Article Text

Abstract
We developed a MRI protocol using transverse (T2) and longitudinal (T1) mapping sequences to characterise lung structural changes in preterm infants with bronchopulmonary dysplasia (BPD). We prospectively enrolled 61 infants to perform 3-Tesla MRI of the lung in quiet sleep. Statistical analysis was performed using logistic Group Lasso regression and logistic regression. Increased lung T2 relaxation time and decreased lung T1 relaxation time indicated BPD yielding an area under the curve (AUC) of 0.80. Results were confirmed in an independent study cohort (AUC 0.75) and mirrored by lung function testing, indicating the high potential for MRI in future BPD diagnostics.
Trial registration DRKS00004600.
- paediatric lung disaese
Statistics from Altmetric.com
Introduction
Bronchopulmonary dysplasia (BPD), notable for its significant long-term sequelae, affects up to 50% of very low birthweight infants worldwide. Clinically defined by the need for oxygen supplementation or ventilator support at term, specific diagnostic tools for the assessment of structural pulmonary changes are missing. Our aim was to identify and validate reliable imaging markers indicating BPD with high sensitivity using transverse (T2) and longitudinal (T1) mapping strategies in a newly developed MRI protocol.
Methods
Study population
Sixty-one very preterm infants with a gestational age (GA) ≤32 weeks (online supplementary table S1) were prospectively included in the study on informed parental consent (exploration cohort n=40, Perinatal Centre LMU Munich, EC #195–07; confirmation cohort n=21, Perinatal Centre UKGM Giessen, EC #135/12). BPD (mild, moderate and severe) was diagnosed at 36 weeks GA.1
Supplemental material
MRI protocol and analysis
Lung MRI was performed at 36 weeks GA in spontaneously breathing infants (fractional inspired oxygen (FiO2)=0.21) using a 3-Tesla whole-body scanner. The protocol included pulse sequences for assessment of morphology, volume and quantitative relaxation parameters: (i) ECG-triggered T2-weighted single-shot fast spin echo (ssFSE) sequences in three orthogonal orientations (echo time (TE): 57 ms; repetition time (TR): 2 RR intervals), (ii) single-slice ssFSE T2 mapping (TR 2000 ms, 4 TEs 26–92 ms) and T1 mapping (TR/TE 3000 ms/26 ms, six inversion times TI (slice-selective): 25–2600 ms and no inversion) acquiring eight averages (total acquisition time ≈5 min).
For T2-mapping/T1-mapping analysis, manual segmentation into four lung quadrants was performed (Osirix MD). T2 and T1 relaxation times were calculated by non-linear exponential signal fitting for four lung quadrants separately and the total lung.
ILFT
Standardised ILFT (tidal breathing analysis, passive respiratory mechanics, functional residual capacity (FRCp)) was performed at 36 weeks GA according to the guidelines of the American Thoracic and European Respiratory Society in spontaneously breathing infants (FiO2=0.21) under light sedation (chloral hydrate, 30–40 mg/kg; orally).
Statistics
Missing values were imputed by sampling from a normal distribution (sample mean and SD) and accounting for the covariance structure of the highly correlated MRI variables. To model binary disease outcomes, BPD was dichotomised (no vs mild/moderate/severe BPD; no/mild vs moderate/severe BPD). A Grouped Lasso Logistic model was used to estimate the impact of different variables on the outcome BPD; independent variables included GA, gender, weight, steroids, early onset infection and imaging data.
The Grouped Lasso Logistic model was repeated using lung function and imaging data as independent variables. Quality of the models was assessed by leave-one-out cross-validation for unbiased validation avoiding overoptimistic AUC for model validation.
Model validation was realised in an independent study cohort calculating ROC and AUC by comparing predicted results with true output. Confirmation of the results was obtained using logistic regression (no vs mild/moderate/severe BPD) under consideration of the confounders GA, gender, steroids and early infection. Methods are detailed in the online supplementary S1-S4.
Results
Quantification of structural changes in the BPD lung by MRI relaxation times
By regularised linear modelling, we identified quantitative MRI parameters associated with the diagnosis of BPD in premature infants near term. With significant clustering of regional values, total lung values are presented (online supplementary figure S1).
