Article Text

Statistics from Altmetric.com
As the COVID-19 pandemic sweeps across the UK there remain issues with reverse-transcription polymerase chain reaction (RT-PCR), the gold standard diagnostic method. Delays in obtaining results have been particularly problematic. Some patients, including those with high clinical suspicion of COVID-19, test falsely negative on initial RT-PCR test, sometimes requiring multiple subsequent tests to return an eventual positive result. Suggested possible reasons for this include: suboptimal clinical sampling techniques; variations in viral load; and manufacturer test kit sensitivity.1 With surging caseloads, managing these RT-PCR ‘negative’ patients is proving hugely challenging.
An emerging bottleneck to effective care is dealing with isolation capacity. Inpatients who are truly PCR negative can be moved to a non-isolation ward, thereby freeing up isolation beds for COVID-19 positive patients and also reducing risk of nosocomial virus transmission. Patients with high index clinical suspicion of COVID-19, but who test negative on initial RT-PCR test, continue to be managed with respiratory isolation precautions, often undergoing repeat PCR testing. However, this means further delay while awaiting subsequent test results. Against this backdrop, an effective pathway to deal with negative COVID-19 RT-PCR results in the setting of high clinical probability is urgently needed.
A further important concern is developing regarding deisolation on patient discharge to either home or community care: a confirmed COVID-19 diagnosis - or confirmed alternative, non-COVID-19 diagnosis - is key to imparting advice to families and carers.
Imaging has been suggested as a potential solution to some of these problems. Most patients undergo chest radiograph (CXR) at presentation to hospital, with CXRs being hot-reported using a template classification system produced by British Society of Thoracic Imaging (BSTI).2 This stratifies patients into one of four groups based on CXR: COVID classic/probable; COVID indeterminate; COVID normal; and Non-COVID. Frontline doctors have found this a useful adjunct to clinical assessment.
In mainland China, CT was often a first-line investigation for COVID-19. However, such practice was burdensome on radiology departments and hugely challenging for infection control. CT in COVID-19 shows typical findings of ground glass opacity, peripheral consolidation or a combination of both. Ai et al reported CT sensitivity from their Wuhan cohort of 97% when compared with RT-PCR.3 When combined with the possibility for near instantaneous results, it is perhaps not surprising that CT has seen most widespread use in endemic regions of China, Italy and Iran. Some reports have also described typical CT findings consistent with COVID-19 in patients with initial negative RT-PCR who subsequently tested positive on repeat RT-PCR testing.3 4
Several authors5 and professional societies6 have steadfastly suggested that CT should not be used as a first line or pure diagnostic test – while highly sensitive, CT findings of COVID-19 pneumonia are not specific. In addition, false negative CT rates vary in the literature, ranging from 3%–56% in RT-PCR positive patients.7 CT features tend to peak later (day 6–11) in the disease course.8 Importantly, there are huge resource implications of this approach as the scanner requires decontamination each time a ‘positive’ patient is scanned. Radiographers risk repeated exposures to COVID-19, with high likelihood of illness and absence from work, at a time when healthcare workers are a precious resource. Finally, concerning reports from Italy suggest that over-reliance on CT potentially contributed to ‘dirty’ scanners acting as virus transmission vectors, thereby exacerbating COVID-19 spread among staff and COVID-19 naive patients.
We agree with Hope et al 5 that “…CT does not add diagnostic value” if used indiscriminately but would disagree that it has no role to play in diagnostic workup. They state “it is clear that the positive results can only be believed if the pre-test probability of disease is high.” This is supported by data from Wong et al where “in the scenario of high clinical suspicion of COVID-19 it is conceivable that a positive CXR can obviate the need for a CT”, thereby reducing burden on CT units during the COVID-19 pandemic.9
While awaiting the RT-PCR result, most suspected COVID-19 patients are clinically diagnosed with the triad of clinical assessment, CXR and blood tests. CT could however play a limited, but important, role in providing diagnostic radiological confirmation in patients with clinically suspected - but RT-PCR negative - disease. This would potentially help resolve whether a patient with suspected high clinical probability of COVID-19 has an alternative diagnosis in addition to influencing infection control strategy (namely the ability to stepdown a patient to a deisolation ward).
We have seen patients with negative RT-PCR at presentation with ‘classic/probable’2 changes on CXR and repeat RT-PCR which returns positive. However, there remain a small proportion of patients in whom multiple RT-PCRs are negative and whose CXRs are repeatedly ‘normal’ or ‘indeterminate’, although clinical suspicion remains high. These ‘high clinical probability’ patients are those unwell enough to be admitted to hospital and are not presumed to represent the complete spectrum of COVID-19 patients, most of whom have mild symptoms requiring self-isolation in the community.
