Article Text

Abstract
The concept of chronic obstructive pulmonary disease (COPD) control has been proposed to guide treatment decisions in COPD. In this study, we aimed to validate the prospective value of this concept in the SPARK study population. Control was assessed based on COPD stability and impact. Patients with low impact and stability during weeks 1–12 were classified as controlled, and exacerbations were measured during a 52-week follow-up. Of the 2044 patients included a majority were non-controlled (80%), frequently due to high impact. During the follow-up, the rate of moderate/severe exacerbations was significantly lower in controlled patients (rate ratio, 0.56, 95% CI 0.48 to 0.65 p<0.0001) and time-to-first moderate/severe exacerbation was significantly delayed. This study demonstrated an association between control status and risk of exacerbations.
- COPD Exacerbations
Statistics from Altmetric.com
Introduction
Current recommendations for treatment of chronic obstructive pulmonary disease (COPD) are based on exacerbations, symptoms or clinical phenotypes.1–3 However, in the same severity group or phenotype, a patient may experience variation in symptoms, more frequent exacerbations or an impairment in health status that does not result in a change in category, and therefore, no step-up or step-down recommendation is established.
The concept of disease control has been well characterised in asthma. Physicians dispose of several evaluation tools, such as the Asthma Control Questionnaire, which allow to determine the level of control and subsequently to guide therapy in clinical practice.4 Recently, José Soler-Cataluña et al 5 6 proposed a definition to assess the concept of control in COPD based on impact of the disease and clinical stability. Impact is related to the manifestations of the disease and it is assessed by symptoms reported by the patient, or using a symptom questionnaire.7 8 Two previous studies have partially addressed the validation of control in COPD.9 10 However, prospective, follow-up studies are required to investigate the prognostic value of the concept of control.
In the present analysis, we aimed to assess the association of the proposed concept of COPD control on future exacerbations in a population of severe and very severe patients with COPD from the SPARK study population.11
Method
The SPARK study was a 64-week, double-blind, parallel-group multicentre study, which included patients with severe and very severe COPD between April 2010 and July 2012, with at least one moderate exacerbation the previous 12 months.11 Patients were randomised to receive tiotropium 18 µg, glycopyrronium 50 µg or a fixed-dose combination of indacaterol 110 µg and glycopyrronium 50 µg for 64 weeks.
In this post hoc analysis, we investigated the association of control status on future exacerbations. Control was defined based on impact and stability. The study was divided into two time periods: weeks 1–12 were used to assess control status, and a follow-up period of 52 weeks (weeks 13–64) to evaluate the predictive value of control (online supplementary figure 1).
Supplemental material
‘Low impact’ or ‘high impact’ was defined based on the assessment of dyspnoea and sputum colour from the electronic diary and use of rescue medication from the electronic case report form at the end of week 12. Patients were classified as high impact if they had any of dyspnoea ≥2, sputum colour 2–3 (yellow or green) or >2 puffs/day rescue medication use or as low impact if they did not fulfil any of the previous. Alternatively, impact could be assessed using the Saint George’s Respiratory Questionnaire (SGRQ) score (see online supplemental material and supplementary figure 3). Stability was defined as the absence of exacerbations during 12 weeks. Patients with low impact and no exacerbations during weeks 1–12 were classified as controlled and patients with high impact and/or an exacerbation during this period were classified as non-controlled. For the validation of the concept of control, rate of moderate/severe and all exacerbations; and time-to-first moderate/severe and all exacerbation were assessed during a follow-up. The statistical analysis is described in the online supplemental material
Supplemental material
Supplemental material
Results
A total of 2044 patients were included. At week 12, only 418 (20%) of patients were classified as controlled. Of the non-controlled patients, 1539 (95%) had high impact of COPD, being the major contributors dyspnoea (72.5%), sputum colour (22%) and use of rescue medication (75.6%). Overall, most patients (76%) were stable having no moderate/severe exacerbations during weeks 1–12. Among those classified as non-controlled, 25% fulfilled both high impact and instability (see online supplementary figure 2).
Supplemental material
Controlled patients had a slightly better lung function with less patients classified as very severe, were less frequently frequent exacerbators and less patients were treated with inhaled corticosteroids (ICS) at baseline. They also had significantly better health-related quality of life measured by the SGRQ and a lower COPD symptom score (table 1).