Supplemental material
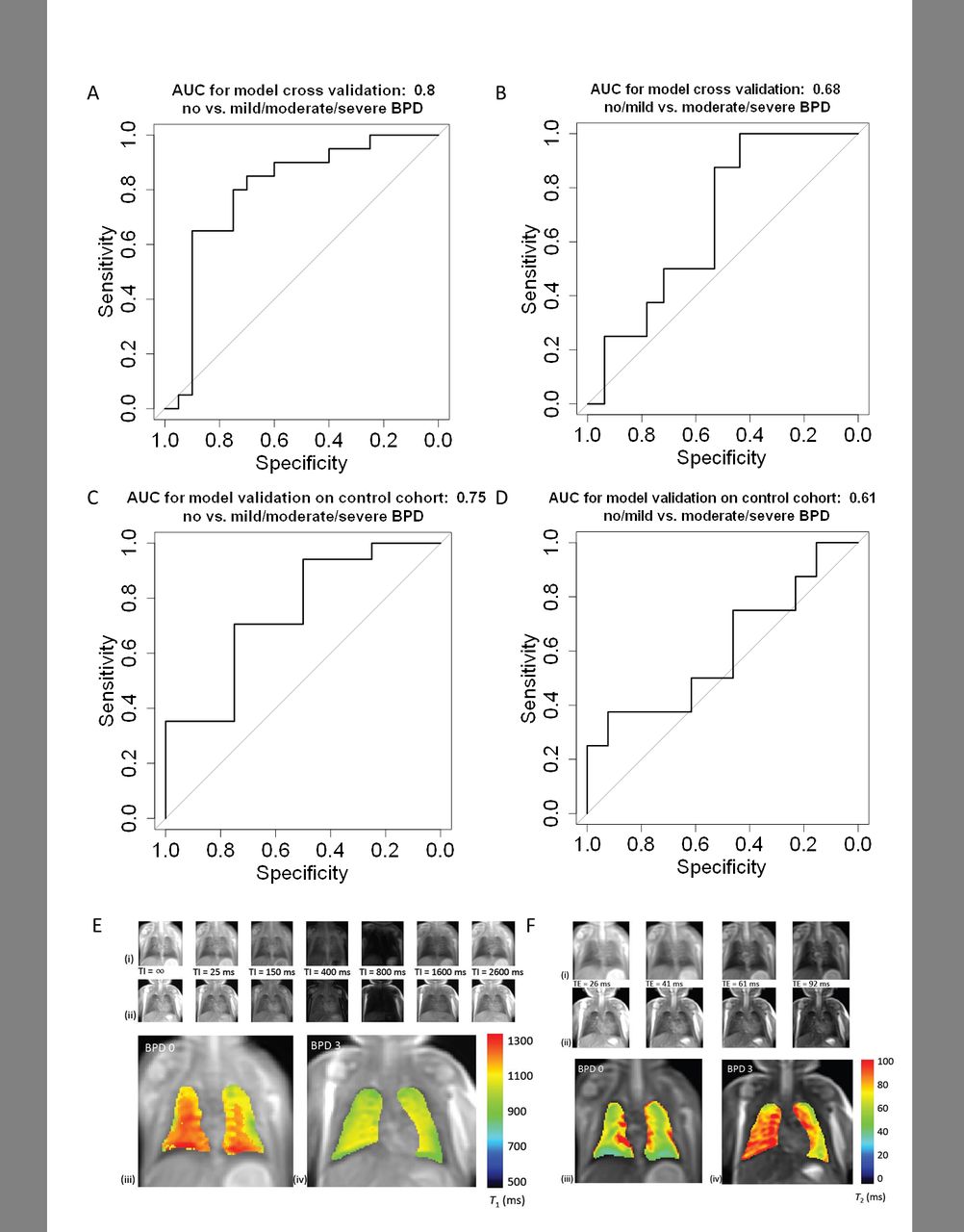
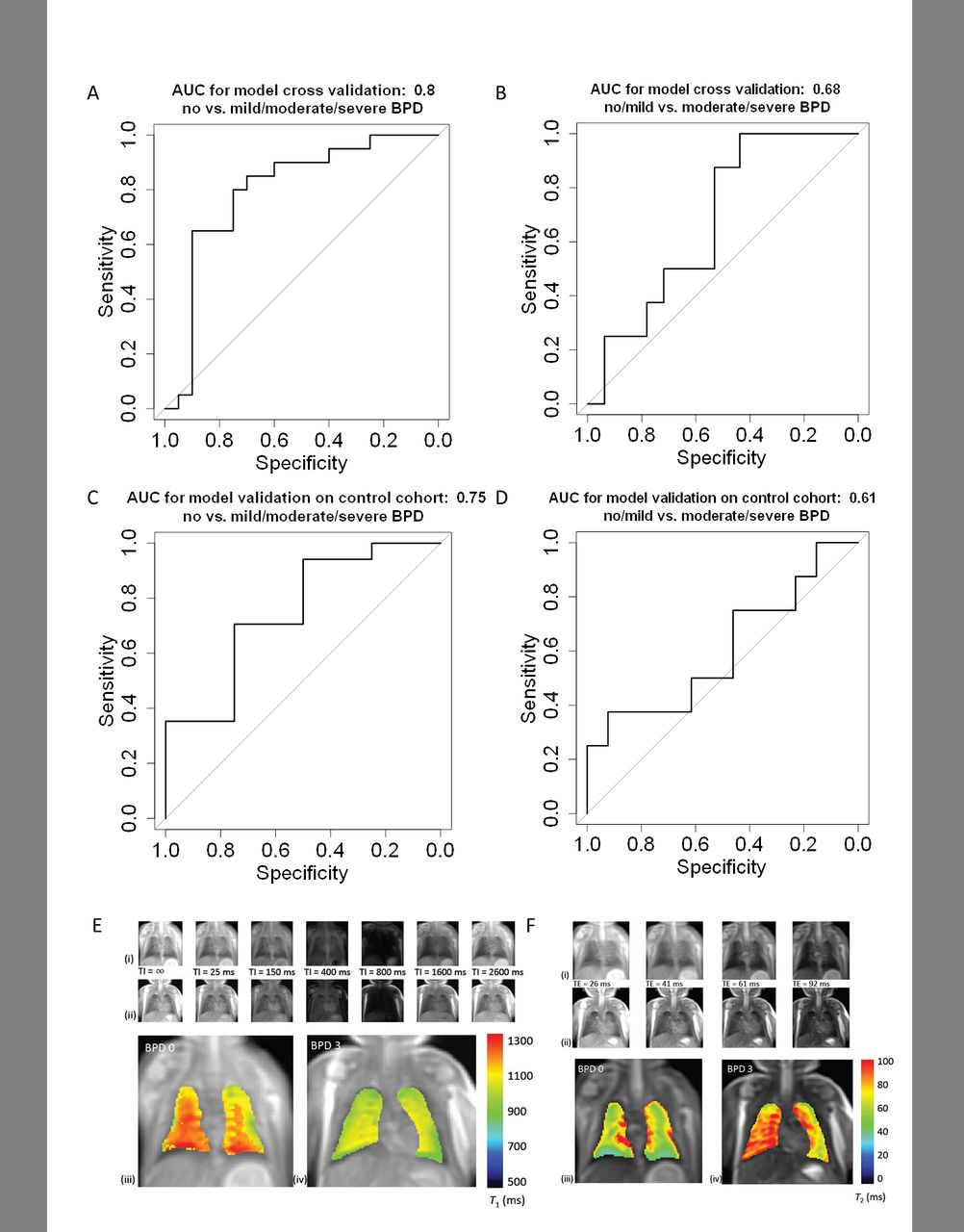
Increased lung T2 relaxation time and decreased lung T1 relaxation time are associated with an overall increased risk for BPD (mild, moderate and severe BPD vs no BPD, T2: β=0.037 (OR 1.038); T1: β=−0.0001 (OR 1)) as well as an increased risk for higher disease grades (moderate and severe BPD vs no or mild BPD, T2: β=0.007 (OR 1.007); T1: β=−0.003 (OR 0.997)) (table 1, figure 1). Leave-one-out cross-validation yielded an AUC of 0.8 (0.65–0.95) (mild, moderate, severe BPD vs no BPD) and an AUC of 0.68 (0.49–0.86) (moderate/severe BPD vs no/mild BPD) (figure 1), respectively. The variable GA showed significant impact on the study results.
{kind=link}
Leave-one-out cross-validation for the logistic imaging model with an area under the receiver operating characteristic (ROC) of 0.8 (0.65–0.95) (mild, moderate and severe bronchopulmonary dysplasia (BPD) vs no BPD (A)) and an area under the ROC of 0.68 (0.49–0.86) (moderate/severe BPD vs no/mild BPD (B)). Confirmation of the cross validation by the logistic imaging model for BPD in an independent study cohort with an area under the ROC of 0.75 (0.44–1) (mild, moderate and severe BPD vs no BPD (C)) and an area under the ROC of 0.61 (0.33–0.99) (moderate/severe BPD vs no/mild BPD (D)). (E) Representative T1-weighted MR images (i, ii) without inversion pulse (TI=∞) and inversion times (TI) between 25 and 2600 ms. Calculated T1 maps of two subjects with BPD 0 (iii) and BPD 3 (iv). T1 relaxation time is decreased in severe BPD. (F) Representative T2-weighted MR images (i, ii) with echo times (TE) between 26 and 92 ms and calculated T2 maps in BPD 0 (iii) and BPD 3 (iv). T2 relaxation time is increased in severe BPD.
