Article Text

Abstract
Large numbers of people are being discharged from hospital following COVID-19 without assessment of recovery. In 384 patients (mean age 59.9 years; 62% male) followed a median 54 days post discharge, 53% reported persistent breathlessness, 34% cough and 69% fatigue. 14.6% had depression. In those discharged with elevated biomarkers, 30.1% and 9.5% had persistently elevated d-dimer and C reactive protein, respectively. 38% of chest radiographs remained abnormal with 9% deteriorating. Systematic follow-up after hospitalisation with COVID-19 identifies the trajectory of physical and psychological symptom burden, recovery of blood biomarkers and imaging which could be used to inform the need for rehabilitation and/or further investigation.
- viral infection
- respiratory infection
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Large numbers of people are being discharged from hospital following COVID-19 without systematic assessment of their recovery and need for rehabilitation or further investigation to detect complications. Initial reports are emerging of significant ongoing symptom burden1 termed ‘Long-COVID’, and of changes in lung function2 and imaging.3
Method
We rapidly established a post-COVID follow-up service across three large London hospitals, collecting data to identify unmet health needs and to identify people requiring additional rehabilitation and/or investigation for complications. In brief, we aimed to follow up all SARS-CoV-2 positive COVID-19 admissions by phone or in-person four-to-six weeks after discharge. Key symptoms were graded as absent, or present on an 11-point (0-10) scale in which a higher score was more severe. We invited people with abnormal blood tests or imaging at discharge to repeat these. Imaging was classified using British Society of Thoracic Imaging criteria.4 Full details of our follow-up procedures and protocol are included as an online supplemental appendix.
Supplemental material
Results
This report summarises the clinical assessment of 384 patients reviewed a median of 54 (IQR 47–59) days following hospital discharge with COVID-19. Three hundred eighty-four patients represent 34% of the total number of patients with COVID-19 discharged during this period (online supplemental figure 1). Of the 479 patients we attempted to contact, we were able to complete the call in 395 (82%) and of these only 11 (2.8%) declined to participate. Data for 79 of the 95 patients in who we were unable to complete the follow-up demonstrate similar age, sex, ethnicity and comorbidity to those we were able to follow-up.