Demographic and clinical characteristics of patients based on control status
Control status and exacerbation events
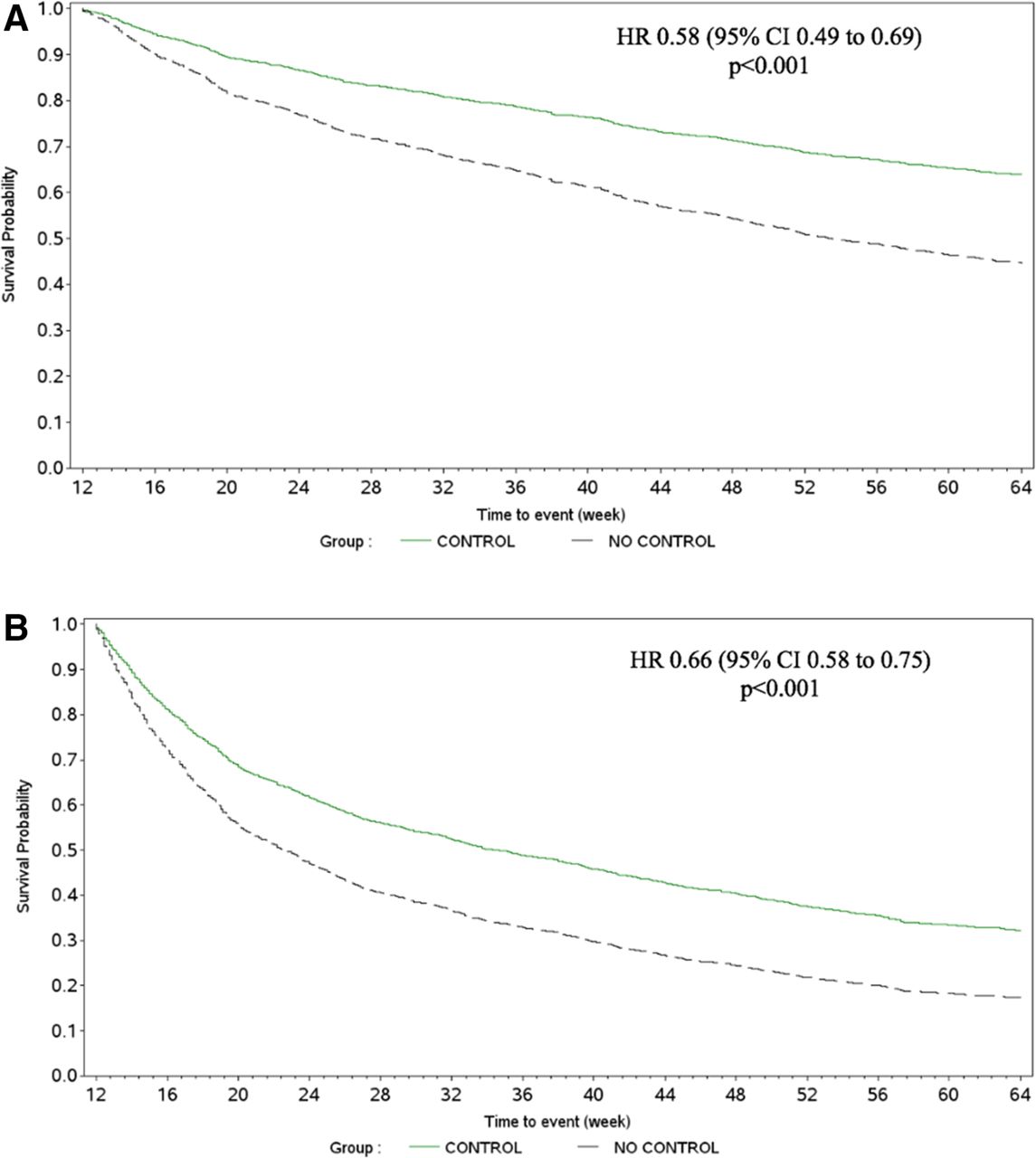
The rate of moderate/severe exacerbation events was significantly lower in the controlled group (annualised rate in controlled patients 0.54, 95% CI 0.43 to 0.69; annualised rate in non-controlled patients 0.98, 95% CI 0.81 to 1.18; rate ratio (RR), 0.56, 95% CI 0.48 to 0.65 p<0.0001). Time-to-first moderate/severe exacerbation was also significantly delayed in the controlled group (93 days (95% CI 84 to 102) for controlled, 222 days (95% CI 184 to 222) for non-controlled; HR (HR), 0.58, 95% CI 0.49 to 0.69 p<0.0001); because less than 50% of patients in the controlled group had an exacerbation, the time by which at least 25% of patients had a first to moderate/severe exacerbation was calculated instead of the median time. Similar trends were observed for all exacerbations with significantly lower rate (RR 0.71, 95% CI 0.63 to 0.80, p<0.0001) and delayed time-to-first exacerbation in the controlled versus the non-controlled group (172 (95% CI 114 to 219) vs 75 (95% CI 65 to 83) days, HR, 0.66, 95% CI 0.58 to 0.75 p<0.0001) (figure 1) (Adjusted by prior history of exacerbations and treatment, see online supplementary material for statistical analysis).
{kind=link}
Kaplan-Meier plot of time-to-first (A) moderate/severe exacerbation and (B) all (mild, moderate and severe) exacerbation in controlled and non-controlled patients during 52 weeks† adjusted by prior exacerbations and treatment. †Control status was based on clinical variables in the e-diary/eCRF. eCRF, electronic case report form; e-diary, electronic diary.
Discussion
Our results showed that a low number of patients could be classified as ‘controlled’ using impact and stability with the proposed thresholds as indicators of control status. Among the different criteria proposed, having a high impact of the disease was the most frequent cause for being classified as non-controlled. Time-to-first exacerbation was found to be significantly delayed and exacerbation rate was lower in patients who were classified as controlled, therefore, indicating that evaluation of control status has prognostic implications.