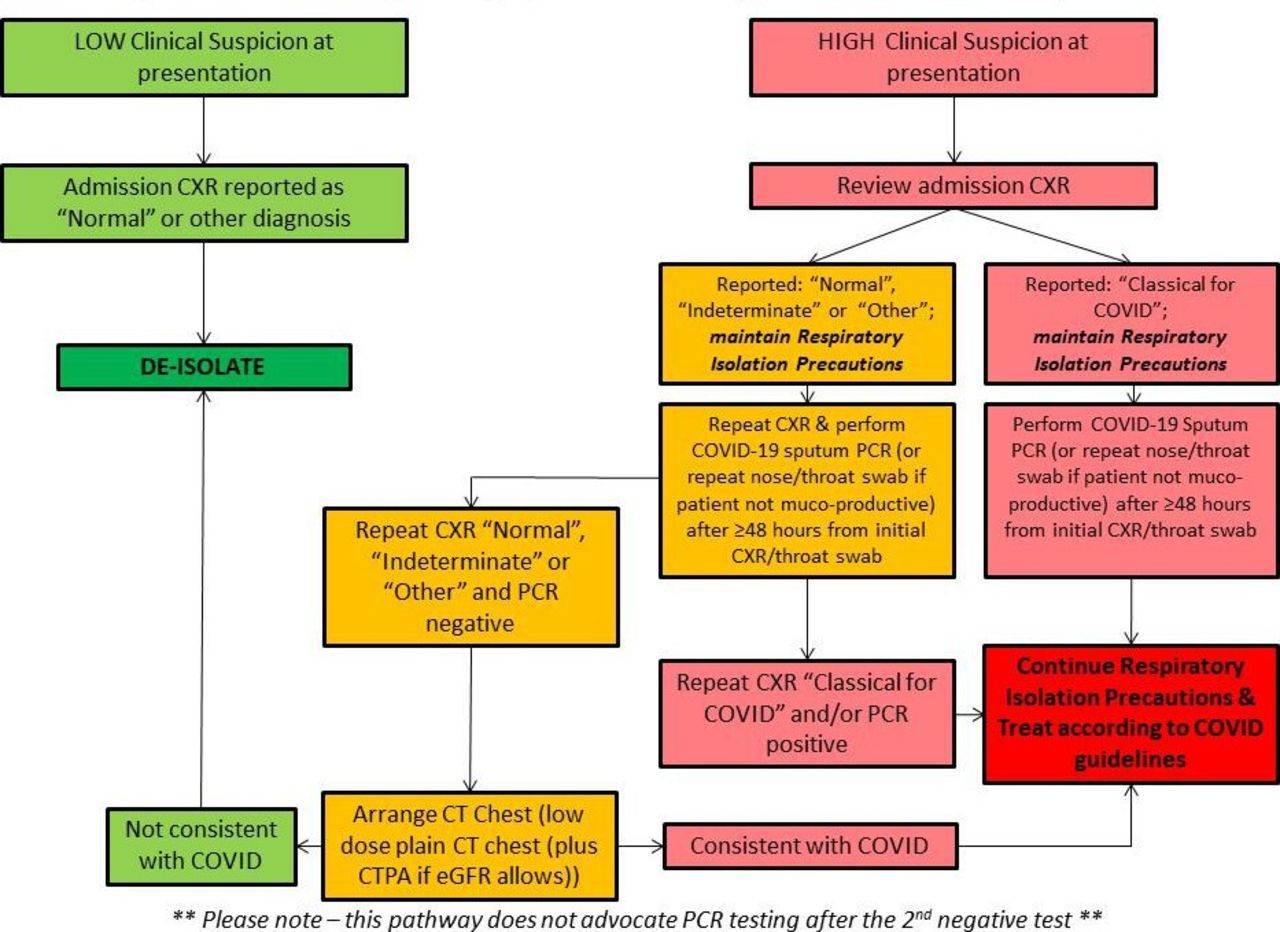
Our institution has thus devised a pragmatic protocol (figure 1), using CT to help diagnose this group of patients. Capacity for CT use in this limited way has been created as a result of cancelling elective/routine CT requests for other indications, thereby permitting not only rapid access to CT scanning but also allowing ample time for scanner terminal clean in between cases. In our algorithm, CT is performed in patients who return two negative RT-PCR swabs and two CXRs (≥48 hours apart) reported as ‘normal’ or ‘indeterminate’ for COVID-19 (‘double-double negative’). RT-PCR remains the lynchpin of diagnosis and, if negative, is repeated (usually around 48 hours after presentation). The rationale for repeat CXR in patients where the index CXR was not COVID-19 classic/probable is that several patients go on to develop COVID classic appearances, despite a normal/indeterminate index CXR, in the setting of high clinical probability.

{kind=link}
Proposed infection control management of inpatients with a negative initial COVID-19 nose/throat swab RT-PCR.
Patients who are deemed eligible for CT as per our protocol undergo a sequential low dose non-contrast CT thorax and CT pulmonary angiogram (if renal function allows).10 CTPA is performed to ensure occult PE is excluded, particularly in light of reports of increased pro-thrombotic risk in COVID-19. The non-contrast CT prior is performed for two main reasons: i) dependent ground glass is often exaggerated on post-contrast scan and can be mistaken for true ground glass; ii) having a baseline non-contrast scan can be useful if then performing subsequent unenhanced scans. The key to our pathway is thorough clinical assessment as pre-test probability determines how these patients are managed, above all else.
As the pandemic progresses it may be that so many cases ‘swamp’ the system that CT is forced to take a more upfront role in patient triage. At present with infection control such a key facet of patient management – as well as staff safety – the RFL NHS Trust negative PCR pathway enables a systematic approach to patient deisolation and stepdown from COVID ward to Non-COVID wards.
Footnotes
ANT and AB are joint first authors.
DDC and SSH are joint senior authors.
Twitter @lungdiagnosis
Contributors SH, DC and AK devised the pathway. AT, JB, HJ, SB and AB revised the pathway, AT, SH and DC wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves