Article Text

Abstract
Although nasal continuous positive airway pressure or non-invasive ventilation is used to manage some patients with acute lung injury due to COVID-19, such patients also demonstrate increased minute ventilation which makes it hard, if the device is used in line with the manufacturer’s instructions, to achieve adequate oxygen delivery. In addition, if a hospital contains many such patients, then it is possible that the oxygen requirements will exceed infrastructure capacity. Here we describe a simple modification of two exemplar ventilators normally used for domiciliary ventilation, which substantially increased the fraction of inspired oxygen (FiO2) delivered.
- non invasive ventilation
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Acute respiratory distress is a life-threatening complication of COVID-19.1 If severe, this is managed by endotracheal ventilation followed by a lung-protective ventilation strategy, however, this is not universally applied. First, symptoms may be milder so that the treating clinician feels that a non-invasive approach is justifiable; second, comorbidities or frailty may be such that an invasive approach is judged inappropriate; and third, it is possible, even in resource-rich countries, that facilities for invasive ventilation may be overwhelmed. Thus, there has been interest in increasing the amount of ventilatory support available by, for example, using one ventilator to treat two patients, although it is accepted that this is a ‘last resort’ solution.2 3
Another ‘last resort’ approach could be the use of devices for domiciliary non-invasive ventilation (NIV) that are inexpensive and commonly available. If effective, this solution would avoid the ethical issues associated with ‘two for one’ therapy.4 However, these devices are typically intended for use during sleep where minute ventilation is <10 L/min.5 Minute ventilation during acute COVID-19 infection has not been documented (and might be potentially hazardous to investigators wishing to do so due to the risk of viral transmission by aerosol), but anecdotal reports suggest that it may exceed 30 L/min. Under these circumstances, even adding oxygen at a constant flow of 15 L/min, the maximum provided by a standard wall supply, into the circuit may fail to give a sufficiently high FiO2.
Here we describe a solution using, as exemplars, two commonly available devices for domiciliary ventilation. We chose the devices to test on the basis that one of them has a dedicated oxygen inlet port and internal blender; the other does not. In essence, our solution was to capture the gas mixture discarded by the machine during expiration so that in the subsequent inspiration, the machine drew from an oxygen-enriched gas mixture and mixed it with oxygen added in the normal manner. Of note, although conventional wall-mounted O2 flowmeters are only calibrated to 15 L/min, oxygen flow may be as high as 60 L/min if the tap is open fully. We appreciate that clinical imperative may lead some users to do so in an attempt to increase FiO2, but this practice, in combination with increased patient numbers, may overload a hospital’s oxygen supply.6
We compared the delivered FiO2 before and after modifications with different levels of O2 delivered through the oxygen inlet. We used a calibrated Fluke 52 II Thermometer (Norwich, UK) to assess any potential excessive heat of the ventilator when used with the modification assembly in situ. We ran the Vivo 2 for up to 4.5 days. We found only small temperature variations (~1°C), which could be attributed to environmental temperature fluctuations. FiO2 was measured using an ENVITEC O2 analyser and a Fluke VT PLUS HF Gas flow analyser connected to a Fluke ACCU LUNG also allowed measurement of minute ventilation and tidal volume.
