Article Text

Abstract
Long-term exposure to particulate matter 2.5 μm (PM2.5) air pollution is associated with an increased risk of lung cancer. However, the evidence is limited in low-income and middle-income countries. We estimated the association between the incidence of lung cancer and PM2.5 air pollution exposure in the Urban Employee Basic Medical Insurance (UEBMI) beneficiaries in China. A total of 16 483 new lung cancer cases diagnosed from 12 966 137 UEBMI beneficiaries from 36 cities between 2013 and 2016. The relative risk for lung cancer associated with a 10 µg/m3 increase in 3-year PM2.5 exposure was 1.12 (95% CI 1.00 to 1.26). The population attributable risk estimated for a reduction in PM2.5 concentration to 35 µg/m3 corresponded to a decrease of 14% in cases of lung cancer. Reducing PM2.5 air pollution has a significant public health benefit.
- lung cancer
Statistics from Altmetric.com
Introduction
Air pollution has a wide-ranging and deleterious effect on human health, and constitutes a major public health concern for global communities.1 In China, lung cancer is both the most commonly diagnosed cancer and the leading cause of cancer-related deaths, with 781 000 new cases diagnosed each year.2 Studies involving large cohorts have shown the relationship between long-term exposure to particulate matter 2.5 μm (PM2.5) and incidence of lung cancer, but few studies have been conducted in low-income and middle-income countries with a large population and high air pollution level.3
We conducted a study using a random 5% sample of China Urban Employee Basic Medical Insurance (UEBMI) beneficiaries who were enrolled between 2013 and 2016. We hypothesised that participants exposed to higher PM2.5 concentrations would be at a higher risk of lung cancer compared with participants exposed to a lower PM2.5.
Methods
We obtained a random 5% sample of UEBMI beneficiaries from 01 January 2010 to 31 December 2016, using systematic sampling with a random start. City-level age-standardised rates of lung cancer were standardised to Sixth National Census in 2010 and expressed as a rate per 100 000 persons per year. Annual average concentration of PM2.5 from 1998 to 2016 were estimated, using a neural network model that incorporated aerosol optical depth (AOD), land use and meteorological variables.
We estimated relative risks (RRs) and CIs for the incidence rates of lung cancer with 10 µg/m3 increase in PM2.5 exposure using weighted logistic regression model, the lung cancer incidence rate was used as weight variable. We also modelled PM2.5 air pollution using restricted cubic splines to evaluate the non-linear concentration-response relationship between PM2.5 air pollution and lung cancer.
See online supplementary file S1 for more detailed information on study method.
Supplemental material
Results
A total of 16 483 lung cancer cases were diagnosed from 12 966 137 UEBMI beneficiaries from 36 cities between 2013 and 2016. The mean age of lung cancer patients was 63.7 years (SD 12.2 years), and 34.0% of them were women in 2016 (table 1). The annual nationwide average PM2.5 concentration ranged from 30.5 to 48.9 µg/m3 between 1998 and 2016 (online supplementary figure S1). The age-standardised incidence rates (ASRs) of lung cancer standardised to Sixth National Census in 2010 were 105, 110, 107 and 118 per 100 000 from 2013 to 2016, respectively. The ASRs peaked for beneficiaries aged from 60 to 74 years (153 per 100 000) (online supplementary table S1). The city-specific incidence rate of lung cancer is presented in online supplementary table S2.
Basic characteristics and lung cancer rate of the random 5% sample of Urban Employee Basic Medical Insurance beneficiaries, 2013–2016
In the fully adjusted model, the RR (95% CI) for lung cancer associated with a 10 µg/m3 increase in 1-year, 3-year, 5-year and 10-year PM2.5 exposure was 1.09 (95% CI 0.98 to 1.21), 1.12 (95% CI 1.00 to 1.26), 1.11 (95% CI 0.98 to 1.26) and 1.11 (95% CI 0.98 to 1.26), respectively (table 2). For all exposure periods, the magnitude of the RRs increased in the areas with high PM2.5 exposure (≥35 µg/m3). The population attributable risk estimated for a reduction in PM2.5 concentration to 35 µg/m3 corresponded to a decrease of 14.02 (95% CI 11.76 to 16.27) in cases of lung cancer, with a prevalence of high air pollution exposure (≥35 µg/m3) of 81%.