We have evaluated the prognostic value of the concept of control previously developed by Soler-Cataluña et al.6 This concept was proposed to monitor the state of the disease in patients with COPD, and thus to help in optimising pharmacological and non-pharmacological treatment in daily clinical practice. The applicability of control has already been assessed in cross-sectional and database studies. Nibber et al 9 aimed to validate the definition of control in the OPCRD. The authors used the proposed definition to retrospectively assess the status of control during a period of 3 months, followed by a 12-month follow-up. In this cohort, 90% of patients had mild-to-moderate COPD and within this group only 4.5% of patients were defined as controlled, while no severe-to-very severe patients were identified as controlled. Time-to-first exacerbation was longer for the controlled patients with mild-to-moderate COPD, therefore, demonstrating the association between control status and exacerbations.
More recently, a cross-sectional analysis of control status from an international, prospective study of a cohort of 314 patients with COPD has been reported.10 In this cohort, up to 21% of the individuals were classified as controlled, all having mild-to-moderate disease. Two-thirds of the patients did not fulfil control criteria due to the high impact of the disease, being high dyspnoea score and low physical activity the most common reasons. The results of both studies reflected that the criteria or thresholds selected to define control were too restrictive. The number of severe/very severe patients was low in both studies and none of them was considered controlled based on the criteria used. Besides, the study design did not allow validating the concept of control as predictor of future outcomes.
In accordance with the previous studies, we observed that the majority of COPD individuals in the SPARK population did not fulfil the criteria for control, and most of them were classified as non-controlled due to high impact of the disease. The rate of exacerbations was lower in the controlled group during 1-year follow-up. Time-to-first exacerbation was also significantly delayed (for all exacerbations and for moderate/severe exacerbations) in patients who were controlled.
We observed that controlled patients, although less frequently, still presented exacerbations during follow-up. In COPD, it may be difficult to reach absolute control with the current therapies, and there is not a defined intermediate stage level of control.12
This study has some limitations that need to be acknowledged. The design of the study limited inclusion and assessment only to patients with severe and very severe COPD, and therefore, these results cannot be extrapolated to less severe patients with COPD. Validation of these findings in a prospective study including a broader spectrum of COPD patients would help to support the thresholds evaluated here and serve as additional proof for the predictive utility of control status. Despite these limitations, the large study sample size and the availability of high-quality data from 1-year follow-up support the suitability of the SPARK study population to test the concept of control.
In conclusion, these findings support the utility of the concept of clinical control as a predictor of future risk of exacerbations and, moreover, as a tool to guide treatment intensity in patients with COPD. Future prospective studies may confirm this prognostic value in populations of less severe COPD.
Acknowledgments
The authors thank Paul McKiernan of Novartis Ireland, Dublin and Archana Jayaraman (PhD), and Santanu Bhadra of Novartis Healthcare, Hyderabad, India for providing writing support in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). The authors would like to thank Pritam Gupta for his support on the statistical analysis of this manuscript. MB is the recipient of an Rio Hortega contract in the 2017 Strategic Action Health Call from the Instituto de Salud Carlos III for the years 2018–2019.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Juanjosoler5
Contributors MB, KK, KM, BA, JJJJS-C, MM and JAW contributed to study design. KK, KM, SS and JAW were responsible for planning and conducting the study. SS, KK, KM,MM and JAW performed and/or supervised data analysis. MB was responsiblefor drafting the manuscript. All authors contributed to data interpretationand to development of the final manuscript. MM and JAW take responsibilityfor the integrity of the data and the accuracy of the data analysis.
Funding This analysis has been funded by Novartis Pharma AG, Basel, Switzerland.
Competing interests MB has received speaker fees from Menarini, GlaxoSmithKline, Gebro Pharma, Boehringer Ingelheim, CSL Behring and Grifols and consulting fees from Novartis. KK is an employee and shareholder of Novartis Pharma AG, Basel, Switzerland. KM is an employee of Novartis Pharma AG, Basel, Switzerland. SS is an employee and shareholder of Novartis Pharmaceuticals, New Jersey, USA. BA reports personal fees and grants from Novartis AG, personal fees from Boehringer Ingelheim, personal fees from GSK, personal fees from AstraZeneca, grants and personal fees from Menarini, outside the submitted work. JJJJS-C has received speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Esteve, Ferrer, GSK, Menarini, Novartis, and Pfizer, and consulting fees from AirLiquide, Boehringer Ingelheim, Chiesi, GSK, AstraZeneca, Ferrer and Novartis. MM has received speaker fees from Astra Zeneca, Boehringer Ingelheim, Chiesi, Cipla, Menarini, Rovi, Bial, Grifols and Novartis, consulting fees from Astra Zeneca, Ferrer, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Bial, Gebro Pharma, CSL Behring, Laboratorios Esteve, Mereo Biopharma, Verona Pharma, pH Pharma, Novartis and Grifols and research grants from GlaxoSmithKline and Grifols, outside the submitted work. JAW reports grants from GSK, Johnson and Johnson, Novartis, Boehringer Ingelheim, Astra Zeneca, outside the submitted work.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves