Article Text

Abstract
We performed a prospective, observational, cohort study of children newly diagnosed with children’s interstitial lung disease (ChILD), with structured follow-up at 4, 8, 12 weeks and 6 and 12 months. 127 children, median age 0.9 (IQR 0.3–7.9) years had dyspnoea (68%, 69/102), tachypnoea (75%, 77/103) and low oxygen saturation (SpO2) median 92% (IQR 88–96). Death (n=20, 16%) was the most common in those <6 months of age with SpO2<94% and developmental/surfactant disorders. We report for the first time that ChILD survivors improved multiple clinical parameters within 8–12 weeks of diagnosis. These data can inform family discussions and support clinical trial measurements.
- Interstitial lung disease in Children
- mortality
- ventilation
- oxygen saturation
Statistics from Altmetric.com
Introduction
Interstitial lung disease in children (ChILD) encompasses more than 200 entities,1 many so rare that there is no reported prospective longitudinal disease phenotyping.2 Recent improvements in adult interstitial lung disease phenotyping has led to better disease management. We aimed to use the first international collaboration for ChILD to systematically study new diagnoses for 12 months, to better understand disease progression and support the development of clinical outcomes.
Methods
This was an observational cohort study of children (<18 years) presenting to participating hospitals with a new clinical presentation of ChILD, submitted to the ChILD-EU Registry (http://www.childeu.net) between December 2013 and March 2016.3 Cases were registered following brief screening questions and were subject to multidisciplinary peer review to standardise diagnostic precision.3 Common causes of diffuse lung disease (ie, cystic fibrosis, respiratory distress syndrome) were excluded. There were 133 incident cases during this period. Six were excluded from analysis, leaving 127 reported here (1 time from diagnosis too great, 2 airway disease, 1 pleural disease, 2 insufficient data). The enrolment date (baseline data) was the study start date. Study variables were collected at baseline, 4, 8, 12 weeks and 6 and 12 months (end of the study) and included patient demographics, initial diagnoses, family and neonatal history, current history and symptoms, physical examination findings, Fan score,4 laboratory results and treatments trialled and current (see study protocol (https://www.ed.ac.uk/usher/edinburgh-clinical-trials/our-studies/ukcrc-studies/child-eu) and ChILDEU website (http://www.childeu.net) for study variables and standardisation standard operating procedures).5 6 Biobank materials included (where available) chest radiology (CT), genetic mutation analysis and lung biopsy. Investigation and treatment recommendations were standardised.7 Ethical and legal approvals and were present in all recruiting centres. Fully informed parental consent was obtained prior to study inclusion. Comparison of continuous variable was by Mann-Whitney test (where only two categories that is, dead/alive) or Kruskal-Wallis test (>two categories that is, baseline oxygen levels). Missing SpO2 values were imputed (see online supplementary methods). Height, weight and body mass index were converted to Centre for Disease Control z-scores and percentiles.8 FEV1 and FVC were converted into Global Lung Initiative z-scores and percentiles.9 The trial is registered on clinical trials (https://clinicaltrials.gov/ct2/show/NCT02852928).
Supplemental material
Results
Participants were from nine European countries, predominantly Germany, UK and Poland (online supplementary table 1). The proportion of participants providing follow-up data (or dead) at each time point ranged from 76%–83% (online supplementary table 2). Median age at baseline was 0.9 (IQR 0.3–7.9) years (online supplementary table 1). Peer review diagnosis, investigations and treatments are provided in supplementary information (online supplementary tables 3–5). At baseline, dyspnoea (68%, 69/102) and tachypnoea (75%, 77/103) were frequent, with failure to thrive in 49% (61/125) common (online supplementary table 6). Baseline SpO2 in room air ≤94% was recorded in 53% (65/122) at a median 92% (IQR 88–96). Lower baseline SpO2 was most common in younger infants related to growth, developmental or surfactant related disorders (online supplementary table 3, figure 1).

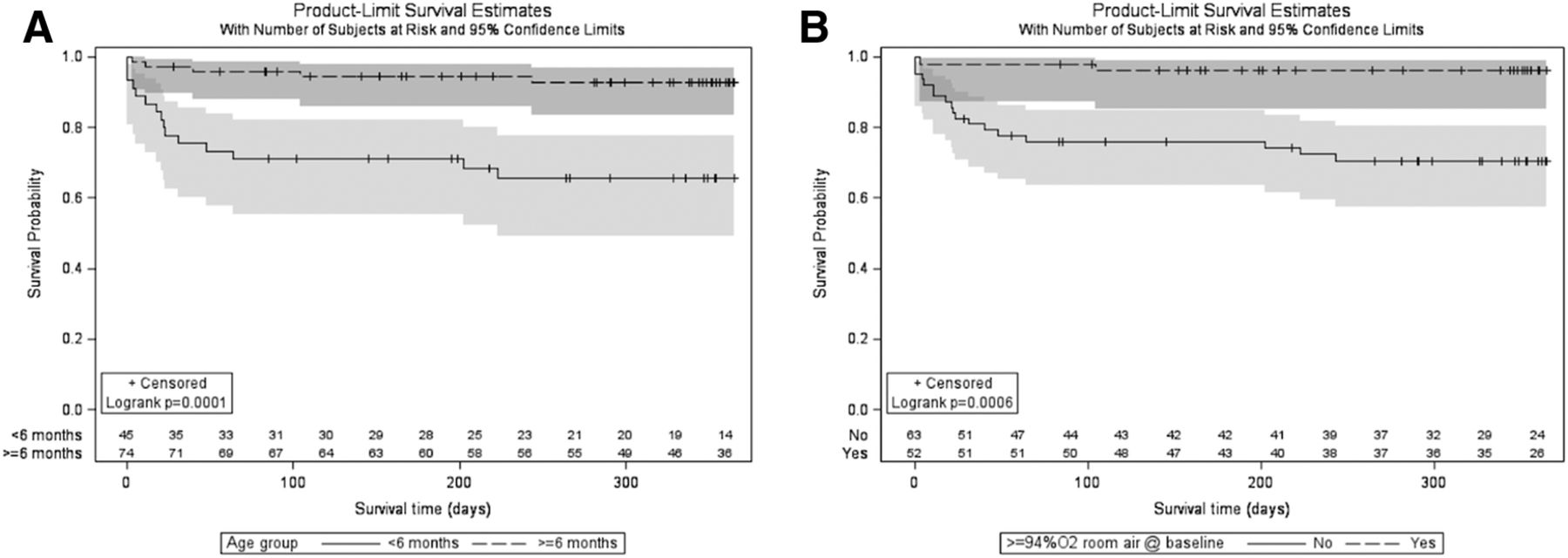
Survival by Kaplan Meier for (A) age < or ≥6 months, (B) baseline room air SpO2< or ≥94%.
Deaths, clinical support and physiology by study visit
There were 20 deaths (16%) over 12 months. Age at death, time from enrolment to death and diagnostic group are provided in online supplementary table 3. Most deaths occurred in diffuse developmental disorders (n=6), alveolar surfactant disorders (n=6) and lung growth abnormalities (n=3). Age at baseline was significantly associated with survival, with deaths in 33% (15/45) of those <6 months of age compared with 7% (5/74) in those ≥6 months of age (log-rank statistic, p=0.0001) (figure 1A). SpO2 at baseline ≥94% was associated with better survival (4% died: 2/52), compared with 29% (18/63) of those with SpO2<94%, (p=0.0006) (figure 1B).
Over 12 months, ventilatory support was used in 49 (39%) children, decreasing steeply over time with improvement or death (table 1). Of the 31 children ventilated at baseline, 15 died (11 invasive, 4 non-invasive ventilation). Supplemental oxygen was provided to 72% (92/127) at any point from baseline to 12 months. The percentage of children in follow-up recorded as receiving oxygen supplementation declined most markedly from baseline (63%, 74/117) to 12 week observations (31%, 23/74). For 33 children (26%), SpO2 in air was never ≥94%, mostly in those who subsequently died or were aged <6 months of age at baseline (table 1). Most improvement in SpO2 in air was observed in the first 8 weeks following enrolment (online supplementary figures 1A,B and 3).
There was a progressive reduction over time in Fan scores (figure 2 and online supplementary figure 1C), predominantly in the first 12 weeks, but continuing up to 12 months (online supplementary figure 4), with deaths more frequent at higher baseline scores (5 (36%, 8/22) and 4 (23%, 9/40)).

{kind=link}
{kind=link}
Change of Fan score over observation period (numbers in bars represent number in each group).
Weight for age at baseline was low and remained so at 12 months (online supplementary table 7). Most improvements in weight and height occurred in the first 4 weeks, with slower gains thereafter. Lower weight and height z-score at baseline was significantly associated with lower baseline SpO2 and death (online supplementary figure 5).
Median respiratory rate tended to be higher than age related reference values10 at baseline but similar to age-adjusted reference values by 12 months. Median heart rate was similar to age related reference values across observations10 (online supplementary figure 6A–D).
Improvement in FEV1 % predicted and z score continued up to 12 weeks, with little subsequent change (table 1). FVC had a more progressive change over the 12-month observation period, again most marked in the first 12 weeks (FVC % predicted median 48% to 65% and to 80% by 12 months). At baseline 19/25 (76%) spirometry demonstrated a restrictive (FEV1/FVC≥0.8) and 6/25 (24%) an obstructive pattern (ratio<0.8).
Systemic corticosteroids were provided to 58% (73/125), hydroxychloroquine 28% (35/126) and azithromycin 36% (45/126) of cases over the observation period (online supplementary information).
Discussion
We report that many clinical parameters appeared to improve within 8–12 weeks of diagnosis and starting treatment in children with ChILD. To our knowledge, this is the first prospective, longitudinal, cohort assessment of ChILD. At 12 weeks, when compared with baseline, provision of oxygen supplementation was observed in 31% fewer children, and lung function was 29% greater for FVC and 24% for FEV1. Mean Fan scores were 29% lower at 12 weeks. Differences in respiratory rate (and heart rate) across timepoints when related to normative data were not observed to have notable differences. We did not, however, provide a formal longitudinal analysis and this together with missing data may have impacted the results. We also acknowledge potential bias may have occurred from the effect of funding limitations on recruitment in some EU countries and translation of study materials. In summary, we have identified key parameters responsive to change in ChILD which could be used in trials of treatment and inform prognostic discussions with families. Furthermore, we suggest that patients with ChILD should be seen more frequently in the first 3 months following diagnosis, so treatment can be adjusted with any clinical improvement.
Acknowledgments
This work is a collaboration of European Respiratory Society Clinical Research Collaboration for Children’s Interstitial Lung Disease (CRC-2015-02), COST Action EnterChILD (CA16125) and KidsLungRegister chILD-EU Register.
Footnotes
Collaborators Dr Jayesh Bhatt, Nottingham Children’s Hospital, UK; Dr Frederik Buchvald, Copenhagen University Hospital, Denmark; Dr Nazan Cobanoglu, Ankara University, Turkey; Dr Fran Child, Royal Children’s Hospital, Manchester, UK; Dr Nwokoro Chinedu, Royal London Hospital, UK; Dr Leonard Donato, Colmar, Civil, Strasbourg, France; Ralph Epaud, INSERM 955 - Equipe 5, Paris, France Dr Ampara Escribano, Valencia, Neumologia Inf, Spain Dr Achim Freihorst, Aalen, Ostalb Klinikum, Germany; Dr Atul Gupta, King’s College Hospital, London, UK; Dr Emma Guy, Leeds General Infirmary, UK; Dr Tobias Hübner, Oldenburg, Zentr. Kind-Jugend, Germany; Dr Petra Kaiser-Labusch, Bremen, Klin. Bremen-Mitte, Germany; Dr Christiane Lex, Göttingen University, Germany; Dr Sarah Mayell, Royal Liverpool Children’s Hospital, UK; Dr Samantha Moss, Royal Victoria Infirmary, Newcastle, UK; Dr Nagehan Emiralioglu, Ankara, Hacettepe University, Turkey; Dr Lutz Nährlich, Giessen, Germany; Dr Nadia Nathan, Hôpital Trousseau, Paris, France; Dr Ruth O’Reilly, Sheffield Children’s Hospital, UK; Dr Nicolas Regamey, Luzern, Kinderspital, Switzerland; Dr Isabelle Rochat, Lausanne, Switzerland; Dr Martin Rosewich, Frankfurt/Main, JWG University, Germany; Dr Tugbu Sismanlar, Ankara, Gazi University, Turkey; Dr Deborah Snijders, Padua University, Italy; Dr Florian Stehling, Essen, University, Germany.
Contributors Chief investigator of ChILDEU project: MG. Principle investigator observational study: SC. Developed protocol: SC, CG, MM, ABa, ACle, NK, KKro, AB, NS and MG. Peer review team: PA, MA, ACal, JLZ, AN, SR, TW, AB, NS and MG. Data preparation: JC, MH, KK, KKro, JL and MW. Analysis: SC and CG. Analysis review: AB, NS and MG. Final draft: SC, CG, MM, PA, MA, ABa, ACal, JC, ACle, MH, BK, KKat, NK, KKro, JL, JLZ, AN, SR, TW, MW, AB, NS and MG.
Funding The project was funded by the European Union’s Seventh Framework Program under grant agreement n°305653—child-EU.
Disclaimer The funders had no role in the writing of the manuscript or the decision to submit it for publication.
Competing interests SC and VS report other from Boehringer Ingelheim, outside the submitted work; MG reports other from Vertex and Boehringer Ingelheim, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.