Risk ratios of lung cancer associated with an increase of 10 µg/m3 in PM2.5 in the random 5% sample of Urban Employee Basic Medical Insurance beneficiaries*
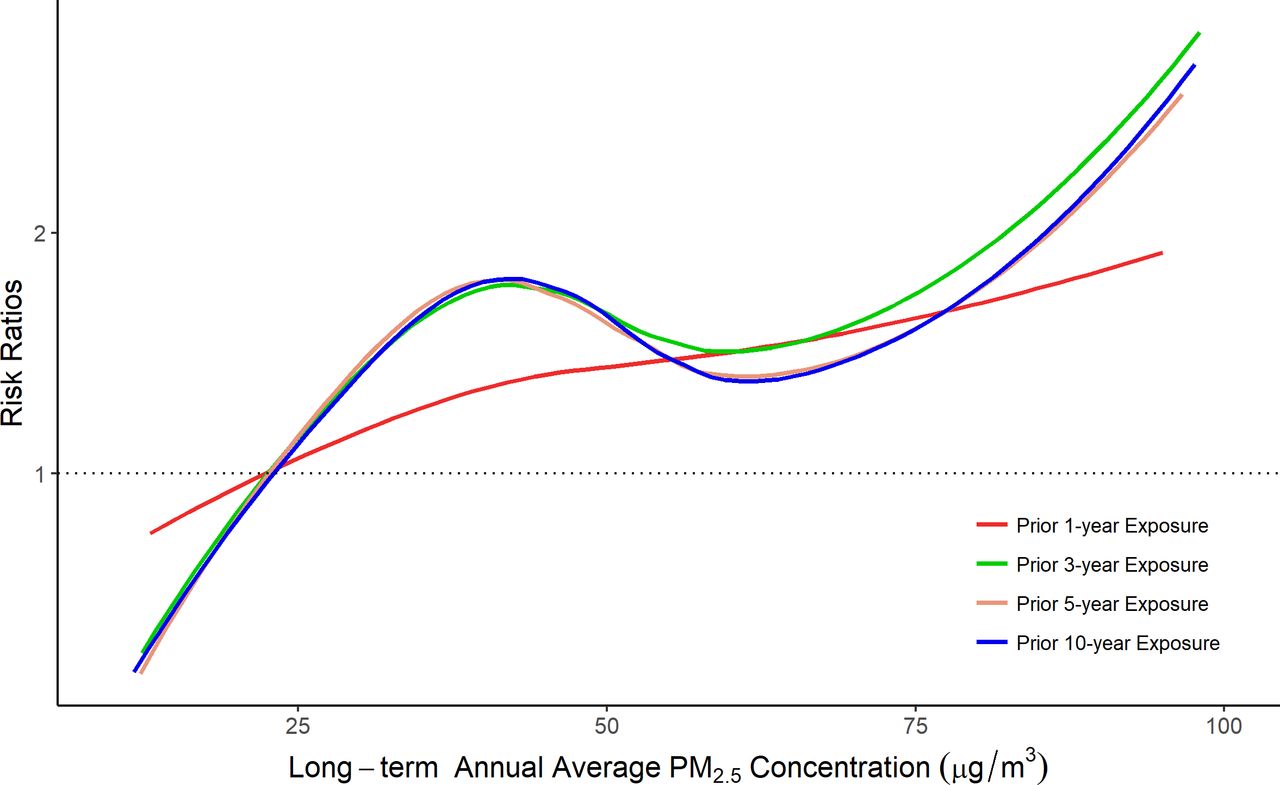
In spline regression analyses, the incidence rate of lung cancer increased with increasing 1-year, 3-year, 5-year and 10-year cumulative average PM2.5 throughout most of the distribution of PM2.5 concentrations (figure 1).
