared either by independent samples t-test for parametric variables or by mann-whitney U test for non-parametric variables. Risk ratios are calculated using a Χ2 analysis.
Results
By the end of May 2020, 1272 patients had been diagnosed with COVID-19 of whom: 1239 (97%) had PCR-confirmed disease; 241 (19%) patients had died; 74 (6%) remained as inpatients. Of the remaining 957 patients: 122 (13%) were uncontactable, 61 (6%) declined any further follow-up, 139 (15%) were considered unsuitable to attend clinic because they were housebound due to frailty or because they were unwell with unrelated conditions; 314 (33%) had returned to functional baseline. Three hundred and twenty-one (34%) patients reported persistent symptoms and were invited for clinical review. We report data from the first 200 patients with a PCR confirmed diagnosis who were seen due to persistent symptoms.
The mean age was 54.8±15.0, 61.5% were male and the majority were overweight (mean body mass index 28.8±6.1). Further characteristics are described in table 1.
Baseline characteristics.
Of the 200 seen, 179 had received inpatient care, the remaining 21 patients been discharged directly from the emergency department. The majority had not been critically unwell and only 55 (27.5%) patients had ever received mechanical ventilation. Other features of their admission are highlighted in table 2.
Admission characteristics
During evaluation (table 3), patients reported their Medical Research Council (MRC) dyspnoea score (graded 1–5) post-illness and retrospectively graded their baseline score pre-illness. A persistent deterioration of two or more MRC points was observed in 36 (18%) patients. Of the 170 patients that underwent 6MWT, 34 (20%) had an oxygen desaturation of 4% or more. Of those that went on to complete lung function tests (n=59), 16 (27%) had a predicted forced vital capacity of 80% or less and 26 (44%) had a transfer factor for carbon monoxide of 70% or less. Screening for anxiety and depression, using standardised tools, identified similar prevalence to that seen in general medical inpatients.9
Structured assessment clinic.
The dominant finding in those seen was persistent interstitial change in 64 (32%) patients on CT. Other respiratory findings included 4 (2%) patients with a previously unidentified pulmonary embolus, lung infarcts (n=2), Klebsiella pneumonia (n=1) and Pneumocystis jirovecii pneumonia (n=1). Either a previously undiagnosed or deterioration of existing cardiac cause for ongoing symptoms was found in eight patients (4%): pericarditis, persistent sinus tachycardia, hypertrophic cardiomyopathy and inferior regional wall motion abnormality, an atrial septal defect with new reversal of shunt, pulmonary hypertension, left ventricular hypertrophy and worsening of pre-existing heart failure.
Asymptomatic patients were followed up as per national guidance with chest radiograph at 12 weeks, 169/314 (54%) attended. Of these, 137 (81%) patients had a film reported as normal by a radiologist. The remaining patients were reviewed by telephone, 8 (2.5%) had known preinfection abnormalities to their chest X-ray but 24 (14%) had residual parenchymal change. Seventeen patients (10%) had no symptoms or change in function and so no further follow-up was arranged. For 7/169 (4%) cases, possible persistent issues were identified and these patients were offered face-to-face clinical assessment.
Discussion
With the COVID-19 global pandemic yet to peak, these early results indicate likely long-term morbidity in a significant number of patients. Of those seen, 119/200 (60%) had persistent subjective symptoms despite no radiological or physiological abnormality being identified and these patients with ‘post-COVID-19 syndrome’ are likely to create a considerable healthcare management dilemma. However, 40% of those seen did have a significant finding. A limitation of our work is that only symptomatic patients were physically reviewed, and while only 4% of these patients went on to have significant findings requiring further follow-up, we advise screening for persistent symptoms in all patients in the weeks after discharge to ensure complications are identified. In addition, given these patients were admitted early in the pandemic, our non-ICU cohort had relatively mild disease, with only 50% requiring oxygen therapy. These findings suggest that more thorough follow-up of patients is indicated than is currently recommended under the BTS guidance,8 and support the more robust approach advised in by the recently published National Institute for Health and Care Excellence guidelines.10 The outcome of this cohort of early patients highlights the current limitations of our knowledge of COVID-19 recovery. Planned studies, such as the UK-based post-hospitalisation COVID-19 study (PHOSP-COVID), will further elucidate the clinical trajectory and improve understanding of differences in patient outcomes.
Acknowledgments
The authors would like to acknowledge the work of all those involved in successfully establishing the clinic: S Agarwal, L Ahmed, C Batista, R Breen, G D’Ancona, J Dhariwal, C Francis, A Hearn, B Hirons, O Kadwani, D Jackson, A Jones, B Lams, A Nanzer-Kelly, G O’Hara, K UrRehman, E Suh, the radiologists, physiologists, nursing staff, physiotherapists and administration staff. We would additionally like to thank the junior doctors at Guy’s and St Thomas’ Hospital who supported the project.
Footnotes
Contributors AD and AW conceived of the idea. JLL was responsible for data entry and data managment. KM, TM and JH were reposonsible for performing the computations. KM verified the analytical methods. JH wrote the manuscript with KM. AD, AW and BM supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This project was approved internally for service improvement (reference 11627).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves
- Editorial