Coefficients logistic group LASSO model
We confirmed the findings using logistic regression showing a significant, positive association of T2 relaxation times with BPD (mild, moderate and severe BPD vs no BPD, β=0.137, OR 1.147; p=0.044)). The regression models including GA, gender, steroids, early infection and T2 and T1 relaxation times as covariables revealed an AUC of 0.85 (0.71–0.98) (mild, moderate and severe BPD vs no BPD) and an AUC of 0.59 (0.32–0.85) (moderate/severe BPD vs no/mild BPD), respectively.
A logistic imaging model confirmed the results in an independent study cohort (AUC 0.75 (0.44–1) (mild, moderate and severe BPD vs no BPD); AUC 0.61 (0.33–0.88) (moderate/severe BPD vs no/mild BPD)) (figure 1). Furthermore, replacement of the primary outcome BPD in the logistic regression analysis by the count variables ‘days of oxygen’ or ‘days of mechanical ventilation’ (birth to discharge) confirmed the results obtained by the grouped Lasso Logistic model (online supplementary figure S2 and S3).
Structural abnormalities correlate with functional and long-term effects
The Grouped Lasso model selected the variables FRCp (β=0.003; 95% CI 0 to 0.15), compliance (Crs/kg) (β=−0.09; 95% CI −1.85 to 0) and tidal volume (VT/kg) (β=−0.05; 95% CI −0.71 to 0) together with T1 (β=−0.002; 95% CI −0.04 to 0) and T2 relaxation times (β=0.002; 95% CI −0.13 to 0.12) as predictors for the outcome variable BPD. In addition, infants with the need for home monitoring showed significantly higher T2 relaxation times when compared with preterms discharged without a device (p=0.04). Detailed results are provided in the online supplementary figure S4 and S5.
Discussion
By the use of a comprehensive MRI protocol in non-sedated, spontaneously breathing infants, we identified quantitative imaging markers with high sensitivity for BPD at term-equivalent age. Namely, increased T2-relaxation time and decreased T1-relaxation time were revealed to indicate BPD and to identify higher disease grades by Lasso-Model, confirmed by logistic regression analysis.
Functional data obtained by ILFT and confirmation of the findings using count variables,2 that is, ‘days of oxygen’, days of MV’ underlined the validity of the results.
T2 and T1 relaxation times are two of the most widely used tissue parameters for image contrast in MRI, their quantification allowing for objective MRI analysis.3 Higher lung T2 relaxation times in preterm infants with BPD may indicate increased interstitial remodelling, that is, fibrosis, potentially associated with pulmonary inflammation and interstitial oedema, recently described for adult patients with lung disease.4–6 Shortened T1 relaxation times potentially indicate emphysematous changes or relative changes in pulmonary perfusion.7 8 The blood concentration of dissolved molecular oxygen can also influence pulmonary T1 relaxation times with oxygen acting as a (weak) paramagnetic contrast agent. The imaging findings thereby reflect characteristic histological changes described for BPD,9 in line with the follow-up data indicating decreased pulmonary stability in infants with abnormal imaging findings as indicated by the need for home monitoring.
In summary, the use of an advanced, quantifiable mapping technique strongly supports the value of MRI lung imaging in preterm infants with BPD, significantly adding to recent findings obtained by a small-footprint 1.5-Tesla scanner using commercially available sequences in neonates after birth.10 The use of a newly developed protocol in a larger number of patients as well as a confirmation cohort underscore the importance of our findings, next to the application of complex statistical modelling that allowed us to account for disease complexity and the multitude of confounders with significant correlation.
Our results hint at possible mechanisms of BPD pathology (and pathogenesis) and provide a step towards improved imaging-based phenotyping in BPD with increased diagnostic accuracy, proven to be critical for personalised treatment strategies and disease monitoring. Future studies will need to join forces between different perinatal centres in order to allow for the identification of disease subtypes and long-term outcome while increasing patient numbers when studying this unique patient cohort with high-end imaging techniques.
Acknowledgments
We thank the AIRR study patients and their families as well as our study nurse, Sonja Dull, or their contribution.
Footnotes
Contributors BEW, HE and AH contributed to the conception and design. KF, HE, AWF, CH and OD contributed to acquiring data. KF, BEW, HB, SS, AP, LN, OD and AH contributed to analysis and interpretation. KF, BEW, HB, SS, AS, OE, FT, OD and AH contributed to the drafting of the manuscript for important intellectual content.
Funding NWG VH-NG-829 (Helmholtz Association), German Center for Lung Research (Federal Ministry of Science).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.