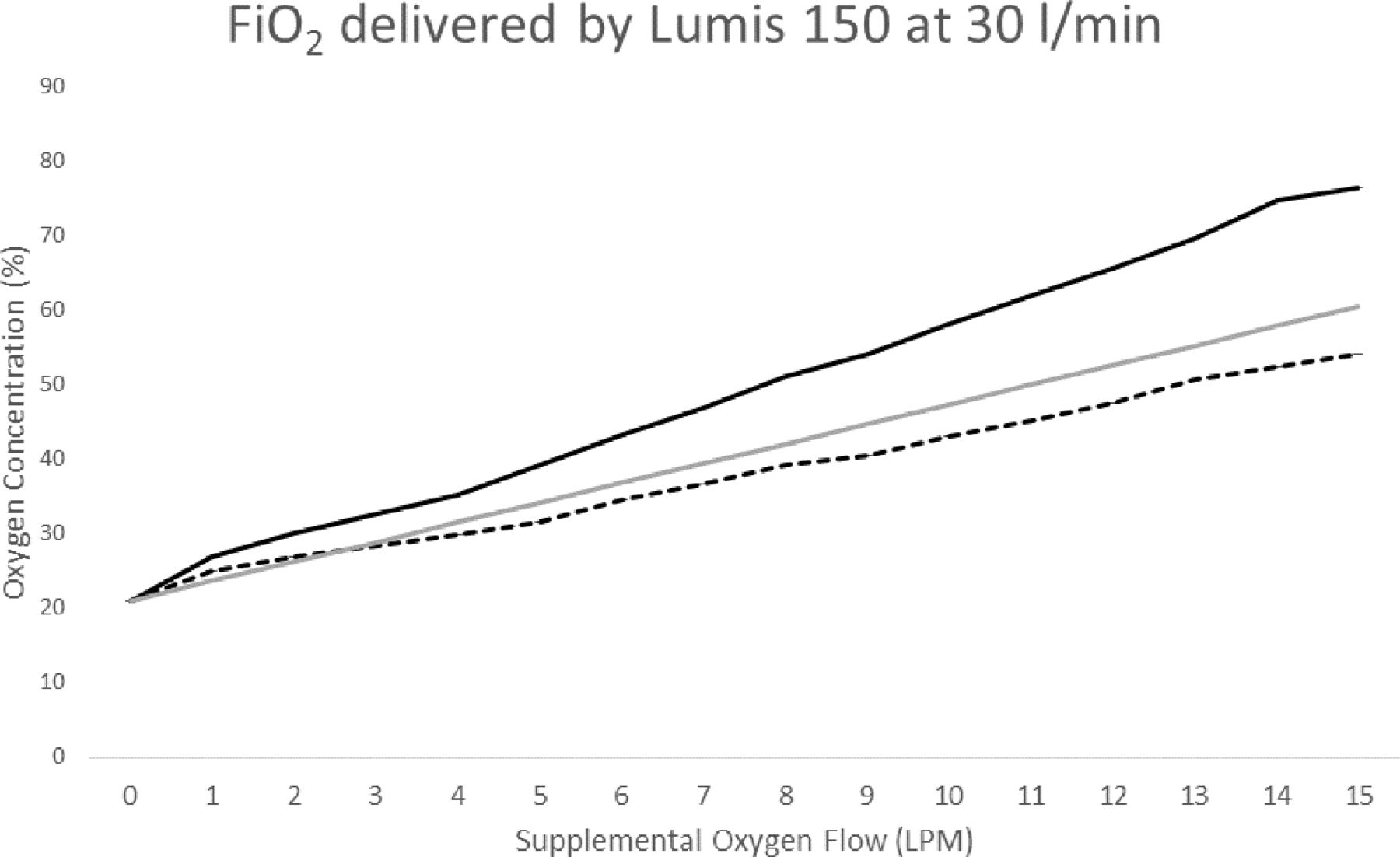
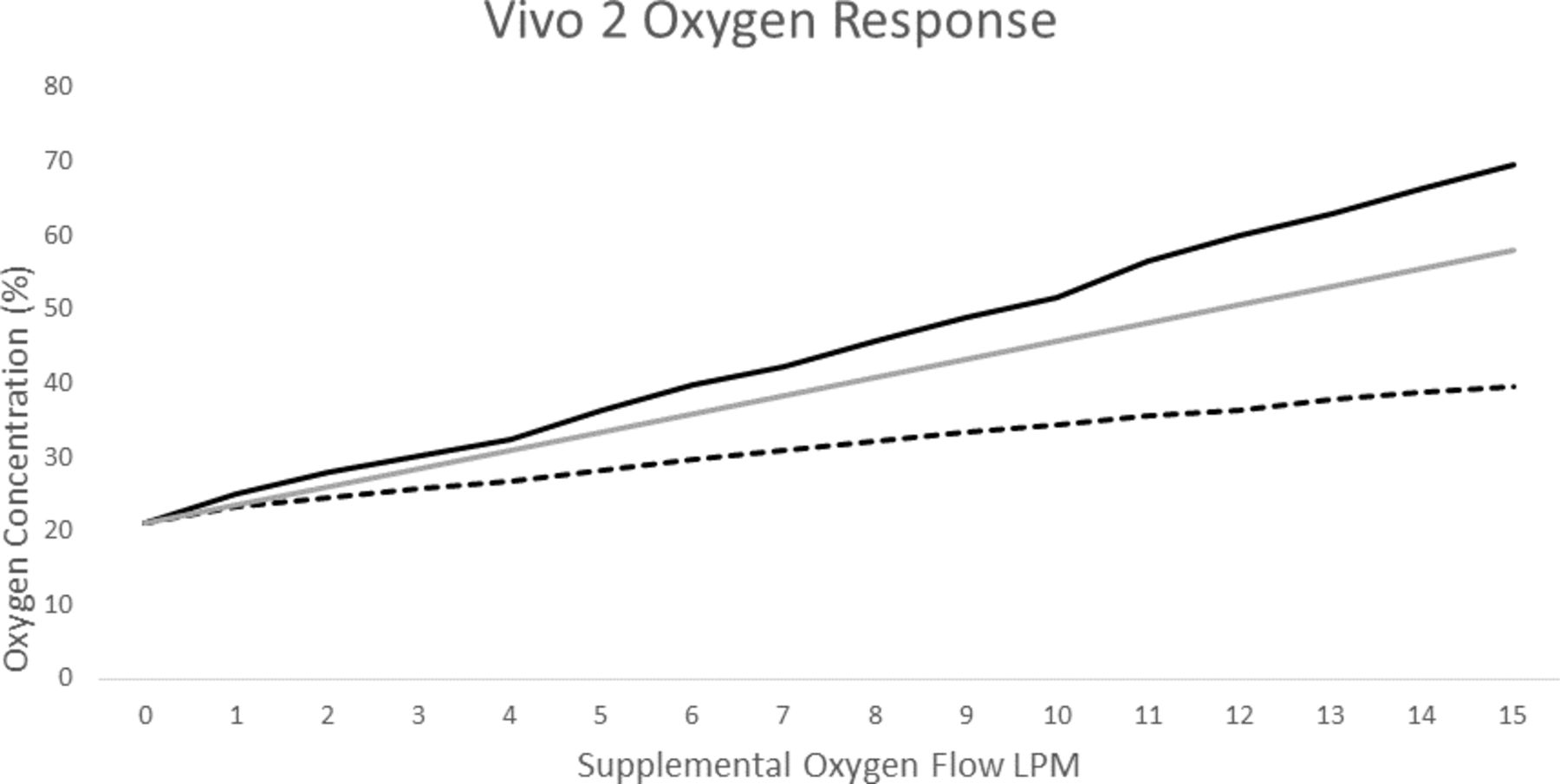
To capture the oxygen, which is normally vented to the atmosphere by the ventilator during the expiratory phase, it was necessary to design and 3D print an adaptor (figure 1), but the remaining components can be purchased from the catalogue of any appropriate medical consumables supplier. We tested a Breas Vivo 2 (Molnlycke, Sweden); this device has a dedicated oxygen inlet port which we used. Our modification resulted in increased FiO2 as shown in figure 2 compared with the performance deliverable under standard conditions of use. In particular, at a minute ventilation of 32 L/min, our modification increased FiO2 from 39.5% to 69.6%. Similarly, we investigated as an exemplar a ResMed Lumis 150 (Sydney, Australia). This device (like others from other manufacturers) does not have a dedicated O2 inlet. Here we designed and printed an adaptor for the air inlet to which the oxygen capture device was connected (Figure E1). With 15 L/min oxygen entrained, this modification increased FiO2 from 52% to 76.4% when used in timed pressure support mode at expiratory positive airway pressure 10 cm H2O and an inspiratory positive airway pressure of 30 cm H2O at 40 bpm, with Ti 0.7 s, with prescribed target volume at 750 mL and measured VE 30 L/min (figure 3). For both devices, the modification increased FIO2 over the entire range of supplemental oxygen used (figure 2).

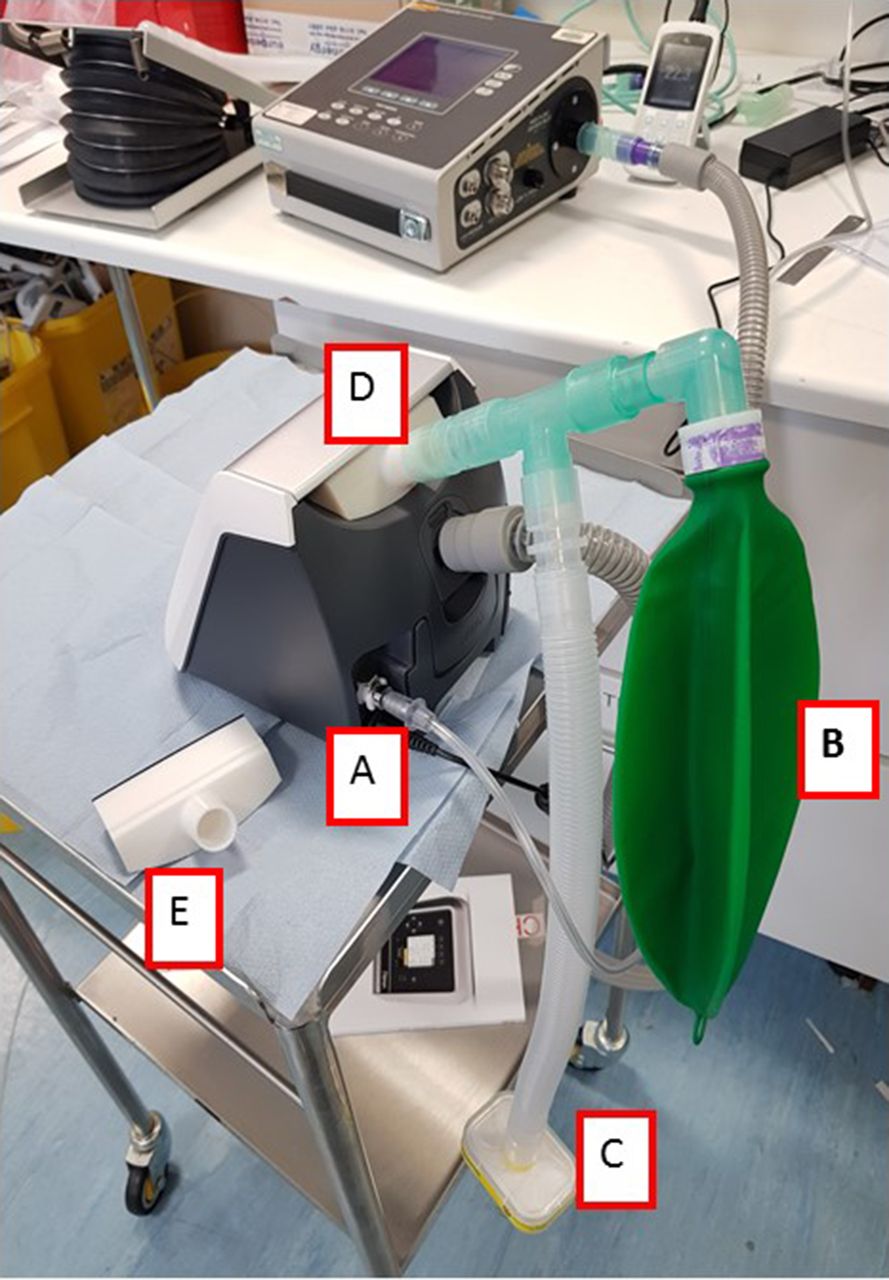
The vivo two with the manufactured inlet adaptor in situ. instruction files for doing so may be found at among the online supplemental file associated with this paper. The general evaluation apparatus may be seen in the background. A—oxygen inlet connected to wall oxygen at 15 L/min. B—reservoir for the capture of expiratory phase O2. C—T-piece allows ingress of room air (protected by a filter). D—air inlet contains 3D printed adapter. E—duplicate air inlet adaptor.