{kind=link}
Risk ratios for lung cancer associated with a 10 µg/m3 increase in PM2.5 concentration by difference exposure periods. Risk ratios were adjusted for calendar time, region and smoking rate. The dose-response curve was calculated using restricted cubic splines with knots at the 5th, 35th, 65th and 95th percentiles of the distribution of PM2.5 concentrations. The reference exposure level was set at the 10th percentile of the distribution of 1-year PM2.5 concentration (23.0 µg/m3), 3-year PM2.5 concentration (24.0 µg/m3), 5-year PM2.5 concentration (24.2 µg/m3) and 10-year PM2.5 concentration (24.5 µg/m3). PM2.5, particulate matter 2.5 μm.
Discussion
In this UEBMI population, there is an increased risk of lung cancer associated with increasing long-term PM2.5 air pollution exposure. These findings add to the limited number of studies showing this association in low-income and middle-income countries.
A growing number of cohort studies have found evidence for the association between long-term PM2.5 exposure and incidence of lung cancer. The European Study of Cohorts for Air Pollution Effects (ESCAPE), Nurses’ Health Study and a Canadian population-based case-control study found positive associations between long-term PM2.5 exposure and incidence of lung cancer, with each 10 µg/m3 increment in PM2.5 associated with HRs of 1.40 (95% CI 0.92 to 2.13), 1.06 (95% CI 0.91 to 1.25) and 1.29 (95% CI 0.95 to 1.76), respectively.4–6 Few studies have conducted in low-income and middle-income countries. A study conducted in China reported that the RR of lung cancer incidence associated with a 10 µg/m3 increase in PM2.5 concentrations was 1.09 (95% CI 1.08 to 1.10).3 Our finding was consistent with prior studies; however, the associations were remarkable stronger when restricted to areas with higher pollution levels, which indicated the non-linear association between PM2.5 exposure and incidence of lung cancer.
The mechanism underlying the relationship between PM2.5 exposure and lung cancer is uncertain. Ambient air pollution has been classified as a carcinogen and may affect cancer development via the well-described pathways, including inflammation, oxidative stress, DNA damage, cell proliferation or epigenetic modification.1
Our findings should be interpreted considering some limitations. Because of the aggregate nature of ecological studies, our study is prone to ecological fallacy and confounding. We did not have data to distinguish the newly diagnosed lung cancer cases from the existing lung cancer cases. To address this, we excluded patients who filed a lung cancer claim between 2010 and 2012; however, we could potentially have included existing lung cancer cases in this analysis. As an additional limitation, we did not have data on population migration and neighbourhood-level socioeconomic status, which could potentially contribute to confounding or measurement error that could bias the estimated association between air pollution exposure and incidence of lung cancer.7 The lower proportion of study subjects under 45 years limited the generalisability of our findings.
China has begun to implement and improve measures to reduce air pollution since 2013, and incremental success has been observed.8 Additional studies are needed to evaluate the effects of the decreased air pollution on the incidence of lung cancer.
In conclusion, long-term PM2.5 air pollution exposure increases the risk of lung cancer among China UEBMI beneficiaries. Reducing PM2.5 air pollution would provide a strong public health benefit.
Acknowledgments
Thanks to Carol Resnick for the language editing of this article.
Footnotes
XS and PH are joint senior authors.
ZZ and DZ contributed equally.
Funding This work was supported by the Peking University’s Start-up Fund (BMU2018YJ004)
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was deemed as exempt from ethical approval by the institutional review board of the Beijing University of Chinese medicine (No.2019BZHYLL0201).
Provenance and peer review Not commissioned; externally peer reviewed.