The characteristics of the 384 participating subjects, and a summary of their COVID-19 admission are reported in table 1. In brief, the population had a mean age of 59.9 years and were predominantly male. Only 34% had no reported comorbidity. Forty-three per cent were from a black, Asian or minority ethnic background. Eight per cent of the cohort was obese. The median length of hospital stay was 6.5 (4–10.75) days and 14.5% required admission to intensive care.
Baseline characteristics, features of the acute COVID illness and symptom persistence at follow-up following hospital discharge
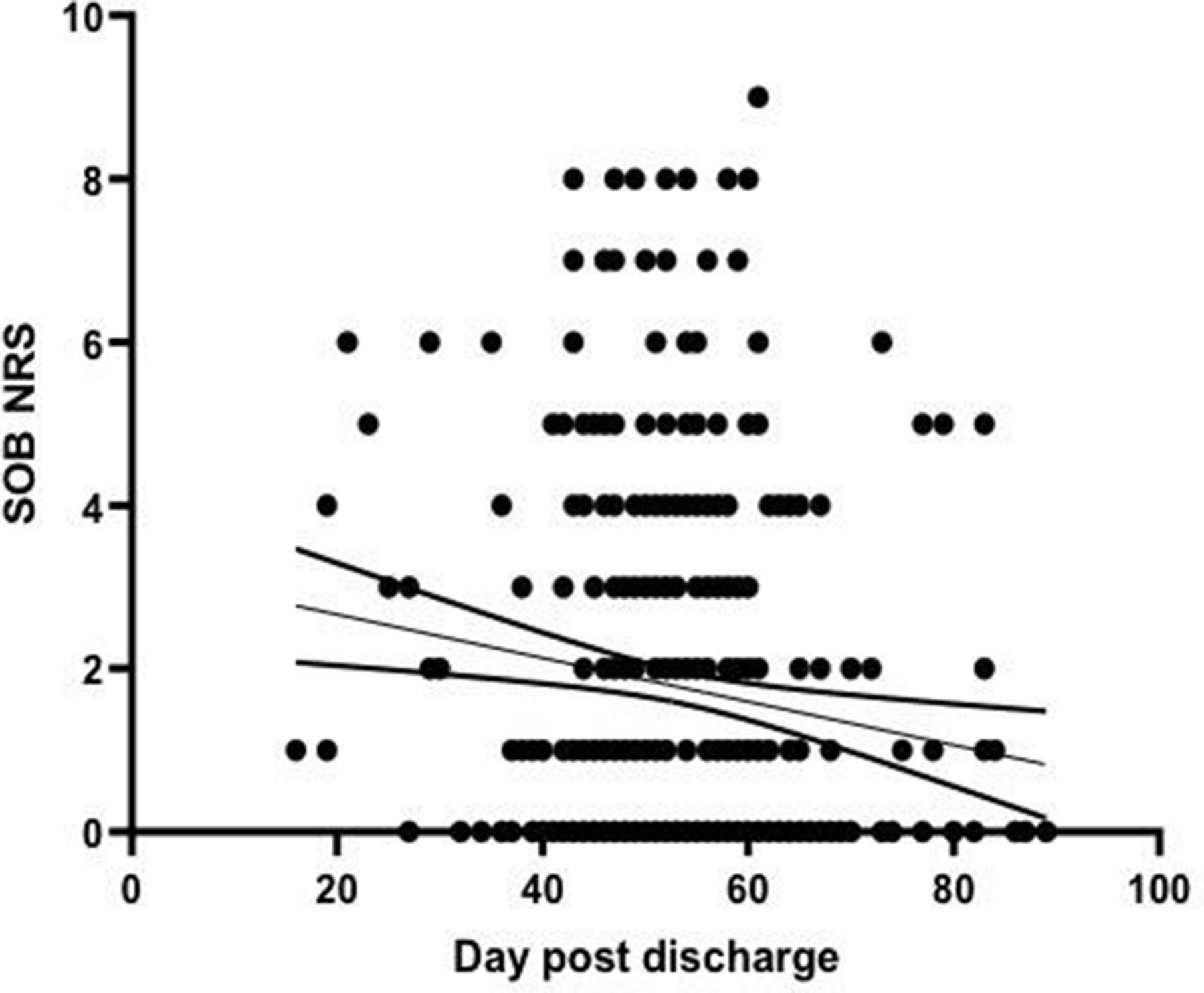
Patients graded their overall recovery health as a median (IQR) 90 (75–100)% compared with 100% best health. Recovery towards usual health was lower in those with comorbidity (as listed in table 1) compared with those without: 85 (70–100)% versus 92.5 (80–100)%, p=0.007. Persistence of symptoms at follow-up, by level of acute respiratory support, is reported in table 1. Follow-up symptoms were least prevalent in those treated with oxygen alone. Further detail on the assessment of physical symptoms at follow-up is reported in online supplemental table 1, including symptom intensity in relation to maximum, and the proportions reporting the trajectory of symptoms to be improving, unchanged or deteriorating. For all symptoms at follow-up, there was a statistically significant improvement from maximum intensity to follow-up (p<0.0001). In those with persistent breathlessness, patients assessed earlier post discharge tended to have higher breathlessness scores (figure 1) suggesting a trend to improvement over time. The trajectory for cough, fatigue and sleep quality is illustrated as online supplemental figures 2–4. 14.6% of participants had a PHQ2 score of greater than 3 indicating significant depression.

{kind=link}
Patient reported breathlessness (0–10 scale) versus time of follow-up from hospital discharge. Each circle represents an individual patient at follow-up, with interpolation line and 90% CI. A higher score represents more severe breathlessness.
The results of blood investigations at admission, the last time point prior to discharge and follow-up, are reported in table 2. Overall, despite significant abnormalities at discharge, blood test results had returned to normal levels in the majority of patients at follow-up. Of those with abnormal discharge results and who attended for further blood tests, 7.3% of 247 patients had persisting lymphopaenia, 30.1% of 229 patients had elevated d-dimer and 9.5% of 190 patients had elevated C reactive protein (CRP). The d-dimer value was decreasing over time (online supplemental figure 5).
Blood investigations at admission to hospital, discharge and follow-up
At presentation, 333/384 (87%) patients had a chest radiograph performed. Of these, 49 (15%) were normal, 188 (56%) were typical of COVID-19 and 96 (29%) were indeterminate for or unlikely to represent COVID-19. Of the radiographs classified as typical for COVID-19, 4 did not have a severity grading, 49/188 (26%) were reported as mild, 78/188 (41%) as moderate and 57/188 (30%) as severe.
Of the 244/384 (66%) patients that had follow-up radiographs, 151 (62%) radiographs were normal, 66 (27%) demonstrated significant improvement, 4 (2%) were unchanged and 23 (9%) showed significant deterioration. Of the patients with radiographs that demonstrated worsening at follow-up, 2/23 (9%) had been normal at presentation, 10/23 (43%) had been typical for COVID-19 and 11/23 (48%) had been indeterminate for or unlikely to represent COVID-19.
14.8% of follow-up patients were deemed to require further assessment with CT chest imaging, pulmonary function tests, other investigations or a face-to-face review.
Discussion
Our data show that while symptom burden in subjects recovering from hospital admission with COVID-19 had generally improved at early follow-up, 53% reported persistent breathlessness, 34% persistent cough and 69% persistent fatigue. Fifteen per cent were depressed. Of people who attended for repeat imaging and blood tests because investigations on discharge had been abnormal, 9% had a deteriorating chest radiograph appearances at follow-up, and 30.1% and 9.5% had persistently elevated d-dimer and CRP concentration respectively. COVID-19 is associated with increased risk of thrombosis5 but the significance of the persistent elevation in d-dimer is unclear. Deteriorating chest radiograph appearances raise the possibility of developing lung fibrosis. These data are compatible with studies reporting longer term abnormalities in SARS survivors,6 and initial data emerging from smaller COVID-19 cohorts.1 7
There are strengths and weaknesses to this analysis. We only included those who tested positive for SARS-CoV-2, and patients requiring prolonged ICU and inpatient stay may be under-represented in this early analysis. Comparing against maximal symptoms risks recall bias and other symptoms such as chest pain may also be important. Not all participants were willing to take part in the review, or attend for investigations, potentially introducing selection bias. We cannot determine if these features are unique to COVID-19 or similar to those following admission for other critical respiratory illness.
To conclude, we provide the first report of physical and psychological symptom burden, blood markers and chest imaging trajectory following discharge for a hospitalised episode of COVID-19. We have identified persisting symptoms and radiological abnormalities in a significant proportion of subjects. These data may assist with the identification of people outside expected recovery trajectories who could benefit from additional rehabilitation and/or further investigation to detect post-COVID complications. Identifying which patients have persistent dyspnoea due to complications rather than deconditioning alone is an important question for future research.
Acknowledgments
This work was partially undertaken at UCLH/UCL which received a proportion of funding from the Department of Health NIHR Biomedical Research Centre funding scheme. JJ was supported by a Wellcome Trust Clinical Research Career Development Fellowship: 209553/Z/17/Z.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lungdiagnosis, @lungradiologist, @drjoporter
Collaborators The ARC Study Group: Aishah Ahmed, Asia Ahmed, Andrea Bangay, Izumi Barbor, Meg Barber, James Batty, Thea Buchan, Tom Burns, Alisha Chauhan, Ben Cooper, Roise Dudley, Mark Duncan, Nada Elsaid, Rebecca Evans, Samuel Flatau, Lydia Gabriel, James Goldring, Heather Groombridge, Liam Healy, Neel Jain, Afshan Khan, Camila Nagoda Niklewicz, Ezgi Ozcan, Preena Patel, Shivani Patel, Alexander Procter, Alice Ring, James Robertson, Portia Sagoe, Anita Saigal, George Seligmann, Runil Shah, Magali Taylor, Andrew Wendruff and Hannah Woodcock.
Contributors SM, SEB, JSB, MH, TEH, MCIL, JCP and JRH developed the clinical follow-up protocol. JB, JJ, SSH and AN developed and led the radiology protocols and analysis. SM, EKD, MH, HCJ, SBN and GST delivered and supported the follow-up process at three hospital sites. SM led the initial data analysis. JRH developed the first draft of the manuscript. All authors revised the manuscript for important intellectual content and approved the final version for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.