Supplemental material

Measured inspired FiO2 as a function of wall oxygen flow rate with vivo two in timed+target volume mode at EPAP 10 cm H2O and an IPAP permitted between 20 and 30 cm H2O at 40 bpm, with Ti 0.7 s. The prescribed target volume was 1000 mL but at this respiratory rate, typical tidal volume was ~800 mL and measured VE 32 L/min, in the normal use (dashed line) and with our modification (solid line). Calculated ideal data (assuming no leak and no dead space/rebreathing) from an intensive care ventilator are shown in grey. EPAP, expiratory positive airway pressure; IPAP, inspiratory positive airway pressure; LPM, litres per minute.
{kind=link}
{kind=link}
{kind=link}
Measured inspired FiO2 as a function of wall oxygen flow rate with Lumis 150 in timed pressure support mode at EPAP 10 cm H2O and an IPAP of 30 cm H2O at 40 bpm, with Ti 0.7 s. The prescribed target volume was 750 and measured VE 30 L/min, in the normal use (orange) and with our modification (blue). Calculated ideal data (assuming no leak and no dead space/rebreathing) from an intensive care ventilator are shown in grey. EPAP, expiratory positive airway pressure; IPAP, inspiratory positive airway pressure; LPM, litres per minute.
Even when modified our approach is inferior to devices designed for intensive care unit use. In particular, FiO2 cannot be accurately measured by the clinician who would have to rely on demonstrating adequate patient oxygenation. Second, the ‘blower’ in domiciliary ventilators is insufficient to cope with rapid variation in flow and thus the prescribed pressure is unlikely to be the received pressure throughout the inspiratory cycle. Third, this approach does not permit measurement of compliance or resistance or plateau pressure which is optimal for the management of acute lung injury. Fourth, in view of the urgency of COVID-19, we were unable to evaluate the safety of the materials used and thus whether they pose any long-term risk to health. Fifth, the adaptation (by intention) raises the amount of oxygen within the machine which could represent a fire hazard, given their electrical operation.
Nevertheless, the approach described resulted in a substantial increase in FiO2 delivered for any given level of supplementary oxygen and would in principle be applicable to other devices. This property could be of value for increasing the FiO2 delivered to any single patient; alternately by reducing the oxygen consumption of the entire hospital, it permits the treatment of more patients at any given FiO2 for the same total consumption of oxygen. This is of interest given media reports that some hospitals have run short of oxygen during the COVID-19 pandemic.
We stress that this is an off-label adaptation of these devices and that our work has been carried out entirely independent of their manufacturers, and without their approval. Moreover, as currently constituted, we believe this adaptation does not comply with the regulatory environment in our own country. We cannot, therefore, recommend clinicial use; however, the principal may be of interest both to ventilator designers or to clinicians operating in alternative regulatory environments, especially those with insufficient ventilators certified for ICU use or whose hospitals face pressures on their oxygen supply.
Supplemental material
Supplemental material
Acknowledgments
The authors would like to acknowledge the technical support we received from Robin Hardie, Farakh Aziz, Toby Kinsey, Bethany Wale and Royal Brompton Hospital Clinical Engineering teams and Respiratory Support teams.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YM and MIP equally contributed on all aspects of this work from conception, design, development to completion/reporting, and together produced the first draft of the manuscript. SP and IM helped with experimental data acquisition. PJ and RD-G helped with 3D design printing. DF, DA and RT, using their clinical experience of treating COVID patients, provided valuable conceptual insights which helped the develop the idea. All authors read and approved the final manuscript. The evolution of this idea stemmed from colleagues in NW London and in discussions with clinical colleagues (DF/RT/DA/MIP). Manufacturing and adapting the adaptation was undertaken by BME/innovation at RBHFT (YM/SP/IM/RD-G). The original idea was developed by YM. MIP produced the first draft of the MS and all authors have seen and approved the draft.
Funding This was supported by the Royal Brompton and Harefield NHS Trust and Brunel University London.
Disclaimer Although the design for the adaptors described in this article is provided free to users (see supplementary files 2 and 3), RBHFT and Imperial College have filed a patent application to protect the innovation which at least in theory could result in financial gain to the institutions in the future, although authors' principal current aim is to protect their ability to disseminate the method to health care providers who may wish to use it. Clinical use of this modification is entirely at the risk of the user. The authors and their institutions accept no responsibility for the consequences of clinical use.
Competing interests MIP serves as a paid consultant for Philips and JFD.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.